Article Text

Abstract
A case of an 82-year-old woman who experienced repeated falls is described. She exhibited a cardioinhibitory carotid sinus hypersensitivity after right carotid sinus massage (CSM), but without evidence of orthostatic hypotension. After a pacemaker was implanted, she did not experience any falls, dizziness or syncope. Her balance eventually deteriorated, but she remained cognitively intact and died from lung cancer at the age of 89 years. Neuropathological examination showed only age-related Alzheimer’s disease pathology and a few α-synuclein-positive granular deposits and neurites in the dorsal nucleus of the vagus and solitary tract nucleus in the medulla, but a marked α-synuclein pathology in the stellate ganglia. The cardioinhibitory element of her CSM was possibly because of the α-synuclein pathology in the ganglion, which impaired sympathetic transmission. This case shows another phenotype among patients with α-synucleinopathy.
- CNS, central nervous system
- CSH, carotid sinus hypersensitivity
- CSM, carotid sinus massage
- DLB, dementia with Lewy bodies
- PAF, pure autonomic failure
Statistics from Altmetric.com
- CNS, central nervous system
- CSH, carotid sinus hypersensitivity
- CSM, carotid sinus massage
- DLB, dementia with Lewy bodies
- PAF, pure autonomic failure
Carotid sinus hypersensitivity (CSH) is one of the most common causes of falls and syncope in elderly people.1,2 CSH is an exaggeration of the carotid sinus-mediated baroreflex, which is activated by stimulation of local mechanoreceptors in response to intra-arterial pressure changes. CSH is characterised by an abnormal heart rate, a slowing of >3 s asystole (cardioinhibitory CSH) or a fall in systolic blood pressure of >50 mm Hg (vasodepressor CSH) during a short period of massage over either sinus. CSH rarely occurs before 50 years of age and increases in frequency thereafter.1 Hypertension, atherosclerosis and coronary artery disease are common in patients with CSH.3 The disorder has also been reported in patients with tumours of the head and neck4 or in those with dementia, dementia with Lewy bodies (DLB) in particular.5 The underlying pathophysiology, however, is largely unknown. We describe the neuropathological findings on a patient with symptomatic CSH.
CASE REPORT
A woman aged 82 years, who was living alone, had a 4-year history of multiple, recurrent and unexplained falls that occurred about once a month and had recently increased in frequency. At the referral appointment, she denied prodrome or a loss of consciousness. She had sustained numerous injuries, including bilateral shoulder and wrist fractures. She was eventually confined to the house because of the fear of falling. Drugs prescribed were diltiazem, isosorbide mononitrate and diazide for hypertension, and inhalers for chronic obstructive airway disease.
Clinical examination showed her gait and balance to be normal, she was in sinus rhythm, had a normal surface electrocardiogram and a blood pressure of 140/90 mm Hg. No orthostatic hypertension was noted. During 5 s of supine right carotid sinus massage (CSM), her heart stopped for 8.8 s, blood pressure dropped from 158/51 mm Hg to unrecordable values and she lost consciousness, which she could not recall later.
Diltiazem was discontinued because it could cause bradycardia. The patient was reviewed 1 month later. In the intervening period she had had three falls. Once again, right supine CSM produced 6 s of asystole and the blood pressure dropped from 179/97 to 99/54 mm Hg, resulting in a loss of consciousness. Results of other standard cardiovascular investigations, including ambulatory blood pressure and heart rate monitoring, repeated orthostatic blood pressure measurements and head-up-tilt studies were not diagnostic. CSH was diagnosed and she received a dual-chamber cardiac pacemaker to correct the bradycardia. In subsequent years, she did not experience any falls or syncope. She remained in sinus rhythm and did not exhibit orthostatic hypotension. However, she continued to complain of a marked loss of confidence and had a fear of falling. Her balance had deteriorated, although gait, 24-h blood pressure and 24-h heart rate were normal. Cognitive function remained intact—the Mini-Mental State Examination result 16 months before her death was 29/30. She died from lung cancer at the age of 89 years.
AUTOPSY FINDINGS
A limited postmortem examination of the head, neck and thorax showed a few small, old infarcts in the myocardium and calcified coronary arteries without major occlusion. The carotid arteries showed atherosclerosis, but no major occlusion or vulnerable atherosclerotic plaque was present. We found no evidence of any tumours in the neck. The weight of the brain was 1200 g. An old haemorrhagic area (2×8 mm) was seen below the insular cortex in the white matter. The substantia nigra and locus ceruleus showed normal pigmentation.
The right half of the cerebrum and mid-brain, whole pons, medulla, cerebellum, stellate ganglia and samples from the heart, coronary arteries and carotid arteries were fixed in formalin for 2 months. The tissues were extensively sampled and embedded in paraffin wax to be cut at a thickness of 6 μm for haematoxylin and eosin staining. Silver (Bielschowsky and Gallyas) and Loyez myelin staining methods were used for sections of selected blocks of the central nervous system (CNS). Primary antibodies for immunohistochemistry included AT8 (Innogenetics, Gent, Belgium), α-synuclein (Novocastra, Newcastle upon Tyne, UK), β-amyloid (DakoCytomation, Ely, UK) and ubiquitin (DakoCytomation).
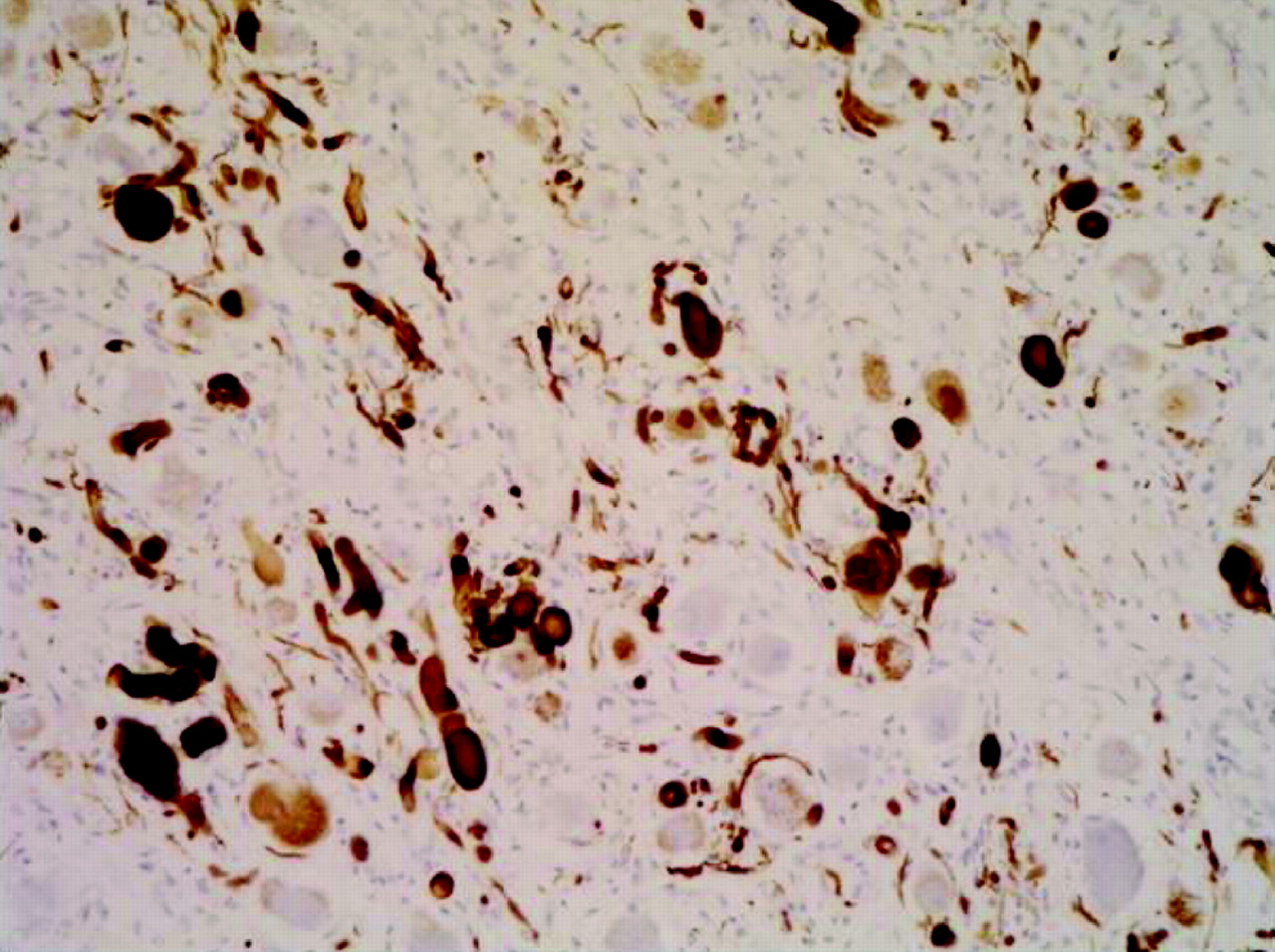
On microscopic examination, the sections showed a moderate density of neuritic plaques, but no neurofibrillar tangle in the neocortex. Braak staging was rated as III. Severe amyloid angiopathy was present focally. No infarct was seen. A few small islands of metastatic adenocarcinoma were present in the medial thalamus. Small foci with extensive myelin loss and occasional foamy macrophages were present in the centre of the pons on both sides of the midline. This finding was interpreted as a form of central pontine myelinolysis, possibly related to the terminal stage of the lung cancer. No neurone loss, Lewy body or α-synuclein-positive neurite was present in the substantia nigra or locus ceruleus. Only a few α-synuclein-positive granular deposits and neurites were seen in the region of the dorsal nucleus of vagus and solitary tract nucleus. The stellate ganglia showed numerous relatively wide, eosinophilic neurites, spheroids and intraneuronal Lewy body-like inclusions with an extensive accumulation of α-synuclein (fig 1). An occasional, pale Lewy body-like inclusion, a few ganglion cells with α-synuclein-positive granular deposits and occasional α-synuclein-positive neurites were present in the epicardial fat.
{kind=link}
α-Synuclein-positive inclusions and neurites (brown) in the stellate ganglion.
DISCUSSION
The carotid sinus reflex is triggered by the carotid baroreceptors at the medial aspect of the proximal internal carotid artery.6 The afferent signal is transferred along the carotid sinus nerve to the glossopharyngeal nerve, and then to the solitary tract nucleus in the vasomotor centre in the medulla.6 The efferent signal follows the vagus nerve and causes bradycardia as the cardioinhibitory component, and it takes a parallel route through the caudal and rostral ventrolateral medulla to the intermediolateral column of the spinal cord, where it decreases the activity of the preganglionic sympathetic neurones as the vasodepressor component.6,7 Importantly, the postganglionic sympathetic cardiopulmonary nerves arise from the stellate ganglia and the inferior halves of the cervical sympathetic trunks.8
The connectivity between the baroreceptors and vasomotor centre in the medulla may be impaired in several ways. The surgical removal of carotid body tumours destroys the adjacent fibres of the carotid sinus nerves. This initially results in increased blood pressure and later in poor regulation of blood pressure.9 Tumours of the head and neck region can cause exaggerated activation or hypersensitivity of the carotid baroreceptors by direct invasion of the carotid sinus or by compressing the glossopharyngeal nerve.4 The carotid sinus hypersensitivity is also associated with DLB, an α-synucleinopathy of the CNS.5 In the patient described here, the CSH was associated with a notable accumulation of α-synuclein in the cardiopulmonary sympathetic ganglia, but without a marked accumulation in the CNS. The mild pathology in autonomic nuclei in the medulla and clinically proved response of bradycardia to CSM suggests that the parasympathetic arm of the signal pathway was not profoundly damaged. Therefore, the cardioinhibitory CSH in this patient was probably caused by an imbalance between the apparently intact parasympathetic efferent pathway and poorly functioning cardiac postganglionic sympathetic nerves. The possible low activity of the cardiac postganglionic sympathetic neurones and their delayed response to the decreasing blood pressure resulted in an inefficient and delayed recovery after a parasympathetic cardioinhibitory impulse.
The pathological findings in this patient are similar to those seen in patients with pure autonomic failure (PAF), which are also associated with the accumulation of α-synuclein in the autonomic nervous system.10 The accumulation of α-synuclein-positive material in the brain stem, however, is usually more extensive in patients with PAF. In addition, clinically, PAF is characterised by orthostatic hypotension, with evidence of more widespread autonomic failure but without other neurological features.11 On the other hand, orthostatic hypotension in PAF is often preceded by other, milder symptoms related to abnormalities in the function of the autonomic nervous system, such as constipation, urinary incontinence, heat intolerance and syncope, and erectile dysfunction in men.10,12 Our patient did not show any evidence of autonomic failure other than CSH, and her brain stem showed only minimal α-synuclein accumulation. Thus, the limited clinical symptoms, which were successfully managed with a pacemaker, should be attributed to focal α-synucleinopathy. We cannot exclude the possibility of a more widespread α-synuclein deposition in the peripheral autonomic nervous system, however. The consent for limited autopsy did not permit extensive assessment.
Although no published information is available on the frequency of α-synucleinopathy in the peripheral autonomic nervous system of elderly people, the relatively common occurrence of α-synuclein in the brains of elderly people suggests that it may not be rare. The clinical and neuropathological overlap between PAF and other α-synucleinopathies with Lewy bodies (Parkinson’s disease and DLB) suggests that these diseases are only different phenotypes of one disease process.13 In this context, we describe a new phenotype for this group of α-synucleinopathy. As in this patient, the cardiac but not the medullary sympathetic neurones seem to be affected in people with Parkinson’s disease and PAF.14,15 Therefore, on the basis of these prior findings and our own findings, we hypothesise that the cardioinhibitory CSH in patients with Lewy-body pathology is more related to the severity of such pathology in the cardiac sympathetic neurones rather than in the CNS.
REFERENCES
Footnotes
-
Funding: This work was partially supported by grants from the Medical Research Council UK and the Alzheimer’s Research Trust (ART) UK. VM was supported by studentship from ART.
-
Competing interests: None.
-
Informed consent was obtained from the patient’s next of kin for publication of the patient’s details in this report.