Article Text

Abstract
Objectives: To determine the prevalence of cognitive delay and possible associated dysmorphic features in children exposed to antiepileptic drugs (AEDs) in utero.
Design: Retrospective study of children born to mothers with epilepsy.
Setting: Regional epilepsy clinics in Liverpool and Manchester, UK.
Participants: Children aged between 6 months and 16 years born to mothers with epilepsy.
Main outcome measures: Structured interviews, hospital records, clinical examination, and psychometric tests (Wechsler) were used to assess exposure and intelligence quotient (IQ). Blinded assessment of photographs was used to score children with characteristic dysmorphic features.
Results: A total of 249 children aged 6 and over were studied: 41 were exposed to sodium valproate, 52 to carbamazepine, 21 to phenytoin, 49 to polytherapy, and 80 were unexposed. Mean verbal IQ was significantly lower in the valproate group compared to unexposed and other monotherapy groups. Multiple regression analysis showed that both valproate exposure and frequent tonic-clonic seizures in pregnancy were significantly associated with a lower verbal IQ despite adjusting for other confounding factors. There was a significant negative correlation between dysmorphic features and verbal IQ in children exposed to valproate.
Conclusions: This study identifies valproate as a drug carrying potential risks for developmental delay and cognitive impairment and is the first to suggest that frequent tonic-clonic seizures have a similar effect. Our results need to be interpreted with caution given their retrospective nature. Women with epilepsy need careful counselling about individual risk benefit of AED treatment before pregnancy.
- AEDs, antiepileptic drugs
- AEN, additional educational needs
- FACS, fetal anticonvulsant syndromes
- FSIQ, full scale IQ
- IGE, idiopathic generalised epilepsy
- IQ, intelligence quotient
- LD, learning difficulties
- NART, National Adult Reading Test
- PIQ, performance IQ
- SES, socioeconomic status
- SGSII, Schedule of Growing Skills II
- VIQ, verbal IQ
- WISC-III, Wechsler Intelligence Test for Children
- 95% CI, 95% confidence interval
- antiepileptic drugs
- epilepsy
- pregnancy
Statistics from Altmetric.com
- AEDs, antiepileptic drugs
- AEN, additional educational needs
- FACS, fetal anticonvulsant syndromes
- FSIQ, full scale IQ
- IGE, idiopathic generalised epilepsy
- IQ, intelligence quotient
- LD, learning difficulties
- NART, National Adult Reading Test
- PIQ, performance IQ
- SES, socioeconomic status
- SGSII, Schedule of Growing Skills II
- VIQ, verbal IQ
- WISC-III, Wechsler Intelligence Test for Children
- 95% CI, 95% confidence interval
Epilepsy is common and has a prevalence of 5.25 per 1000.1 One third of people with epilepsy are women of reproductive age and 1 in 200 women attending antenatal clinics are receiving antiepileptic drugs (AEDs).2,3 Both seizures during pregnancy and AED exposure in utero are thought to influence the poorer outcomes seen in children born to mothers with epilepsy.
AEDs have been associated with a two to three fold increase in major malformations in children exposed to AEDs in utero, compared to the general population.4–6 Early reports of minor anomalies7,8 and cognitive delay8–10 alerted investigators to the possibility of longer term adverse effects. A characteristic pattern of minor anomalies may be specific to certain AEDs8,11–13 and may be markers of underlying developmental problems.8,12–15 Others have argued that these anomalies may be associated with epilepsy itself.16,17
Retrospective10,18–20 and prospective studies9,21–23 have documented a higher prevalence of early developmental delay in children born to women with epilepsy, but studies following children up to later years have been conflicting,24,25 particularly as to the role of individual drugs.26–33
In this retrospective study of children born to mothers with epilepsy we report the developmental, neuropsychological, and dysmorphic features of children exposed to AEDs in utero, relative to children of women with epilepsy unexposed to AEDs. The aims were:
-
To determine the prevalence of cognitive impairment in children exposed to AEDs in utero
-
To identify drug specific effects
-
To explore the association of dysmorphic features with cognitive impairment or developmental delay.
METHODS
Study population
Between January 2000 and May 2001, women with epilepsy with children aged 6 months to 16 years were identified from the Mersey Regional Epilepsy Clinic between 1989 and 1999 through a pilot survey,34 the Epilepsy Clinic at the Manchester Royal Infirmary between 1991 and 1999, and the antenatal clinic at St Mary’s Hospital, Manchester between 1991 and 1999.
Women with a progressive neurological deficit, significant learning difficulty, or symptomatic generalised epilepsy were excluded. The study was approved by the northwest multicentre and local research ethics committees.
Clinical assessment
Mothers
A clinician conducted semi-structured interviews of mothers to ascertain information about their epilepsy and relevant pregnancy. Clinical records were used to confirm information. Epilepsy type was categorised into three groups: idiopathic generalised, localisation related, and unclassified epilepsy using the ILAE classification.35
Children
A semi-structured interview was used to collect data for each child on early development, behavioural problems, schooling, additional educational needs (AEN, defined as having a statement for AEN, being on the register for AEN, or requiring extra help in mainstream school), and the need for additional therapy including speech therapy.
Dysmorphic features, defined as cosmetic variations without disability, were recorded by an examiner at each centre, using a checklist of 30 features previously described for fetal anticonvulsant syndromes (FACS).36 Children’s faces, profiles, hands, and feet were photographed. These were assessed by two geneticists and a paediatrician, who were unaware of the drug exposure of the children. The reviewers gave a consensus score for overall appearance on a scale of 0–10 for typical features of FACS. Scores were categorised as normal appearance (0), minor (0.5–3), moderate (4–6), and severe features of FACS (7–10).
Major malformations, defined as structural abnormalities requiring medical or surgical intervention to prevent disability, were recorded using the EUROCAT guidelines.37
Neuropsychological tests
Children aged between 6 and 16 years were blindly assessed by a neuropsychologist using the Wechsler Intelligence Test for Children (WISC-III)38 which provides a measure of full scale intelligence quotient (FSIQ) from a composite score of verbal IQ (VIQ) and performance IQ (PIQ). Psychomotor and cognitive development was assessed in children from birth to 5 years using the Schedule of Growing Skills II (SGSII).39 Maternal intellectual functioning was assessed using the National Adult Reading Test (NART).40
Socioeconomic status
Socioeconomic status for each child was classified according to the National Office of Statistics guidelines41 using the details of the father or the mother where the former were unavailable.
Statistical analysis
For each outcome those exposed to specific monotherapy regimes or any polytherapy were compared to unexposed children.
The primary outcome was the IQ in children over 6. The study had 90% power to detect a 10 point difference in IQ with unequal sample sizes (72 unexposed and 36 exposed). A one way analysis of co-variance with Bonferroni adjustment of significance level was used to compare mean FSIQ, VIQ, and PIQ between multiple groups and Student’s t test for two groups.
Linear regression was used to study explanatory factors for VIQ, PIQ, and FSIQ. Factors identified a priori included maternal age at birth, number of convulsive seizures during pregnancy, maternal epilepsy type, regular alcohol/smoking during pregnancy, pre-conceptual folic acid, family history of malformations and learning difficulties in a first degree relative, maternal FSIQ (as assessed by NART), and socioeconomic status. Spearmans correlation was used to examine correlation between dose of AEDs and IQ, and dysmorphic features and IQ.
Statistical analyses were undertaken using the SPSS statistics computer package (version 10).
RESULTS
Characteristics of the mothers, their pregnancies, and their children
From the 547 mothers approached, 219 (40%) agreed to participate (169 from epilepsy clinics and 50 from the antenatal clinic) (table 1). Some 48% of the participating mothers (106) had responded to a pilot survey about their children’s schooling.34
Characteristics of mothers and their epilepsy
There were a total of 375 children aged between 6 months and 16 years (mean age 7.7 years, SD 4.3). Their drug exposures are described in table 2.
Characteristics of pregnancies (frequencies are shown)
The reasons for non-exposure were pregnancy predating the diagnosis of epilepsy (52%), seizure free mothers (34%), and other reasons including non-compliance (14%).
We have no evidence that drug exposure influenced the likelihood of inclusion. While we do not have information on the drug exposures of all non-participants, the subset of participants who responded to both the pilot survey34 and the current study does not suggest bias (32%, 38%, and 32% for valproate and carbamazepine monotherapy and unexposed, respectively). Furthermore, the distribution of drug exposures in this study conforms with that seen in cases collected for an ongoing prospective study (24% of cases carbamazepine monotherapy, 20% valproate monotherapy, and 20% unexposed).
Developmental and cognitive outcomes
Children over the age of 6: Wechsler Intelligence Scale
Of the 256 children, 249 completed the WISC (table 3). Two refused to take part, one was too old when recalled for testing, one was lost to follow up, and three were unable to complete the test due to behavioural problems, speech impairment, and severe learning difficulties, respectively.
WISC scores for children aged 6 years or older by drug exposure
The mean FSIQ was at the low end of the average range for children exposed to monotherapies and was similar to the mean score in unexposed children. Those exposed to polytherapies had a lower mean score than the unexposed and those exposed to monotherapies, but this was not statistically significant.
The mean PIQ was within or close to the average range in all drug groups, with no significant difference among the different exposures.
The mean VIQ was in the low average range in those exposed to VPS monotherapy and was significantly lower than the unexposed and other monotherapy drug groups, being on average 7 points lower (table 4). Those exposed to VPS as part of a polytherapy regime had a non-significant lower mean VIQ.
Independent Student’s t test for comparisons between groups for VIQ
There was a greater proportion of children scoring in the low (23%) and exceptionally low range (7%) in the unexposed group than one would expect, potentially reflecting a bias introduced by mothers self selecting to participate in the study (fig 1). However, among those exposed to VPS monotherapy, the proportion of children scoring in the low (20%) and exceptionally low range (22%) was significantly greater than in the carbamazepine exposed group (χ2 for trend 8.431, df 1, p = 0.004).

Distribution of VIQ according to monotherapy drug exposure in utero compared to the expected score in the general population. The WISC is an age standardised test which has been administered to a large representative sample of the UK general population, allowing norms to be determined from the results. The scales have a mean of 100 and SD of 15, and the expected distribution in the normal population is shown at the far left.38
The odds ratio for a VIQ of 69 or less compared to the unexposed group was significantly greater for VPS monotherapy (3.5, 95% CI 1.1 to 10.6).
A total of 88 younger siblings of 158 children aged 6 and over were also assessed. This could represent a source of bias. When the IQ scores were examined in the first born only, the results remained consistent with those from all children. Mean VIQ in first born children exposed to VPS (n = 27, 82.7, 95% CI 75.6 to 90.0) was significantly lower than the unexposed group (n = 53, 94.1, 95% CI 89.7 to 98.5, p = 0.006) and those exposed to carbamazepine (n = 27, 95.5, 95% CI 87.9 to 103.0, p = 0.006).
Exploration of factors predicting VIQ in the children
Univariate linear regression analysis (table 5a) using all the a priori listed variables, showed that five factors were significantly associated with VIQ, but multiple regression analysis suggested only three factors: lower maternal IQ, valproate exposure, and five or more tonic-clonic seizures in pregnancy were independently predictive of a lower VIQ (table 5b). All variables were included in the final model if they reached a significance of p<0.1 in univariate analysis or were considered clinically important. The numbers of mothers with regular alcohol were too small to explore in the analysis.
Univariate linear regression for VIQ
Multiple linear regression for VIQ for all children
Inclusion of siblings may have introduced bias, particularly if a large proportion of one drug exposed group were from one family, and an apparent drug effect may have been confounded by a genetic effect. We have explored this bias by performing the regression analysis on the first born children only. The results from these analyses were similar to those from inclusion of all children. Univariate analysis showed evidence for a decrease in children’s VIQ in association with valproate exposure, five or more tonic-clonic seizures in pregnancy, and a family history of learning difficulties, in contrast to an increase with increasing maternal IQ (as measured by NART) and maternal age. However, multiple regression in this group confirmed that the main predictive factors were maternal IQ (β coefficient 0.600, 95% CI 0.386 to 0.813, p<0.001), exposure to valproate in utero (β coefficient −10.912, 95% CI −17.785 to −4.308, p = 0.006), or five or more tonic-clonic seizures (β coefficient −15.154, 95% CI −22.564 to −7.744, p<0.001). Socioeconomic class as a group variable did not contribute significantly to the variance of the model though the β coefficient for the lower socioeconomic group did reach significance (β coefficient −6.242, 95% CI −12.350 to −0.134, p = 0.045). This exploration showed that the significant variables had larger β coefficients (or estimate of effect size) than those from the analysis that included all children. We would conclude that the bias from inclusion of siblings is unlikely to explain our findings.
The mean maternal IQ (100.0, 95% CI 98.3 to 101.7) was within the average range regardless of mother’s epilepsy type or drug use in pregnancy, with no significant differences between epilepsy or drug groups.
Among children exposed to VPS, 59% had mothers with IGE while 78.8% exposed to carbamazepine had mothers with localisation related epilepsy (χ2 = 19.613, df 5, p = 0.001). While this association may have prevented detection of an effect of IGE on VIQ in multivariate analysis, it would not explain the lack of association in univariate analysis.
There was no significant association between monotherapy regimes in pregnancy and seizures during pregnancy (χ2 for trend = 2.838, df 1, p = 0.092). Those exposed to five or more tonic-clonic seizures in pregnancy were more likely to have mothers with focal epilepsy (63.4%) than IGE (36.6%).
The number of children with major malformations (15), epilepsy (six), exposure to regular alcohol intake (27), and adequate folic acid (15, pre-conceptual dose of 5 mg) were too small to explore in a regression analysis. Exploration of exposure to folic acid at any dose in any stage of pregnancy (115) versus no exposure failed to show any association (R2 = 0.00, F = 0.109, p = 0.742).
In general, the proportion of children of all ages with a major malformation was higher in the VPS monotherapy group (14%) compared to the unexposed group (4%). Of the 15 children over the age of 6 with major malformations, seven were exposed to VPS monotherapy. However, we found no evidence of an association between major malformations and low VIQ. The mean VIQ (91.33, 95% CI 84.83 to 97.84) in those with major malformations (15, 6%) was similar to those without (90.6, 95% CI 88.4 to 92.7). Two children with malformations (13.3%) had a VIQ below 79. Both were exposed to VPS, one had hypospadias, and the other a split hand.
Exploration of dose effect
There was no significant correlation between VIQ and drug dose for carbamazepine or phenytoin. There was a negative correlation between VIQ and VPS dose in the first trimester (Spearman’s ρ −0.399, p = 0.011) and the whole pregnancy (Spearman’s ρ −0.293, p = 0.093), but the latter was not significant. Exploring this further to look for a possible threshold effect, we divided the dose range into three approximately equal portions (table 6). Doses above 800 mg of valproate were associated with, on average, 8–15 points lower VIQ, compared to those on 800 mg and below, though the numbers were small. The VIQ of children exposed to 800 mg or below was similar to unexposed children.
Dose effect of valproate monotherapy in utero on VIQ in children
Children under age 6
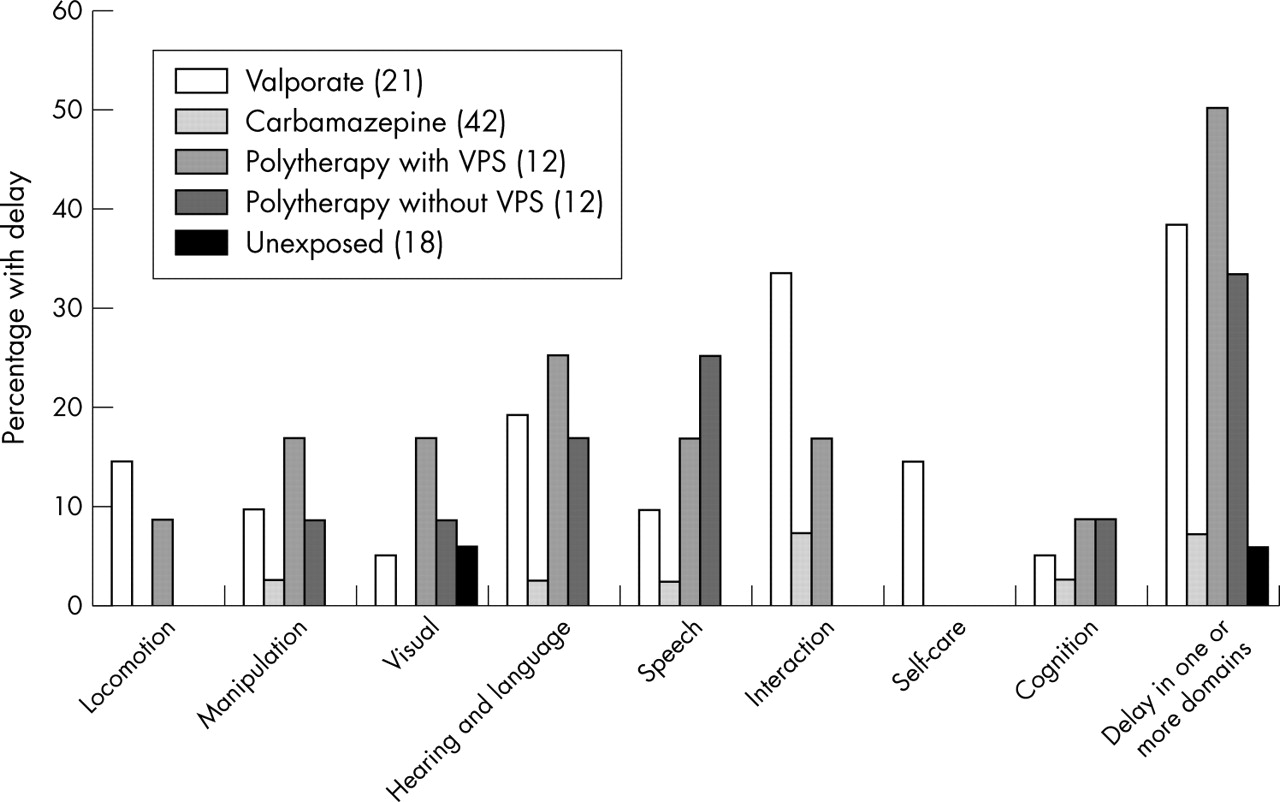
A total of 119 children aged under 6 completed the SGS assessment. A higher proportion of children exposed to VPS monotherapy and to polytherapy showed delay in some domains compared to carbamazepine exposed or unexposed children. This was particularly marked for the interaction (VPS 33.3%, unexposed 0%,) and hearing and language domains (VPS 19%, unexposed 0%) (fig 2).
{kind=link}
{kind=link}
Percentage of children with delay in each of the domains assessed by the SGSII. Nine skill areas are assessed with a separate score for cognition. Passive posture and active posture are not shown as these are only assessed in children up to 12 months and were normal in all groups. Each skill area is scored independently and categorised as “normal” or “delayed” for the child’s age.
There was a significantly higher odds of any delay in those exposed to VPS monotherapy (OR 10.5, 95% CI 1.2 to 94.5) compared to the unexposed group.
AENs and therapeutic input
It is evident that valproate exposure in monotherapy or polytherapy is associated with AENs (table 7, for children aged 4 and above). A total of 19.7% (74) of all the children had received speech therapy input at some point. This was particularly high among the VPS monotherapy exposed group (47.6%, 30) with the other groups being similar to the unexposed group (15, 14.6%).
Educational problems
Only nine children had received a specific diagnosis requiring therapeutic input. In particular, there were two with Asperger’s syndrome (one VPS monotherapy, one VPS polytherapy), two with attention deficit hyperactivity disorder (both VPS monotherapy), and five with dyspraxia (two VPS monotherapy, three unexposed).
Dysmorphic features and low VIQ
The majority of children had a normal appearance or only mild dysmorphic features regardless of drug exposure. However, dysmorphic features were more commonly seen in children exposed to VPS, with 44% having moderate to severe dysmorphic features in contrast to those exposed to carbamazepine (9.2%) and the unexposed (2.2%).
In the children aged 6 and over, 22% of those with normal appearance had a low VIQ (<79) in contrast to 55% of those with moderate to severe features. The association between VIQ and dysmorphic features was most marked in the VPS monotherapy group, which was the only group with a significant correlation (Spearman’s ρ −0.436, 95% CI −0.107 to −0.827, p = 0.007). This probably reflects the fact that the majority of those with dysmorphic features were in the VPS exposed group.
DISCUSSION
The optimal management of women with epilepsy during their childbearing years, and during their pregnancies in particular, presents a considerable clinical dilemma. It has been recognised that treatment with AEDs during pregnancy is associated with an increased risk of major congenital malformation. However, the justification for treatment has been that the risks of seizures to a pregnancy are greater than those of AED therapy. This needs to be questioned. We need to define what risks we are considering and whom they might affect, mother or child?
The confidential enquiries into maternal deaths in the United Kingdom42–46 do identify women with epilepsy as being at particular risk (table 8). If it is assumed that between 1:200 and 1:250 pregnancies occur in women with a history of epilepsy, it can be calculated that the approximate odds for maternal death are 10 times higher for women with epilepsy than the general population. This seems to represent an increased mortality risk during pregnancy above the usual standard mortality rate of 2–3 for epilepsy throughout life as a whole.47,48 The case histories in the reports suggest these are due to seizure occurrence often associated with stopping AEDs or with poor compliance. There is little literature or data to quantify any risk for malformations or other adverse outcome in the fetus from seizures.49 Inevitably, disentangling the potential effects of seizures from those of AEDs will be confounded by the fact that women with more severe epilepsy will be exposed to a higher burden of drug therapy during their pregnancies.
Confidential enquiry into maternal deaths 1985–99
The main focus of research for risk to the fetus has been the risk of major congenital malformations. However, minor dysmorphic features, possibly associated with developmental delay, have been reported with most AEDs including phenytoin,8 carbamazepine,12,14 and valproate.11,13 Though the fetal valproate syndrome was first described in 1984,11,13 the association between dysmorphism and cognitive impairment has remained unclear, including whether more subtle cognitive problems might occur in the absence of dysmorphism.
This study has focused on the cognitive and developmental outcomes in children born to women with epilepsy. Retrospective ascertainment through epilepsy clinics is liable to bias, being more likely to identify women with more problematic epilepsy. The relatively low level of response to participation (40%) is likely to lead to an overestimate of the size of any observed effects. There seems little doubt that women whose children have problems were more likely to participate than those whose children are developing normally. These biases seem to be evident in the assessments of children whose mothers’ pregnancies were not exposed to AEDs. We cannot exclude that this bias may operate differently for different exposures though this seems unlikely.
The unexposed comparator group may be criticised as being an imperfect control group, but no perfect control group exists. It does offer the possibility of a limited examination of any possible genetic contribution to our results. Inevitably this group does differ in many respects from those receiving treatment, but the use of a multiple regression model has allowed us to explore some confounding factors including seizure frequency, epilepsy type, and maternal IQ.
Our results demonstrate that children exposed to sodium valproate may show a specific pattern of impairment for verbal abilities without statistically significant effects on PIQ or FSIQ. VIQ is a measure of verbal abilities and verbal comprehension, while PIQ is more a measure of non-verbal problem solving abilities. Children with severe mental retardation often have a low FSIQ, while those with a learning disability may have discrepancies between their verbal and PIQ. Reductions in mean VIQ compared to performance and FSIQ are well recognised in these groups of children.38 We have explored the implications of this in a further publication.
Similarly it is evident that younger children are already exhibiting delayed development as measured by the schedule of growing skills (SGS) including effects on speech and language. The consistency of these observations across the age groups, using different tools, argues for their validity, as does an observed dose related effect for valproate with as much as an 8–15 point difference in VIQ between children exposed to doses below 800 mg/day of valproate compared to those exposed to higher doses. Interpretation of the dose effect is limited by small numbers, lack of information regarding compliance, or drug levels in pregnancy. However, this may be taken as soft evidence that doses below 800 mg may be safe. In the group as a whole as well as the first born children only, exposure to valproate appears to be one of the three main determining factors of a child’s VIQ along with maternal IQ and the occurrence of five or more tonic-clonic seizures during pregnancy. This latter finding is one of the first attaching a developmental risk to the occurrence of seizures during pregnancy.
Our results conflict somewhat with those of Dean et al.20 They found adverse effects with valproate, carbamazepine, and phenytoin exposure in early development using a structured questionnaire in mothers ascertained from maternity hospital records. Differences may result from the different methodologies used. The focus on valproate as a particular risk to development is in keeping with independent series, published in abstract form.30,31 The pattern of cognitive impairments in older children, with the emphasis on impaired verbal abilities, is similar to that found in a smaller series.50
While our results may indicate higher odds of cognitive problems due to valproate, it would be unwise to use our study to estimate the level of absolute risk, which will only be satisfactorily ascertained by a prospective study with community based ascertainment. If we assume that the 60% of the children who we were unable to examine had a similar exposure to AEDs and all had normal IQs, then 17% of all valproate exposed children would have had an IQ in the low range or below compared to an expected rate of 9% in a normal population.38 It is evident within the population studied that the verbal impairments noted have considerable consequences both in terms of demand for therapy and difficulties in schooling.
We found a consistent correlation with the degree of dysmorphism that children show and the likelihood of significant cognitive impairment. This argues that the fetal valproate syndrome constitutes a real clinical entity that includes developmental delay and cognitive impairments, but that some children might exhibit some developmental delay without marked dysmorphism.
While the mechanisms leading to the fetal valproate syndrome are uncertain, abnormalities of folate metabolism have been implicated.51 Our data cannot provide support for a protective effect for preconceptual folate, as only 15 women took adequate doses of folate in this way. While it is usually accepted that many of the risks for major malformations from AEDs are due to first trimester exposure, we have no evidence to indicate the degree to which the observed impairments might be related to first trimester exposure or indeed later exposure.
What then are we to advise women with epilepsy about pre-conceptual drug therapy? Valproate may best be avoided in women with localisation related epilepsy. Here there are a number of alternatives, including carbamazepine, that are more likely to be effective in seizure control than valproate.52
The dilemmas persist, however, for women with idiopathic generalised epilepsy. While there are no satisfactory trials comparing the efficacy of valproate to other AEDs in these syndromes, there is a clinical consensus and some open uncontrolled data indicating its superiority over other AEDs for seizure control.53,54 Thus, here there is a potential conflict between the desire to avoid complications from seizures and from drug therapy. Women could be offered alternative treatment with phenytoin, lamotrigine, or carbamazepine, all of which may offer some protection against tonic-clonic seizures. The inclusion of a small number of women with phenytoin in our study does not suggest any major risk of cognitive impairment, which is in agreement with other investigators,25 and it appears a relatively low risk drug for major malformations.3,5,55 Lamotrigine has been widely advocated for the treatment of women. Again it appears to be a relatively low risk antiepileptic drug for major malformations (approximately 4%),55 but there is no evidence concerning neurodevelopmental outcomes. Carbamazepine might be considered as an alternative, but it can on occasions exacerbate other seizure types seen in the idiopathic generalised epilepsies (myoclonus and absence). The gradual withdrawal of valproate and a switch to one of these options (or indeed other newly licensed AEDs without evidence of safety in pregnancy) could be discussed with women with IGE, but if seizure control is not optimal then a combination of low dose valproate with an additional drug might be an acceptable alternative. However, there is some evidence that a valproate-lamotrigine combination carries a relatively high risk of malformation56 (Morrow, personal communication). For women with idiopathic generalised epilepsy who have enjoyed significant remission of their epilepsy, then withdrawal of AEDs may be considered, though if they have IGE the risk of recurrence within 1–2 years of withdrawal may be high.57 Ultimately, drug withdrawal involves a balance of risks, with loss of seizure control having potential implications not only for the mother and the course of her pregnancy but, as suggested by our study, her child as well. In order to allow women to make an informed choice we require more accurate data about seizure control and pregnancy outcomes. This has implications for the design of prospective studies.
The results of our study are of concern given that valproate was first licensed in the United Kingdom in 1975. The last 10 years have seen the licensing of seven new AEDs, some of which may come to be used commonly during the childbearing years. It is essential that adequately controlled prospective studies are established now to identify the level of risk for cognitive impairment in children of women taking both new and established AEDs during pregnancy.
Our data demand that epilepsy services deliver adequate information and counselling about drug treatment during childbearing years. This needs to be offered before pregnancy and updated regularly. Counselling might initially take place as part of an adolescent clinic transferring care from paediatric to adult services. Current services and practice would need to evolve considerably as for many women these issues are only raised when they present in the first trimester of pregnancy.
REFERENCES
Footnotes
-
Competing interests: none declared
Linked Articles
- Editorial commentary