Article Text

Abstract
Objective: To report the nature of stroke in patients infected with human immunodeficiency virus (HIV) in a region with high HIV seroprevalence and describe HIV associated vasculopathy.
Methods: Patients with first ever stroke, infected with HIV and prospectively included in the stroke register of the Groote Schuur Hospital/University of Cape Town stroke unit were identified and reviewed.
Results: Between 2000 and 2006, 67 of the 1087 (6,1%) stroke patients were HIV infected. Of these, 91% (n = 61) were younger than 46 years. Cerebral infarction occurred in 96% (n = 64) of the HIV positive patients and intracerebral haemorrhage in 4% (n = 3). HIV infected young stroke patients did not demonstrate hypertension, diabetes, hyperlipidaemia or smoking as significant risk factors for ischaemic stroke. Infection as a risk factor for stroke was significantly more common in HIV positive patients (p = 0.018, OR 6.4, CI 3.1 to 13.2). In 52 (81%) patients with ischaemic stroke, an aetiology was determined. Primary aetiologies comprised infectious meningitides/vasculitides in 18 (28%) patients, coagulopathy in 12 (19%) patients and cardioembolism in nine (14%) patients. Multiple aetiologies were present in seven (11%) patients with ischaemic stroke. HIV associated vasculopathy was identified in 13 (20%) patients. The HIV associated vasculopathy manifested either extracranially (seven patients) as total or significant carotid occlusion or intracranially (six patients) as medium vessel occlusion, with or without fusiform aneurysmal dilation, stenosis and vessel calibre variation.
Conclusion: Investigation of HIV infected patients presenting with stroke will determine an aetiology in the majority of patients. In our cohort, 20% of patients demonstrated evidence of an HIV associated vasculopathy.
Statistics from Altmetric.com
Infection with the human immunodeficiency virus (HIV) contributes to an increased risk of stroke.1–4 In South Africa, 5.4 million people out of a total population of nearly 48 million South Africans are infected with HIV, giving a total prevalence of approximately 11% in 2006.5 Isolated reports have identified vasculopathy as a cause of stroke in HIV infected patients.6–12
We report the largest clinical cohort of HIV associated strokes prospectively admitted and investigated by the only tertiary stoke unit in Sub-Saharan Africa. Groote Schuur Hospital is a university teaching hospital serving an open population of approximately 2.9 million persons. The selection bias of our Stroke Unit favours patients from low socioeconomic income groups (more affluent patients with health insurance tend to seek medical care in the private sector), young stroke patients under the age of 46 years (24% of the sample because of referral from other hospitals) and more severe strokes.
Our objective was to describe the nature of stroke in HIV infected patients in clinical practice in a region with a high seroprevalence in the general population and further define HIV associated vasculopathy.
PATIENTS AND METHODS
Patients with confirmed first stroke, infected with HIV and prospectively included in our stroke register between September 2000 and August 2006 were identified and reviewed. All young stroke patients (less than 46 years of age) receive HIV testing after informed consent is obtained, while older patients receive HIV testing guided by their clinical presentation. All patients admitted to our stroke unit undergo a full clinical evaluation and clinically directed investigations. Characteristics recorded were demographic data (including age, gender, ethnicity, socioeconomic status) and risk factors/causes, including hypertension, diabetes, smoking, coagulopathies, peripheral vascular disease, other arteriopathies, alcohol and other substance abuse, previous and intercurrent opportunistic infections and the use of antiretroviral therapy. Investigations in HIV positive patients included: cardiovascular workup (including chest x ray, electrocardiogram and echocardiography), extracranial carotid artery Doppler ultrasonography evaluation, computed tomographic scanning of the brain and CSF analysis and culture. Additional radiological investigations such as MRI and angiography (either digital subtraction angiography, computed tomography angiography or magnetic resonance angiography) and coagulation studies were performed only where clinically indicated. Routine blood investigations included fasting serum lipids, serological testing for syphilis, glucose, electrolytes, creatine, urea and full blood count. Routine serum CD4 count measurements were only undertaken from mid-2003 in our hospital.
A final diagnosis of stroke aetiology was made with the benefit of all available clinical and investigative data. Patients with subarachnoid haemorrhage (managed in the neurosurgical service) and non-stroke intracranial lesions were excluded. Post-mortem studies were undertaken on two patients who died as a direct consequence of stroke.
Fisher’s exact test was used to assess the statistical differences in stroke risk factors, pathological types, aetiology and post-stroke complications. The Student’s t test was used to determine the statistical difference between the mean CD4 counts in patients with vasculopathy and the difference between mean Rankin scores in patients with post-stroke complications.
Ethics approval for the stroke register was obtained from the Research Ethics Committee of the University of Cape Town’s Faculty of Health Sciences. All patients undergoing HIV testing were required to give informed consent.
RESULTS
Demographics
Of the 1087 patients admitted to our stroke unit, 67 (6.2%) were identified as HIV infected. Mean age of the HIV infected stroke patients was 33.4 years (range 19–76) while the mean age of the patients not determined to be HIV infected was 64.0 years (range 17–96). In the total cohort, 266 (24%) patients were less than 46 years of age. Of the 67 HIV infected patients, 61 were less than 46 years (91%), making the HIV positive stroke patients a predominantly young stroke population. The female to male ratio was 1.9:1 for those with HIV infection and 1.3:1 for those without.
Stroke risk factors
Risk factors for stroke in the young HIV positive and HIV negative population groups are shown in table 1. None of the patients in our cohort were intravenous drug abusers.
Recent or intercurrent infection as a risk factor for stroke was demonstrated significantly more commonly in the HIV positive young stroke group (odds ratio (OR) 6.4, 95% confidence interval (CI) 3.1 to 13.2). Intercurrent or recent (within 3 months) opportunistic infections were present in 25 (37%) of the cohort and included: tuberculosis (16 patients), varicella zoster (three patients), pneumocystis pneumonia (three patients), cryptococcal meningitis (two patients) and Kaposi’s sarcoma (one patient).
HIV disease parameters
First ever stroke was the clinical event resulting in the initial diagnosis of HIV infection in 28 (42%) patients. CD4 counts were available in 48 patients (72%), with 22 (46%) having counts below 200 cells/μl and 26 (54%) maintaining CD4 counts of greater than 200 cells/μl. Only eight (12%) of the 67 patients were receiving antiretroviral therapy.
Stroke pathological and clinical subtypes
Cerebral infarction occurred in 64 (96%) of the HIV positive patients and intracerebral haemorrhage in three (4%). The proportion of intracerebral bleeds was not different from that of the total stroke population (p = 0.29) in our register.
Ischaemic stroke syndromes in the HIV positive cohort comprised: lacunar stroke (n = 13), partial anterior circulation stroke (n = 33), total anterior circulation stroke (n = 11), posterior circulation stroke (n = 7) and venous occlusion (n = 1). In two patients, workup was incomplete and three patients had involvement of both anterior and posterior circulations.
Stroke aetiology
The aetiology of the intracerebral haemorrhages was hypertension in all three patients. Table 2 shows the aetiology of the 64 patients with ischaemic infarcts. In seven (11%) of the patients with ischaemic infarct, there were multiple possible aetiologies.
Cardioembolism as a cause of cerebral infarction was significantly less common in HIV positive young stroke patients (10%) compared with HIV negative young stroke cases (23%) (p = 0.028).
Investigation for coagulopathy showed that low levels of protein S were present in six (24%) of the 25 patients and low protein C levels in two (8%) of the 25 patients who underwent testing. Anticardiolipin antibodies were measured in 37 patients and found to be normal in 10 (27%), weakly elevated in nine (24%) and significantly elevated in 18 (49%). In the young stroke group, HIV positive patients were significantly more likely to have elevated anticardiolipin antibodies than HIV negative patients (p = 0.002).
Compared with patients not infected with HIV in the stroke register, HIV positive stroke patients experienced significantly more inpatient confirmed deep venous thrombosis (four episodes compared with 13 episodes; p = 0.020). There was no significant difference between these groups for stroke severity at 1 week, with mean Rankin scores of 4.0 in the HIV positive group and 4.2 in the HIV uninfected group (p = 0.70). For the other inpatient post-stroke complications, including death, there was no difference between HIV positive and uninfected patients.
HIV associated vasculopathy
Seven patients (11%) were identified with an extracranial non-aneurysmal vasculopathy for which no obvious cause could be found. This manifested clinically as either a total or significant occlusion of the extracranial carotid artery/carotid bifurcation (fig 1). Autopsy was performed on a 27 year old male who died from a malignant middle cerebral artery syndrome following occlusion of the right extracranial internal carotid artery. Multiple sections of the neck vessels were taken. Sections of the right carotid artery confirmed occlusion of the lumen by thrombus. Sections of the bifurcation showed advential fibrosis with neovascularisation and lymphoplasmacytic infiltrate. The media and intima showed infiltration by neutrophils with nuclear fragmentation present in the intima (fig 2). There was intimal fibrosis and degeneration of the inner half of the media with myocyte atrophy and fragmentation of the internal elastic lamina. There were macrophages in all layers of the vessel wall. Immunoperoxidase stains showed the inflammatory infiltrate to be positive for neutrophil elastase, CD3, CD8 and CD68. CD20 and P24 were negative. Stains for organisms were all negative.


Six patients (9%) had radiological evidence of an intracranial vasculopathy for which no cause could be found. In the group of young patients with stroke who were not HIV positive, a similar vasculopathy was not identified on angiography. The intracranial vasculopathy in the HIV positive patients was characterised as medium vessel occlusion with or without fusiform aneurysms, stenosis and vessel calibre variation by angiography (figs 3–5). The predominant vessels involved were the circle of Willis and the first and second divisions of the anterior, middle and posterior cerebral arteries. Autopsy obtained on one of our patients with this vasculopathy has been published, and demonstrated widespread intracranial vascular degenerative ectasia with superimposed thrombosis.6

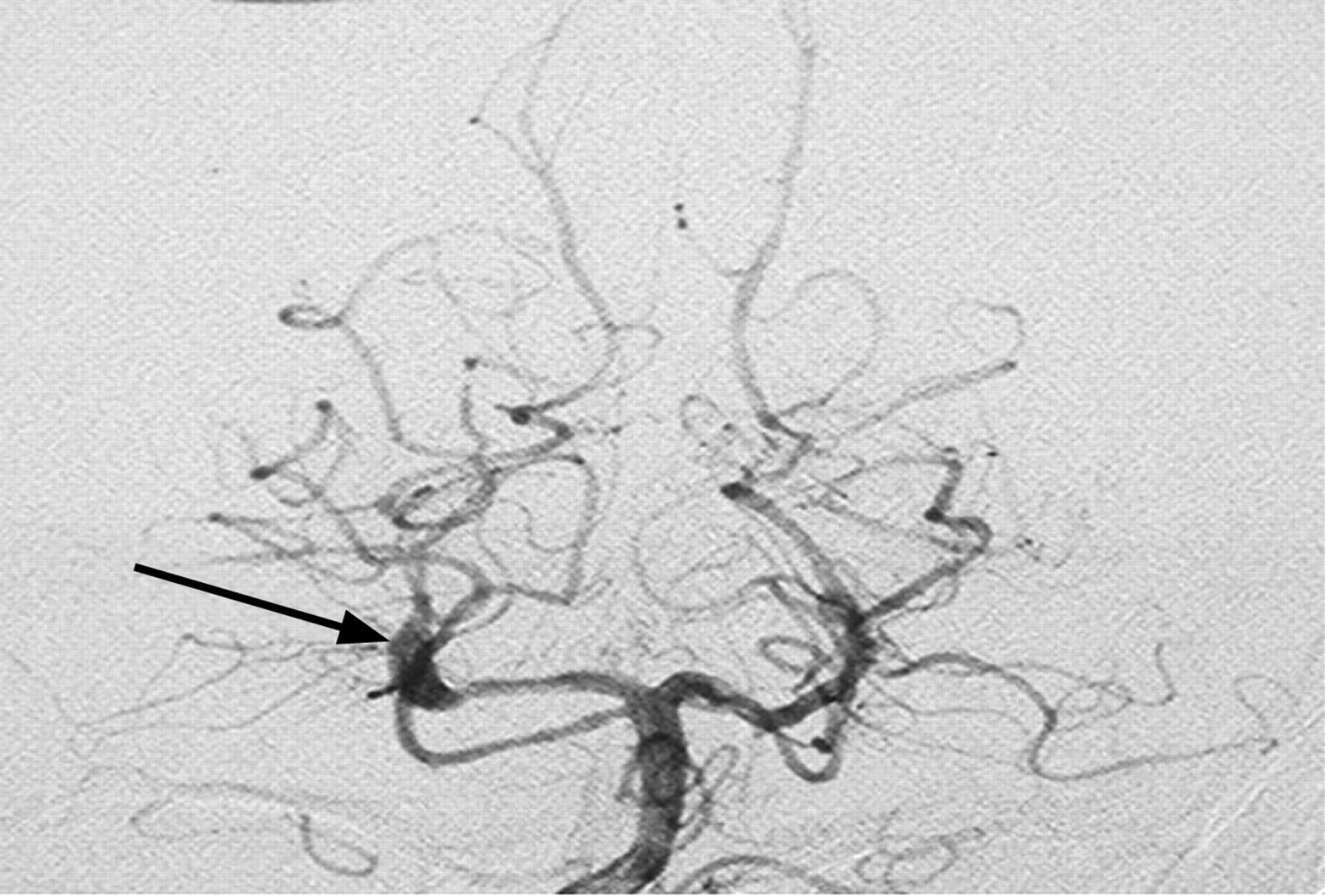

{kind=link}
{kind=link}
{kind=link}
{kind=link}
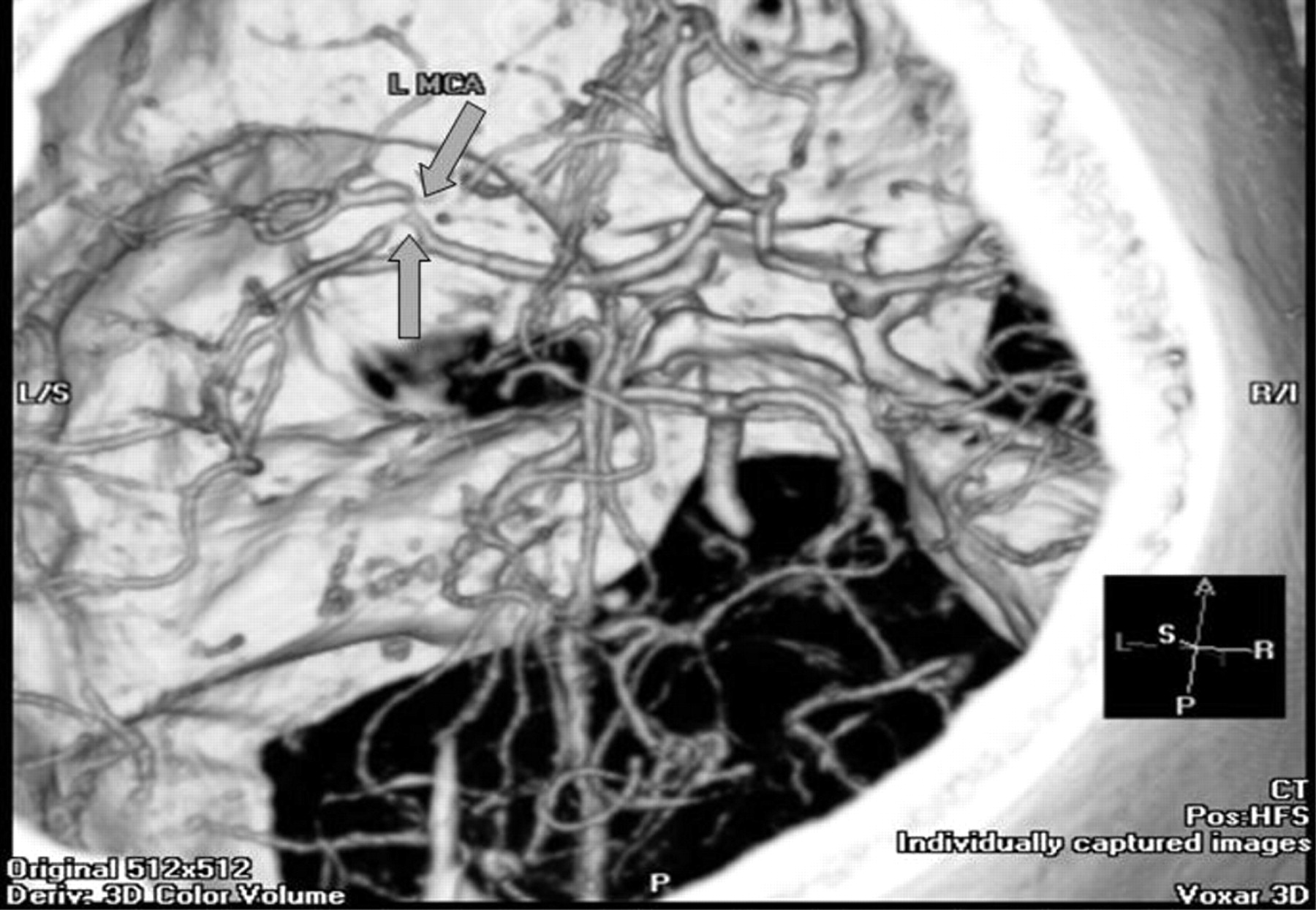{kind=link}
In patients identified with extracranial vasculopathy, five of the seven patients had recorded CD4 counts which ranged from 370 to 533 cells/μl (mean 330 cells/μl). In the intracranial vasculopathy group, six patients had recorded CD4 counts, with a range of 14–277 cells/μl (mean 102 cells/μl). Patients with extracranial vasculopathy demonstrated a significantly preserved CD4 count (>200 cells/μl) compared with patients with intracranial vasculopathy (p = 0.0033).
DISCUSSION
In our stroke unit, HIV associated stroke affected a young stroke population with a risk factor profile that differed from the HIV negative young stroke population in that hypertension, diabetes, hyperlipidaemia and smoking were not significant risk factors. The burden of HIV associated infectious disease was evident in our cohort, with one-third of our patients having experienced a recent or intercurrent opportunistic infection. Twelve per cent of our HIV patients were receiving antiretroviral therapy. This therapy became increasingly available in South Africa from mid-2004. All of our patients on antiretroviral therapy had commenced therapy less than 6 months prior to the date of stroke. A large study in a very different population group has demonstrated an association with antiretroviral therapy and an increased risk of cardiovascular and cerebrovascular events. This risk increases over time but is evident within the first year of therapy.13
The incidence of intracerebral haemorrhage of 4% was similar to other published series of HIV positive strokes patients, which demonstrated incidences of 6–11%.4 14 15
A probable cause of cerebral infarction was found in 52 of the 64 patients (81%). This is similar to the 85% reported in a comparable but smaller cohort.14 Infections (see table 2) were the most common cause in our cohort of HIV positive stroke patients, accounting for 28% of ischaemic strokes, which is similar to previously published smaller cohorts.4 14
Protein S deficiency has been recently recognised as a epiphenomenon of HIV infection with no recognised relation to stroke.16 This casts doubt on the reported aetiological association with stroke in previously reported studies which attributed this as causal in 20–51% of infarcts.4 14 Coagulopathy attributed to the presence of elevated anticardiolipin antibodies was present in 18 (28%) patients with infarcts. These antibodies have been reported to occur in up to half of patients infected with HIV and correlate highly with the presence of perfusion defects on single positron emission computed tomography scanning.17
HIV testing was systematically performed only in stroke patients who were younger than 46 years; this may have introduced bias in the mean age of the HIV positive stroke patients.
HIV associated vasculopathy
This poorly defined vasculopathy has been reported in adults as involving either large or medium extracranial or intracranial arteries.6–12 15 The extracranial large arteries may manifest with both aneurysmal and non-aneurysmal disease.7 Similarly, the intracranial vasculopathy may manifest with both aneursymal and non-aneurysmal lesions, as seen in our study. In addition to large and medium vessel involvement, an intracranial small vessel vasculopathy has been described in an autopsy series of patients that died with AIDS.18 This is largely an asymptomatic vasculopathy and is characterised by hyaline small vessel wall thickening, perivascular space dilatation, rarefaction and pigment deposition with vessel wall mineralisation and occasional perivascular inflammatory cell infiltrates, and is associated with microinfarcts.18 This latter vasculopathy is difficult to define clinically. The cause and mechanism of the various HIV associated vasculopathies is poorly understood.
In our cohort, patients with extracranial vasculopathy (all non-aneurysmal) had preserved CD4 counts (mean 479 cells/μl), suggesting that this entity could occur as a consequence of an immunocompetent vasculitis. Histology obtained from one patient in our sample was similar to that published previously showing a leucocytoclastic vasculitis of the vaso vasorum with relatively minimal intimal changes.7
In contrast, the intracranial vasculopathy (including both aneurysmal and non-aneurysmal disease) in our patients occurred in immunocompromised patients with low CD4 counts (mean 112 cells/μl). The vaso vasorum, which has been postulated as pivotal in the pathogenesis of the extracranial HIV associated vasculopathy, is not present in the intracranial circulation.7 Post-mortem histology obtained from one of our patients with the intracranial aneurysmal vasculopathy showed intimal hyperplasia, fibrosis and thickened beaded internal elastic lamina with fragmentation, suggesting that the focus of the insult in the intracranial vasculopathy is the intima.6 Immune activation in response to transendothelial migration by HIV strains that have a cerebral tropism is a proposed initiating event.19 Subsequent aneurysmal disease progression may be augmented by dynamic vascular remodelling in response to normal pulsatile shear stress, growth factor and cytokines.20 Intercurrent opportunistic infections may contribute to the production of the necessary cytokines that drive this process.6 Certain infections such as varicella zoster are known to cause vasculitis.
CONCLUSION
To our knowledge, this study represents the largest prospective cohort of stroke in HIV positive individuals. In the majority of individuals, thorough investigation revealed a probable cause of stroke. This emphasises the need for a comprehensive workup in the stroke patient who is HIV positive. The occurrence of stroke in the younger patient who is HIV positive should not preclude a comprehensive workup, as HIV status may be incidental, particularly in a population with a high HIV seropositive prevalence in the general population.
In 20% of HIV positive patients who presented with stroke, there was radiological evidence of intracranial (9%) or extracranial (11%) vasculopathy for which no other cause could be determined. The characteristic radiographic appearance of the intracranial aneurysmal vasculopathy was not seen, without a cause, in any other HIV negative patient in our stroke register. A number of possible mechanisms have been implicated in the pathogenesis of this condition but the exact role of HIV in the aetiology of the condition remains uncertain.
REFERENCES
Footnotes
Competing interests: None.
- Abbreviations:
- HIV
- human immunodeficiency virus