Article Text

Abstract
Objective Impairment of mental well-being (anxiety, depression, stress) is common among people with multiple sclerosis (PwMS). Treatment options are limited, particularly for anxiety. The aim of this study was to update our previous systematic review (2014) and evaluate via meta-analysis the efficacy of mindfulness-based interventions (MBIs) for improving mental well-being in PwMS.
Methods Systematic searches for eligible randomised controlled trials (RCTs) were carried out in seven major databases (November 2017, July 2018), using medical subject headings and key words. Studies were screened, data extracted, quality appraised and analysed by two independent reviewers, using predefined criteria. Study quality was assessed using the Cochrane Collaboration risk of bias tool. Mental well-being was the primary outcome. Random effects model meta-analysis was performed, with effect size reported as standardised mean difference (SMD).
Results Twelve RCTs including 744 PwMS were eligible for inclusion in the systematic review, eight had data extractable for meta-analysis; n=635. Ethnicity, socioeconomic status, comorbidity and disability were inconsistently reported. MBIs varied from manualised to tailored versions, lasting 6–9 weeks, delivered individually and via groups, both in person and online. Overall SMD for mental well-being (eight studies) was 0.40 (0.28–0.53), p<0.01, I2=28%; against active comparators only (three studies) SMD was 0.17 (0.01–0.32), p<0.05, I2 =0%. Only three adverse events were reported.
Conclusions MBIs are effective at improving mental well-being in PwMS. More research is needed regarding optimal delivery method, cost-effectiveness and comparative-effectiveness.
PROSPERO registration number CRD42018093171.
- multiple sclerosis
- meta-analysis
- randomised trials
- stress
- depression
Statistics from Altmetric.com
Background
People with multiple sclerosis (PwMS) often describe the condition as stressful.1 Mental health comorbidity is common;2 anxiety and depression three times as frequent compared with population norms2 and are associated with higher levels of somatic symptoms, increased suicidality, lower quality of life and greater social problems.3
Very little evidence exists on the optimal treatment for impaired mental well-being in PwMS. Systematic review and meta-analytic evidence supports cognitive behavioural therapy (CBT) for both stress and depression in PwMS, but effective treatments for anxiety are lacking.4 5
Mindfulness-based interventions (MBIs) are complex interventions6 increasingly used in healthcare. MBIs have high quality evidence for treating stress, anxiety and recurrent depression in the general population7 and thus might also help PwMS with impaired mental well-being. In 2014, our previous systematic review found preliminary evidence from two randomised controlled trials (RCTs) and a controlled trial to support MBIs as a potential treatment for anxiety and depression in PwMS.8 Due to heterogeneity between study type, populations, interventions and outcomes, meta-analysis was not possible, nor was the optimal MBI for PwMS clear. Since 2014 several more RCTs have been published.
The aim of this review is to undertake a meta-analysis of RCT evidence for MBIs in improving mental well-being in people with MS.
Methods
Eligibility for inclusion
Based on the Study design, Participants, Interventions, Outcomes (SPIO) model (a derivative of Population, Intervention, Comparator, Outcome, Study [PICOS]),9 eligibility included: RCTs of patients with any diagnosis of MS, aged=/>18, any type of MBI (including core components of mindful breath awareness, body awareness and mindful movement), with outcomes focused primarily on impact on mental well-being.
Search strategy
We used our previous systematic review search strategy in: MEDLINE, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, AMED and PsycInfo. The ‘years’ delimiter was 2000–2018; our previous systematic review found the first study in this area was in 2000. We also searched ProQuest Dissertations & Theses Database, reference lists from key papers, contacted relevant experts and searched the grey literature. The initial search was in November 2017, updated in July 2018. Online supplementary file 1 contains the search strategy formatted for MEDLINE.
Supplemental material
Study selection, storage and screening
Search results were first imported into COVIDENCE, a systematic review data storage software package. Two independent reviewers (RS, SS) screened study title/abstracts for potential eligibility using keywords like ‘mindfulness’ and ‘multiple sclerosis’ (MS). Selected studies were then assessed further by two independent reviewers (RS, JB) against SPIO criteria to determine definitively eligibility. A third-party senior reviewer adjudicated any disagreements (SM).
Data collection/data items
Once the final list of studies for inclusion was agreed, data was extracted and expanded to ensure all Consolidated Standards of Reporting Trials (CONSORT)10 and Template for Intervention Description and Replication (TIDieR)11 checklist items were included (online supplementary file 2).
Supplemental material
Quality appraisal
The Cochrane Collaboration’s assessment tool12 was used to summarise the risk of bias for major outcomes in selected studies for individual outcomes, graded as high, unclear or low risk, assessing sequence generation, allocation concealment, participant blinding, personnel and outcome assessor blinding, completeness of outcome data, selective outcome reporting and any other sources of bias. Overall risk of bias for each study was also graded as:
Low=low risk of bias for all key domains
Unclear=low or unclear risk of bias for all key domains
High=high risk of bias for one or more key domains.
Principal summary measures
The ‘Primary outcome’ was identified as mental well-being (anxiety±depression±stress). The main outcome measure was taken as the last follow-up at which data were reported for that outcome. All main outcome measures were reported as continuous measures and their mean, SD and number of subjects for each treatment group were extracted. The unbiased standardised mean difference (SMD) was calculated, whereby a positive SMD reflects a difference in favour of MBI. Where papers reported effect estimates from adjusted regression models, these were extracted as the SMD.
Synthesis of results
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)13 guidance. Due to the wide variety of outcome measures identified and known heterogeneity, random-effects meta-analysis regression model14 was used to derive SMD. Estimates are reported along with their corresponding 95% CI and p values. The I2 statistic was used to assess the variability between studies.15 I2 describes the percentage of total variability in the estimates effect size that is attributable to heterogeneity. I2 varies from 0% (all heterogeneity is due to sampling error) to 100% (all variability due to true heterogeneity between studies)
Funnel plots and Egger’s Test for asymmetry were undertaken to test for publication bias and ‘trim and fill’ method was undertaken to assess the impact of the bias.16–19
All statistical analyses were carried out in R V.3.4.0 and using the meta package.20
Results
Twelve RCTs were identified as eligible for inclusion in the systematic review.21–32 However, only eight studies reported endpoint data that could be included in the meta-analysis.21–24 28–30 32 (figure 1). Further details were sought from study authors,29 31 32 but only one32 responded.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Study characteristics
Five studies took place in Iran,23 25–27 29 three in the UK,22 28 31 two in Italy,24 32 one each in Switzerland30 and the USA.21 Six studies reported assessing a MBI against usual care,22 23 28–31 in three this was not specified,22–24 while three used an active comparator (psychoeducation control).21 24 32 Six studies were powered.21 23 24 29 30 32 Sample sizes ranged from 24 to 150 (median 49). Eight studies measured outcomes at three time points (baseline, post MBI and at follow-up; range 1 month–1 year),21 22 24 28–32 while four were pre–post measurements only.23 25–27 (table 1).
Study characteristics
Participant characteristics
Across the 12 RCTs, the total number of participants was 744, those in the meta-analysis 635. Three studies reported ethnicity,21 22 28 mostly Caucasian. Overall, 76% (n=565) of study participants were female. Where reported, overall mean age of participants was 41.4 years (age not reported in one study26). Only two studies included details on socioeconomic status (SES),22 25 three minimal details on employment status.22 24 31 Ten studies included details on education status,21–23 25–30 32 with the majority in nine studies21–23 25–30 32 having completed at least school level education. Most (at least 447 or 60%) had relapsing-remitting MS, at least 112 (15%) had secondary progressive MS and at least 30 (4%) had primary progressive MS. Mean Expanded Disability Status Scale (EDSS) was reported in five studies,21 22 24 28 30 ranging from 2.3 to 6.5. Only one study reported on number of comorbid conditions (mean 2.3, SD 1.7),22 with four studies reporting on the active use of disease modifying drugs and/or psychotropic medications21 22 30 32 (table 2).
Participant characteristics
Intervention characteristics
Five studies used mindfulness-based stress reduction (MBSR),21 22 29 30 32 two based on MBSR,24 27 three mindfulness-based cognitive therapy (MBCT),25 26 28 one mindfulness-integrated CBT (MiCBT)23 and one mindfulness of movement.31 Six studies reported on participant materials.22 23 27 28 31 32 Three studies required a personal intake interview to take part,26 27 30 two sought baseline evidence of impaired mental well-being.21 28 Eight studies reported session content,21–23 25–29 three gave minimal description,30–32 one referred to the study protocol.24 Seven studies described home practices.21–24 28 30 31 Seven studies reported teacher characteristics,21–24 28–30 but in two detail was minimal.23 29 Eleven studies delivered group MBIs,21–30 32 one was individual.31 Two studies used online MBIs.28 32 Four studies reported intervention delivery location.22 28 29 32 Three studies had nine MBI sessions,21 24 30 eight had eight,22 23 25–29 32 one had six.31 Session length ranged from 1 to 3 hours. Class sizes ranged from five to 25, either one or two instructors present. Six studies modified the MBI for PwMS,22 24 28 30–32 one study during the course,22 simplifying mindful movement. Seven studies monitored treatment adherence (session attendance±home practice),21 22 25 28 30–32 four considered fidelity assessment,22 25 28 32 two recording/checking sessions.25 28 Ten studies delivered core MBI components.21–25 27–31 One study removed mindful movement.28 Three included an MBSR day retreat at week six.21 24 30 (For TIDieR checklist items, see online supplementary file 3.)
Supplemental material
Outcome characteristics
Eleven studies measured MBI effect on anxiety,21–26 28–31 eleven on depression,21–26 28–31 six on stress.21–24 28 29 One assessed likely cost-effectiveness, finding 87% probability of savings on service costs and improved outcomes.28 Three studies reported mean daily home practice (32, 29.2, 32.5 min22 30 31); another median (38 min/day; range 14–8021). Study attrition ranged from 0% to 39%.
Meta-analysis
Effect of MBIs on mental well-being measures
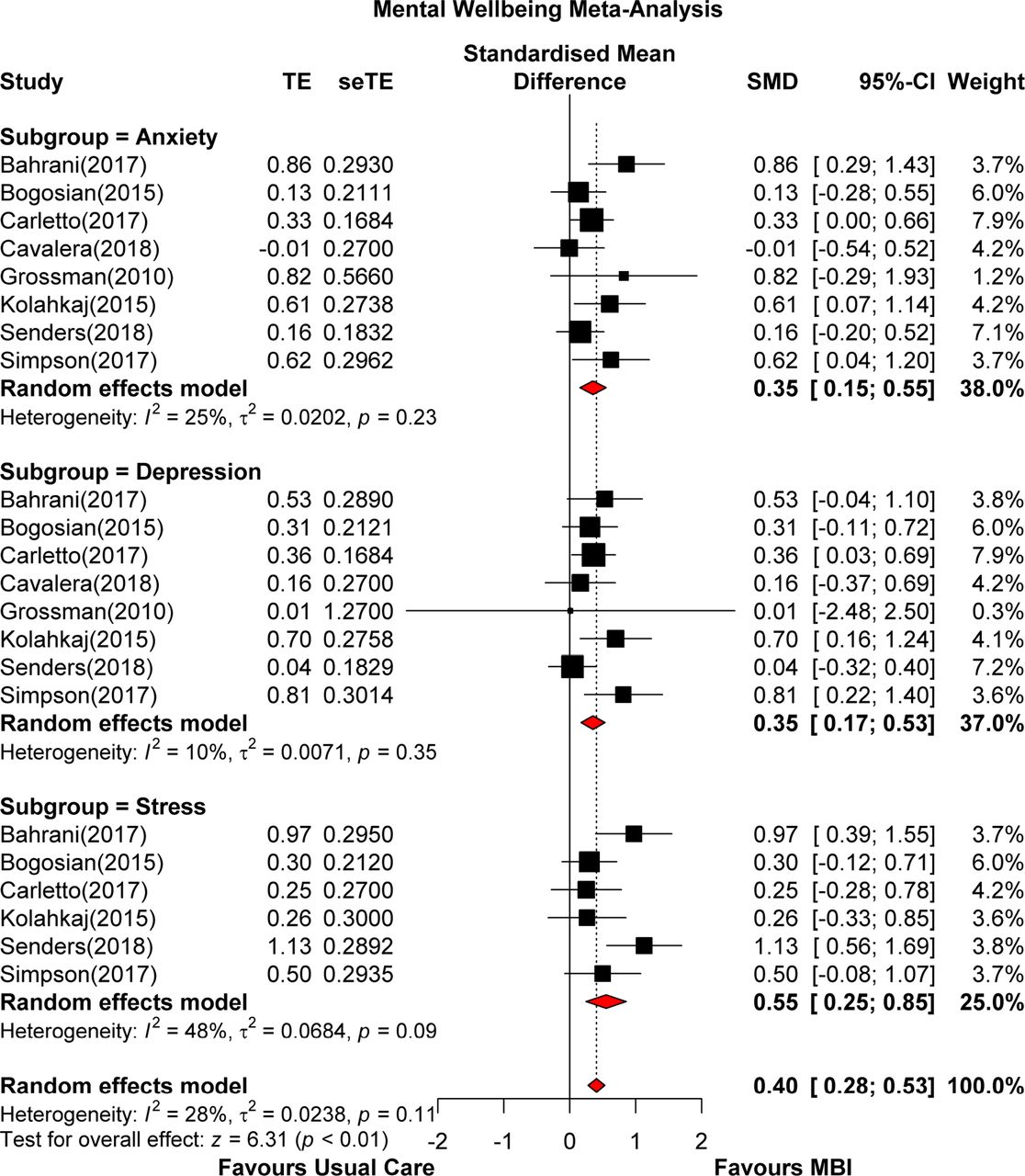
Eleven studies investigated MBI effect on mental well-being,21–26 28–32 however only eight21–24 28–30 32 reported extractable endpoint data. Meta-analysis showed an overall SMD of 0.40 (0.28–0.53; p<0.001), I2=28% (low heterogeneity) (figure 2); against active comparators SMD was 0.17 (0.01–0.32), p<0.05, I2=0% (low heterogeneity) (figure 3). Eight studies evaluated MBI effect on anxiety,21–24 28–30 32 where the SMD was 0.35 (0.15–0.55), I2=25% (low heterogeneity). Eight studies evaluated MBI effect on depression,21–24 28–30 32 where the SMD was 0.35 (0.17–0.53), I2=10% (low heterogeneity). Six studies evaluated MBI effect on stress,21–24 28 29 where the SMD was 0.55 (0.25–0.85), I2=48% (moderate heterogeneity).

Mental well-being (all comparators) forest plot. MBI, mindfulness-based intervention; SMD, standardised mean difference; seTE, standard error of treatment estimate; TE, estimated treatment effect
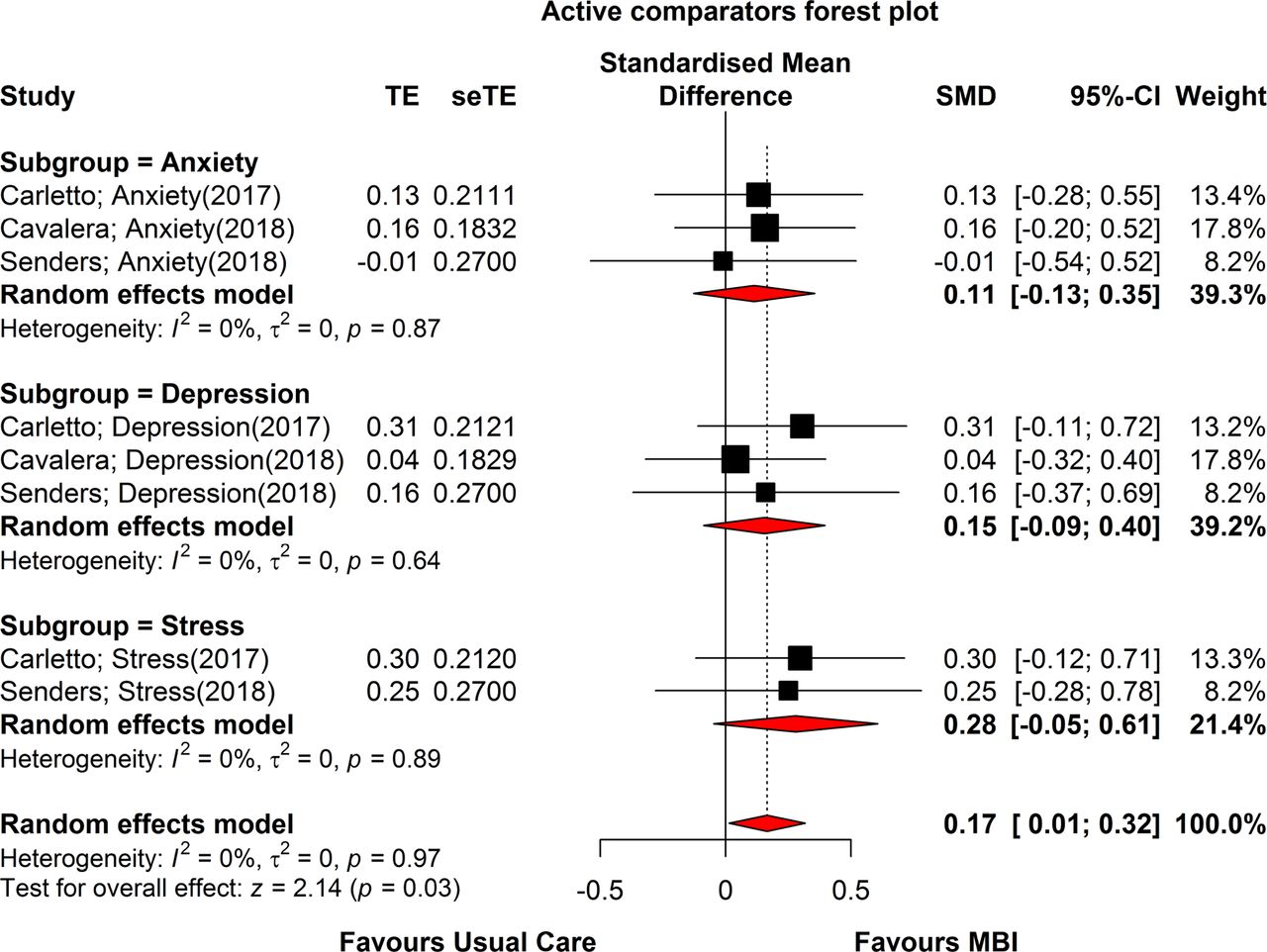
Mental well-being (active comparators only) forest plot. MBI, mindfulness-based intervention; SMD, standardised mean difference.
Heterogeneity and publication bias
Heterogeneity, I2, among the studies was at 28% (low heterogeneity).
There was no evidence of publication bias from the funnel plot (figure 4) and Egger’s Test of asymmetry confirmed that there was no evidence of asymmetry in the funnel plot. However, this was exactly on the threshold at p=0.05. When the trim and fill method was implemented, the estimated number of missing studies was seven. After adjustment for ‘missing’ studies, the pooled SMD estimate was 0.27 (0.12–0.42; p<0.001).
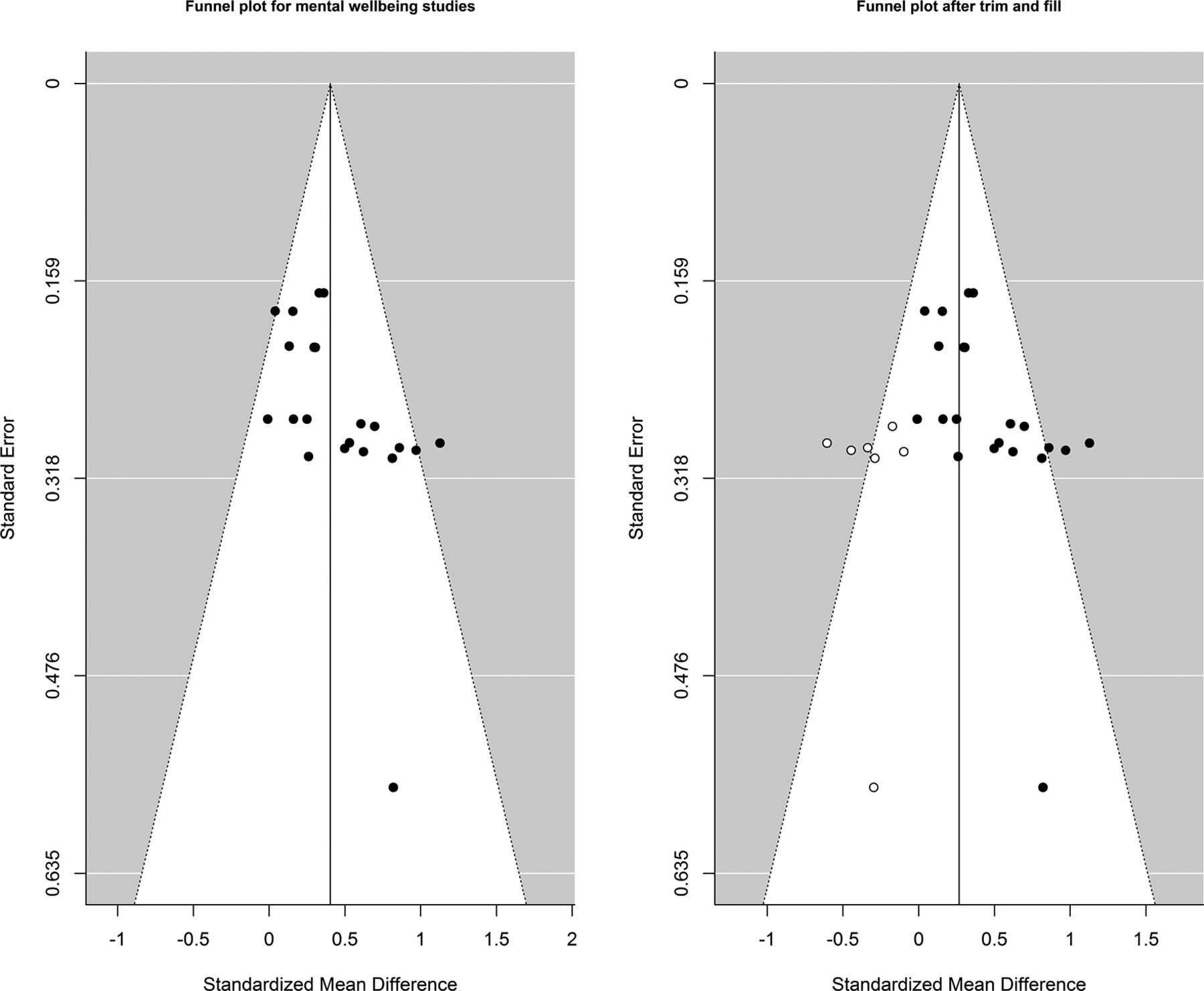
Funnel plot, trim and fill.
Outcomes by intervention type
The largest overall effects were reported for MiCBT,23 SMD 0.80 (0.48–1.12), I2=0%, but this was a pre- post- RCT (n=56), vs usual care. Overall effects for MBCT vs usual care came from a small study28 (n=40), where SMD was 0.78 (0.45, 1.11), I2=0%. In another study24 (n=90), compared with a psychoeducation control, body-affective mindfulness had an overall SMD of 0.24 (0.00–0.48), I2=0%. From the five studies21 22 29 30 32 with extractable endpoint data that used MBSR (total n=449), overall SMD was 0.29 (0.15–0.42), I2=0%, three studies22 29 30 comparing MBSR against usual care, two21 32 against psychoeducation controls.
Study quality
Study quality varied widely. Poor reporting frequently hampered assessment. The highest quality studies derived from Europe and North America. Random sequence generation was well described in nine studies.21–24 27–30 32 Allocation concealment was assessed low risk in six studies,21–24 28 30 and unclear in the remaining six.25–27 29 31 32 Six studies described blinding of assessors,21–24 28 30 while six reported outcome assessor blinding.21–24 28 30 Five studies were adjudged low risk of bias for incomplete outcome reporting,21 22 28 30 32 while selective outcome reporting was adjudged high risk in one.31 Overall, five studies were adjudged low risk of bias,21 22 24 28 30 two unclear,23 32 five high.25 29 31 (table 3). Justifications for risk of bias scores are available in online supplementary file 4.
Supplemental material
Risk of bias
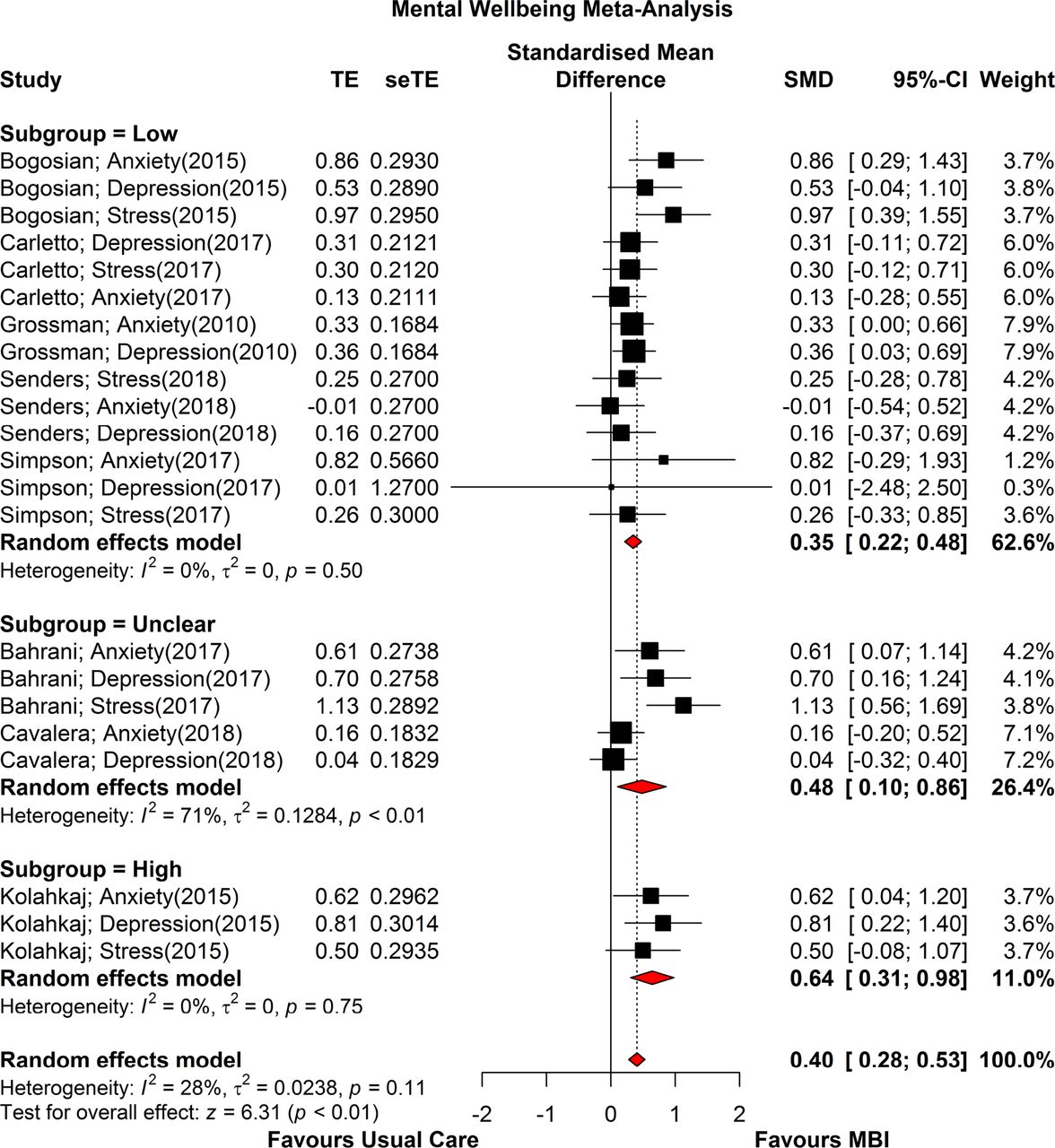
When results were pooled, studies adjudged high risk of bias reported the largest overall treatment effects. Figure 5 shows the SMD for all analysable trials grouped by their risk of bias (high, unclear and low) ratings. High risk of bias (N=3) SMD was 0.64 (0.31–0.98; p=0.002), low risk of bias (N=28) SMD was 0.32 (0.24–0.41; p<0.0001) and unclear risk of bias (N=7) SMD was 0.35 (0.08–0.62; p=0.01). The overall risk of bias analysis showed effect estimates did not significantly differ between risk of bias groups, p=0.20.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of bias forest plot. MBI, mindfulness-based intervention; SMD, standardised mean difference.
Meta-regression
A meta-regression was fitted to analyse the association between predictors and effect estimate. A backward manual selection process was used with intervention type, risk of bias, mean age, gender and EDSS scores as covariates in the model. Covariates were sequentially excluded based on p values (significance level at 5%) to obtain a final model. MBCT and high risk of bias were found to be significant predictors of the effect estimate (table 4)
Meta-regression
Discussion
Summary of main findings
This systematic review and meta-analysis identified twelve RCTs that assessed MBI effect on mental well-being in PwMS. Only three studies compared an MBI against active comparators, six against usual care and in three this was unclear. Two studies explicitly measured intervention fidelity. Most studies had small sample sizes, but six were powered to detect meaningful effects, follow-up ranging from immediately post-MBI–1 year later.
In total, 744 PwMS took part in these studies, the slight majority (60%) having a relapsing phenotype. Where reported, the majority ethnic group was Caucasian, and most participants female. Reporting on levels of comorbidity and disability was mostly poor.
Five studies used MBSR explicitly, two based on MBSR; three MBCT, one MiCBT, one Mindfulness of Movement. The majority of studies were delivered in face-to-face groups. Most studies reported delivering core MBI components and home practices. Class sizes varied. Mostly, teacher characteristics were poorly described. Treatment adherence was reported in seven studies, variably as session attendance±home practice. Attrition ranged widely (0%–39%). Adverse events appear infrequent but were rarely reported.
Generally, study quality has improved since our last review;8 in this current study, five of the RCTs score a low risk of bias on all items in the Cochrane Collaboration tool.
Meta-analysis demonstrated that MBIs are moderately effective for improving mental well-being in PwMS. At present, there is insufficient evidence to recommend any particular MBI over another for PwMS.
Comparison with existing literature
In this study we found MBIs moderately effective for treating anxiety (SMD 0.35; 0.15–0.55), depression (SMD 0.35; 0.17–0.53) and stress (SMD 0.55; 0.25–0.85) in PwMS. A 2004 meta-analysis33 on the use of MBIs in diverse chronic medical conditions reported overall effect sizes (Cohen’s d) for mental health of d=0.50 (0.43–0.56). A 2010 meta-analysis34 on MBSR effects on mental health in patients with varied chronic medical conditions reported smaller effect sizes (Hedge’s g): g=0.27 (0.19–0.35) for depression; g=0.24 (0.10–0.38) for anxiety; and g=0.32 (0.13–0.50) for psychological distress. A 2016 meta-analysis4 of interventions for anxiety and depression in PwMS reported small effect sizes for psychological treatments (mostly CBT, n=9, none testing a MBI) (SMD 0.45; 0.16–0.74), medium effects for pharmacological treatments (SMD 0.63; 0.20–1.07) in improving depression, but limited evidence for effective treatments for anxiety.
When compared with our own analysis, accumulating evidence suggests that MBIs are at least moderately effective for treating anxiety, depression and stress in PwMS; effect sizes comparable with CBT, but marginally less effective than medication, for treating depression.
Strengths of this review
We adopted rigorous search, appraisal and analysis strategies, using a multi-disciplinary team of experienced reviewers for data extraction and a statistician for our meta-analysis. Our methods were guided by the PRISMA checklist,13 the TIDieR checklist11 and the Cochrane Collaboration tool for assessing risk of bias.12
Limitations of this review
This study only included RCTs, necessarily excluding other important sources of data, such as observational and qualitative studies, particularly useful when considering intervention feasibility, acceptability and accessibility. However, by using validated methods such as SPIO, the TIDieR checklist and Cochrane Collaboration tool for risk of bias, various ‘qualitative’ aspects of feasibility, replicability and trial conduct were covered.
Strengths and limitations of the included studies
All studies included in this review were RCTs. However, six had small sample sizes (n≤50), only six were powered to detect statistical significance on outcome measures, and only three tested an MBI against an active comparator. One study did not report on participant age;26 the extractable mean (SD) age from the remaining studies was relatively low (41.4). This potentially indicates a pooled sample skewed towards lower levels of disability.35 Although seven studies stipulated EDSS as an inclusion criterion, only five reported mean (SD) values, making it difficult to determine what role a given MBI may have relative to disability level. While all MS phenotypes featured among the included studies, only two evaluated MBI effects on specific phenotypes,23 31 limiting analysis to pooled data, meaning no recommendations can be made for people with a particular type of MS. Participant SES was poorly covered; important because there is an established link between lower SES and higher incidence of depression in those with MS.36 Both MBSR and MBCT appear effective, with no clear optimal MBI. Several studies altered the manualised MBSR or MBCT courses, often with little/no justification, although most included core MBI components.
Implications for research
Generally, the quality and weight of evidence supporting MBIs to improve mental well-being in PwMS has improved since our previous systematic review. However, many of the RCTs in this meta-analysis did not clearly follow the CONSORT12 criteria and scored unclear or high on the Cochrane Collaboration risk of bias10 tool. Furthermore, several lacked in clarity when it came to describe the MBI used. By using validated, evidence-based tools such as the CONSORT12 and TIDieR11 checklists, study authors could improve reporting in this area and help identify key gaps in knowledge and future research priorities.
The optimal MBI for PwMS remains unclear. As per the MRC guidance on complex interventions,6 PwMS should help design an optimised MBI and this should then be tested in a definitive RCT against current ‘gold-standard’ treatment(s). In PwMS who have stress or depression, this would mean testing against a matched group CBT course and usual care.
An additional consideration for future research in this area could be how MBI training may impact on disease activity in PwMS. Systematic review and meta-analytic data suggest a link between perceived stress and MS relapse.37 38 Preliminary RCT evidence supports CBT-based stress management therapy having a potential role in diminishing underlying disease activity in MS (gadolinium uptake on MRI). Besides the beneficial effects on perceived stress deriving from CBT, the clinical utility of these findings remains unclear.39 However, on the basis of the beneficial effects on perceived stress identified in this meta-analysis, an RCT study examining the effects of MBI training on disease activity in PwMS may now be indicated.
Implications for clinical practice
MBIs effectively improve mental well-being in PwMS. It remains unclear where an MBI might ‘fit’ in the bigger picture of managing comorbid mental health conditions in PwMS, where patient characteristics and clinical severity may vary widely, and stepped care models increasingly predominate.40 However, on the basis of our study and others, it seems prudent to recommend systematic, group-based MBI training with regular home practice41 and follow-up.42
Conclusions
A substantial body of RCT evidence now exists supporting the use of MBIs in PwMS to improve mental well-being. Study quality is improving, but significant scope for improvement still exists in study design and reporting. What constitutes the optimal MBI for PwMS remains unclear.
References
Footnotes
Contributors RS, SWM, NR, ML conceived the design of this project. ML carried out the database searches. RS, SS, JB carried out the literature screening and data extraction. NR and RS carried out the meta-analysis. RS led the writing of the manuscript. All authors read and approved the final version of the manuscript.
Funding This study was funded by the R S McDonald Trust (SC012710).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.