Article Text

Abstract
Objectives: To evaluate a new three dimensional (3D) MRI protocol for the reliable detection of aortic high risk plaques compared with transoesophageal echocardiography (TOE) and to test the reliability of additional MRI in stroke of undetermined aetiology.
Methods: 74 acute stroke patients were examined by both TOE and MRI at 3 Tesla with special regard to aortic high risk plaques (ie, ⩾4 mm, superimposed thrombi). ECG synchronised pre- and post-contrast T1 weighted 3D imaging (spatial resolution ∼1 mm3) covering the thoracic aorta was employed. In plaques ⩾3 mm, additional two dimensional T2 imaging and time resolved (CINE) imaging sequences were performed. Aetiology of brain ischaemia was classified according to modified TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria. Aortic high risk embolic sources detected by MRI in patients with cryptogenic stroke were evaluated.
Results: Differences in maximum aortic wall thickness for TOE and MRI were not statistically significant for all aortic segments. The overall number of high risk plaques detected by MRI (n = 74) was substantially higher compared with TOE (n = 47). Most noticeably, MRI identified aortic high risk pathologies in 8/26 (30.8%) patients with cryptogenic stroke after standard diagnostics, including TOE (n = 2: dissection or thrombus; n = 6: plaques ⩾4 mm).
Conclusions: Our results demonstrate the feasibility of this 3D MRI protocol for the reliable detection of aortic high risk plaques in acute stroke patients. Because of improved visualisation of the aortic arch and the detection of additional embolic sources not seen by standard diagnostics, this novel technique may become a valuable tool for future patients with cryptogenic stroke.
Statistics from Altmetric.com
Transoesophageal echocardiography (TOE) is the current reference standard for the detection of cardiac high risk sources of cerebral embolism, such as aortic plaques ⩾4 mm and aortic thrombi.1 In patients with stroke of undetermined aetiology, these pathologies are by far the most frequent cardiac high risk sources detected by TOE2 and their prevalence is comparable with that of carotid artery stenosis and atrial fibrillation.3 Although the complication rate during TOE is low,4 the procedure is semi-invasive. Furthermore, visualisation of both the distal ascending aorta and aortic arch is strongly reduced by air artefacts and insonation angles. Thus diagnostic accuracy is limited and the exact number of embolic sources overlooked by TOE is currently unclear.3
Previous MRI studies on detection of atherosclerotic plaque were conducted on 1.5 Tesla systems only, and were limited with respect to spatial resolution, anatomical coverage and signal-to-noise ratio5–7 while 3 T MRI improved characterisation of plaques ex vivo in a recent study.8 Also, these studies focused on the detection and composition of plaques either in the descending aorta or in the carotid arteries comparing MRI with TOE or histopathological examination.9–13 However, in patients with cardioembolic stroke, the aortic arch (ie, the origin of the brain supplying arteries) is of high clinical interest. MRI of this region is still challenging as examination is strongly hampered by artefacts due to vessel motion and respiration.
In general, previously reported two dimensional (2D) MR studies suffered from incomplete coverage of the aortic segment of interest. For reliable acquisition of the aortic arch, the use of a dedicated TOE–MRI coil was reported.11–14 However, reduced patient comfort and limited availability of TOE–MRI coils restrict clinical application to experimental studies. More conventional MR imaging using 2D slices positioned perpendicular to the curved aortic arch was successfully performed in animal models of induced atherosclerosis and in a recent patient study.15–17 However, high resolution MRI at 3 T for the detection of atheroma with three dimensional (3D) coverage of the thoracic aorta has not been reported to date. Also, the reliability of additional aortic MRI has not yet been investigated systematically in acute stroke patients.
The aim of this study was therefore to test the agreement between 3D MRI at 3 T and TOE. Furthermore, we hypothesised that because of the improved visualisation of the aortic arch and the detailed retrospective data evaluation, MRI would be equivalent or even superior to TOE in detecting aortic pathologies, in particular in patients with cryptogenic stroke despite extensive clinical routine diagnostics.
PATIENTS AND METHODS
Study population
Seventy-four non-consecutive patients hospitalised in our stroke unit fulfilled the inclusion criteria: age 17–85 years, acute brain ischaemia, performance of TOE examination, no contraindications to 3 T MRI examination. The prospective study was approved by the local ethics committee and written informed consent was obtained from all participants. Following recommendations of a previous study,2 TOE was scheduled if routine diagnostics (brain MRI including MR angiography or CT, or both, transthoracic echocardiography, ECG, extra-/intracranial ultrasound) could not clarify stroke aetiology with a high level of confidence. In addition, TOE was performed individually in younger patients to screen for other cardiac sources, in patients with internal carotid artery stenosis, to exclude an additional high risk embolic source such as complex aortic plaques, and in patients with a history of atrial fibrillation but sinus rhythm in the actual Holter-ECG. Patients underwent both TOE and MRI examinations within 5 and 6 days (median) after admittance to our hospital. Median time interval between TOE and MRI examinations was 1 day.
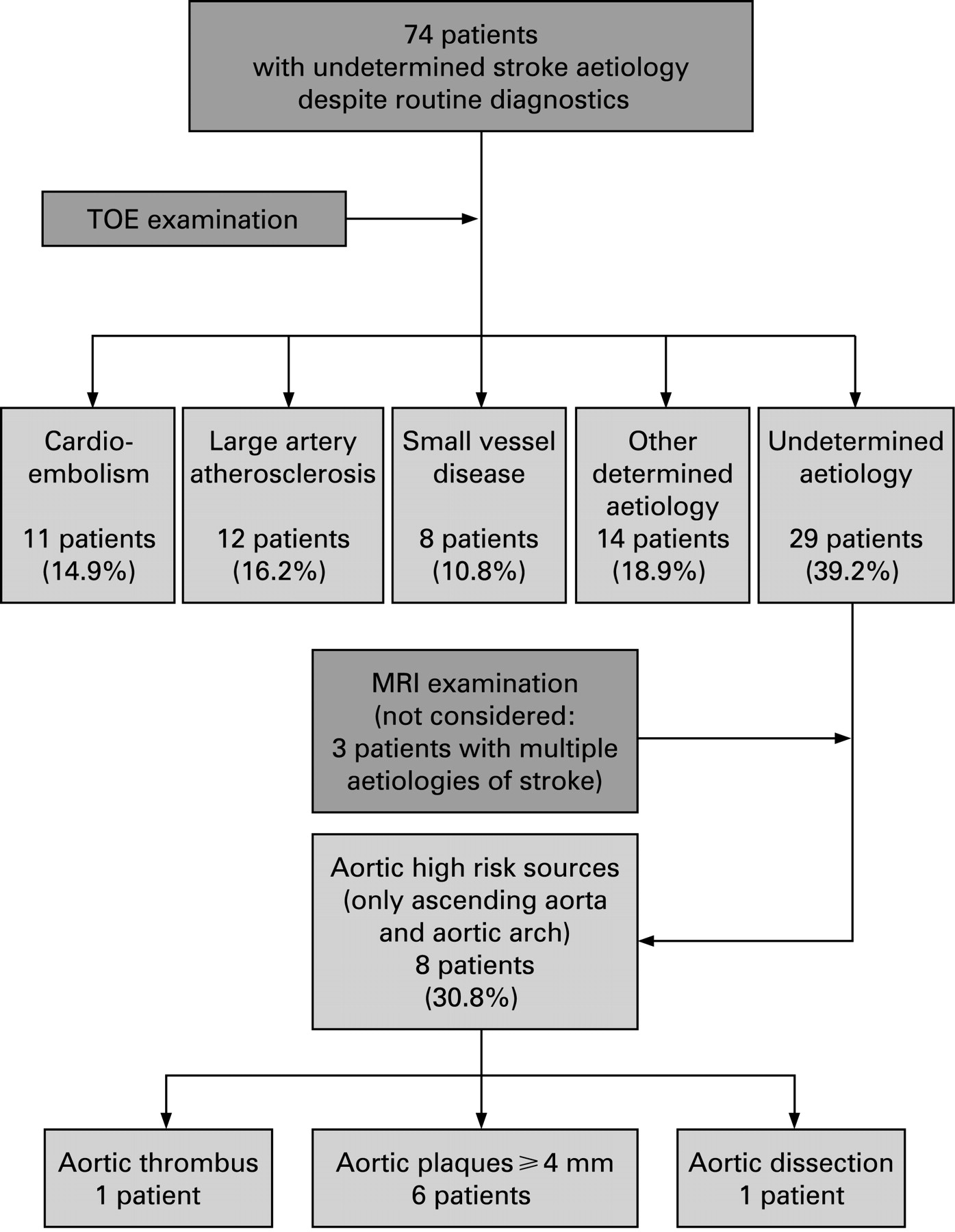
Infarct aetiology was classified according to modified TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria18 taking the results of both routine diagnostics and TOE into account. With respect to additional TOE findings, stroke was classified as “cardioembolic” if left atrial appendage thrombus, spontaneous echo contrast or left atrial appendage flow velocity <30 cm/s was found. Stroke was defined as “other determined aetiology” if aortic plaques ⩾4 mm, aortic thrombi or dissection was detected by TOE. Patients with two or more probable sources of stroke were defined as “determined”. Thus “undetermined” (ie, cryptogenic) stroke was reserved for those without a clarified aetiology despite complete diagnostics, and aortic high risk sources additionally detected by MRI in the ascending aorta or the aortic arch were further evaluated in this subgroup (fig 1). Embolic brain ischaemia was defined as present in patients with a typical pattern on brain imaging (ie, grey matter involvement: disturbed diffusion weighted imaging on MRI or hypodense lesion without clear delineation in CT) and/or characteristic clinical signs (amaurosis fugax, central retinal artery occlusion or cortical signs such as aphasia, neglect, hemianopsia). Cardiovascular risk factors were defined as described previously.2

TOE imaging protocol
TOE examinations were performed by one experienced senior echocardiographer using a 5 MHz multiplane probe (ATL, HDI 5000, Bothell, USA), recorded on videotape and reviewed offline blinded to the MRI results. Three predefined aortic segments (ie, ascending aorta, aortic arch and descending aorta) were imaged in cross sectional and longitudinal orientation. Evaluation criteria included: (a) maximum aortic wall thickness (AWT) (ie, intima–media thickness at sites free of plaques); (b) number and location of plaques (ie, irregular and circumscribed thickening of the intima with increased echogenicity19) per aortic segment, differentiation into low risk (ie, <4 mm) and high risk plaques (ie, ⩾4 mm in thickness or presence of ulcerations or mobile components) and exact localisation, as derived from a cross sectional view; and (c) detection of aortic thrombi defined as laminated deposition along the intimal surface with variable echogenicity which may be associated with mobile lesions.20 21
MR imaging protocol
All examinations were performed on a 3 T system (TRIO; Siemens Medical Solutions, Erlangen, Germany) equipped with an 8 channel phased array body coil. Plaque imaging was performed using a T1 weighted rf-spoiled and fat saturated 3D gradient echo sequence. Three dimensional volumes were carefully adapted to cover the aortic arch and the ascending and descending aorta (voxel size = 0.8×1.1×1.1 mm3; field of view (FOV) = 350×252 mm2; echo time (TE)/repetition time (TR) = 1.7/5.1 ms; flip angle = 20°). To minimise motion induced blurring, data acquisition was executed using ECG gating with a short diastolic data acquisition window (158 ms) within the cardiac cycle.
Respiration control by navigator gating allowing for data acquisition during free breathing and minimisation of breathing artefacts was performed as described previously.22 Retrospectively, ECG gated 2D time resolved (CINE) gradient echo imaging (voxel size = 1.6×2.1×5 mm3; temporal resolution = 26.8 ms; FOV = 400×300 mm2; TE/TR = 2.0/3.4 ms; flip angle = 15°) normal to the ascending aorta was performed at end expiration to individually determine the temporal frames within the cardiac cycle with the least vessel motion. The data acquisition window for 3D imaging was then set to match the period with no or only minor aortic motion.
During the MRI examination, data were analysed using a multiplanar reformat tool available on the scanner software (Siemens WIZARD; Siemens Medical Solutions). Consensus reading of two experienced observers was performed to identify plaques ⩾3 mm. To optimise scan and data evaluation efficiency, data acquisition was split into two axial 3D volumes 3.52 cm thick in order to evaluate the first 3D data volume while the second acquisition was performed.
In the presence of aortic plaques ⩾3 mm in thickness, contrast agent (gadobenate dimeglumine, Gd-BOPTA chelate, Multihance; Altana Pharma, Konstanz, Germany) was injected as a single dose (0.1 mmol/kg body weight, injection rate 3–4 ml/s) and time resolved contrast enhanced 3D MR angiography (tr-CE-MRA) was performed. Imaging parameters included parallel imaging (GRAPPA, acceleration factor = 423) and partial Fourier acquisition along the phase and slice encoding direction (partial Fourier factor = 6/8). The combination with view sharing along the temporal domain (TREAT, double update rate of central k-space24) resulted in a reconstructed voxel size of 1.3×1.9×1.5−1.8 mm3 and an effective (reconstructed) temporal update rate of 2.7–3.0 s (FOV = 400×400 mm2; TE/TR = 0.8/2.0 ms; flip angle = 15–25°). Twenty T1 weighted 3D data volumes were acquired in the sagittal oblique or coronal orientation covering the entire thoracic aorta.
To increase the reliability of plaque detection by improved signal-to-noise ratio, T1 high spatial resolution 3D plaque characterisation was repeated after administration of contrast agent. Breath held T2 weighted (voxel size = 1.5×2.1×5.0 mm3; FOV = 340×276 mm2; TE/TR = 86.0 ms/2×RR; flip angle = 90−(160−180)°) and time resolved (CINE) images were acquired at slice positions corresponding to previously detected plaque locations ⩾3 mm.
MR data analysis
Based on consensus reading, MRI data were evaluated by two experienced readers blinded to patient demographics and TOE data. Image quality of additionally acquired T2 weighted images was categorised as: low = severe blurring of the aortic wall and insufficient black blood saturation, reliable assessment of the vessel wall impossible; moderate = minor blurring of the aortic wall and incomplete black blood saturation, reliable assessment of the vessel wall possible; and high = exact delineation of the aortic wall and complete black blood saturation, assessment possible with a high level of confidence. Aortic plaque was defined as a circumscript thickening of the aortic wall. Maximal extent of plaque involvement was evaluated for each segment of the aorta using all available pre- and post-contrast MR images. The outlets of the great supra-aortic arteries served as landmarks for the description of exact plaque localisation within the 3D data volume. Maximum plaque thickness (AWT) was measured by electronic callipers in the transverse view as the distance between the aortic border and the point of greatest luminal protrusion (see also fig 2). The largest plaque of each aortic segment (ascending, arch and descending) was measured and considered for further evaluation. Aortic thrombi were defined as mobile structures floating within the bloodstream in the transverse view in time resolved CINE imaging with hypointense signal in CINE and T1 images without contrast enhancement.

MR plaque analysis was performed using a multiplanar reformat tool (J-Vision; Tiani Medgraph AG, Innsbruck, Austria) to navigate within the 3D data set and generate pre- and post-contrast images of aortic plaques in planes normal to the aorta. For further orientation, the exact location of individual cut planes could be visualised within a maximum intensity projection of the arterial phase of the tr-CE-MRA data (fig 1). Image location and angulations were carefully fine tuned by visually comparing anatomical landmarks in reformatted pre- and post-contrast images.
Comparison of TOE and MRI data
Aortic segments were defined as follows: (1) ascending aorta: segment from the aortic bulb onto the outlet of the brachiocephalic trunk; (2) aortic arch: the following segment including the outlet of the left subclavian artery; (3) descending aorta: segment distal to the outlet of the left subclavian artery. Following a previous study protocol, localisation and morphology of aortic plaques found in TOE and MRI were documented on two separate sketches.25 As a result, we obtained from all data recorded by TOE and MR a total of 222 segments from our 74 patients. AWT, absolute number of plaques of any size and especially those ⩾4 mm thick or with superimposed thrombi, detection of inflammatory wall disease or dissection membrane in each aortic segment were considered for classification of TOE and MRI findings in each patient.
Statistical analysis
Data are presented as mean (SD) for continuous variables. To detect statistically significant differences between continuous variables, paired t tests were applied. All significance tests were two sided comparing corresponding aortic segments in TOE and MRI and using a significance level of 5%. For comparison of complex aortic plaques found in TOE and MRI, kappa coefficients (κ) for each aortic segment were calculated. Comparison between TOE and MRI measurements for maximum plaque thickness was evaluated using the Bland and Altman approach26 by calculating the mean (d) and SD (ςd) of the difference. From these data, the limits of agreements (d-2ςd and +2ςd) were calculated. All analyses were performed by SPSS statistical package (V.14.0).
RESULTS
Basic findings
Baseline demographic data are given in table 1. Distribution of stroke subtypes is shown in fig 1; embolic brain ischaemia was found in 57 of 74 patients (77.0%). Most noticeably, MRI detected an additional aortic high risk source of brain embolism in 8/26 (30.8%) patients with stroke of undetermined aetiology (ie, no conclusive findings in routine diagnostics or TOE). Nineteen of 26 (73.1%) patients with cryptogenic stroke suffered embolic brain ischaemia.
MRI protocol
In all patients, the entire imaging protocol was successfully performed within 48.9 (12.5) min (range 24–88). Total scan time for high spatial resolution for each 3D pre- or post-contrast T1 data volume was 6.2 (1.7) min (range 3–12) depending on heart rate and navigator efficiency (30–60%).
MRI and TOE results: images
Image quality for both pre- and post-contrast MRI and maximum intensity projections of tr-CE-MRA at maximum arterial contrast is illustrated in comparison with TOE in fig 2. In general, good image quality in T1 weighted sequences was achieved, particularly after application of contrast agent and only minor blurring and ghosting artefacts due to motion were appreciated and obtained in all other patients. Two dimensional T2 imaging often suffered from unsatisfying image quality (low signal-to-noise ratio, insufficient black blood saturation) and could thus be considered in only part of all examined patients. Overall, 118 T2 weighted measurements of the aorta were performed in 44 patients. Image quality was graded low in 51/118 (43.2%), moderate in 35/118 (29.7%) and high in 32/118 sequences (27.1%). T2 imaging proved useful in a patient with type B aortic dissection (fig 3).

Comparison of TOE and MRI data
The wall of the ascending aorta and aortic arch was not reliably assessable by TOE because of limited visualisation in 11/74 (14.9%) and 45/74 patients (60.8%). Overall, TOE detected aortic high risk plaques in 23/74 (31.1%) compared with 37/74 (50%) patients, as identified by MRI (p = 0.029). Also, the absolute number of aortic plaques ⩾4 mm and thrombi detected by TOE (n = 47) was lower than in MRI (n = 74) (table 2, fig 4).

Differences in maximum AWT for TOE and MRI were not statistically significant (see table 2). AWT and number of aortic high risk plaques increased from the ascending to the descending aorta. Agreement between MRI and TOE for the detection of aortic segments with plaques ⩾4 mm or aortic thrombi was moderate to substantial (0.90>κ>0.50), as indicated by the kappa coefficients in table 2. A detailed interindividual comparison of findings for all patients is provided by the Bland–Altman plot in fig 5. Results show limited agreement of MRI and TOE measurements in direct comparison. The mean (SD) of the difference was small, whereas the differences between MRI and TOE were relatively wide in comparison with the mean, with the difference increasing with the mean of maximum aortic wall thickness. For the 95% of the differences within the limits of agreement there was no indication of a systematic error.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Further data analysis revealed that in only four patients MRI overlooked aortic high risk plaques detected by TOE: in two patients the atheroma ⩾4 mm was located outside the predefined MRI 3D data volume (ie, in the very proximal ascending or distal descending aorta), in another patient a 4.4 mm thick plaque in the arch was not detected by MRI and in the fourth subject measurements of AWT in MRI and TOE were 3.9 and 4.0 mm, respectively. Additional CINE imaging allowed for the detection of a mobile descending aortic thrombus, as confirmed by TOE in one patient. Another mobile thrombus located at the anterior wall of the aortic arch as well as a dissection of the aortic inner curvature not visible in TOE could be clearly identified in the transverse view by MRI CINE imaging. Concordantly, aortic dissection in two patients who had received partial aortic graft repair could be detected by both diagnostics. Inflammatory vessel disease was not observed in any patient.
DISCUSSION
In our study, plaque detection in the thoracic aorta using high spatial resolution 3D MRI at 3 T was successfully demonstrated in 74 acute stroke patients in direct comparison with TOE. Although the agreement between MRI and TOE using Bland–Altman analysis was poor, further evaluation suggests that MRI may be more reliable than TOE for the detection of high risk aortic diseases in stroke patients: the number of high risk plaques found by MRI was significantly higher compared with TOE which can only partly be explained by the fact that MRI measures all layers of the aortic wall whereas TOE considers intima–media or plaque thickness. The spatial resolution of MRI in this study was not sufficient to fully resolve the thin adventitia which may result in partial volume effects and offer a potential explanation for overestimation. Nevertheless, overestimation was relatively small such that comparing MRI and TOE provided a valid test for evaluation of the reliability of MRI. In contrast with 3D MRI, TOE, the currently best available reference method, failed to reliably assess the aortic arch because of insufficient visualisation in half of the patients. Therefore, we believe that both the apparent poor agreement of both methods in the Bland–Altman analysis and the higher number of aortic pathologies found by MRI is particularly due to improved aortic coverage and visualisation than to measurement of “false positive” pathologies. Our findings emphasise the need for a method such as 3D MRI. Previous studies confirmed that TOE underestimates the true number of plaques due to limited visualisation of the aortic arch.3 27 However, a detailed analysis of the number of patients with inappropriate visualisation of the arch in TOE has not been reported.
Most noticeably, additional aortic high risk sources of brain ischaemia were detected by MRI in almost 30% of patients with stroke of undetermined aetiology after routine diagnostics, including TOE. The significance of these additional MRI findings was confirmed by the high number of embolic strokes in this subgroup. Thus our findings suggest that high field 3D MRI may increase diagnostic accuracy for the detection of aortic high risk pathologies, especially in patients with cryptogenic stroke. Although the increased risk of cerebral embolisation in patients with severe aortic plaques is well documented, the optimal treatment has not yet been established by prospective and randomised trials and such patients currently receive only antiplatelets and statins.28 However, the future value of aortic 3D MRI may increase after the results of the ongoing Aortic arch Related Cerebral Hazard (ARCH) trial comparing aspirin plus clopidogrel versus warfarin for the optimal treatment of aortic high risk plaques.
It is uncertain whether a cut-off value of ⩾4 mm used to identify high risk plaques on MRI is similar to that on TOE and whether those plaques carry a risk similar to those identified on TOE. Thus, next to the definition of cut-off values for MRI, larger cohorts of stroke patients need to be examined in order to evaluate the role of aortic atherosclerosis in more detail by also detecting those plaques in the ascending aorta and proximal arch that are often overlooked by TOE. High resolution spiral 3D CT yielding complete coverage of the aorta could be an alternative future reference method but next to general disadvantages such as radiation exposure and contrast agent containing iodine, plaque morphology can only to a certain extent been categorised.29
To date, only a few in vivo studies have compared MRI and TOE measurements for the evaluation of aortic plaques: Shunk and colleagues30 compared TOE with transoesophageal MRI but such MRI coils are not widely available and are also semi-invasive. Two other studies included only a few subjects and MRI was not performed in acute stroke patients.9 31 In contrast with Kutz and colleagues31 but consistent with others,9 28 our results demonstrate both the moderate agreement of AWT and comparable reliability for the detection of aortic high risk plaques for both techniques. In contrast with others,5–7 9 16 31 we present a novel MRI protocol at 3 T, providing a 3D data set with high spatial resolution covering the aorta, including the aortic arch, and evaluate its additional diagnostic impact in acute patients with cryptogenic stroke. The definition of individual scan delays, the short diastolic acquisition window and the technique of respiratory navigator gating provided good diagnostic image quality, even in the aortic arch. Pre- and post-contrast imaging was primarily performed to maximise reliability of aortic plaque detection. Furthermore, application of contrast agent allowed for supplementary time resolved CE-MRA, providing additional 3D information on exact plaque location and thoracic vascular geometry which is especially helpful in patients with aortic aneurysm, type A dissection or Takayasu’s arteriitis.
The detailed characterisation of aortic plaque remains challenging: four patients with aortic plaques ⩾4 mm on TOE were not identified by MRI because the plaques were located outside the predefined MRI 3D data volume or thickness was minimally underestimated by MRI. Further optimisation therefore includes coverage of the very proximal ascending aorta and a higher spatial resolution (ie, <1 mm). Individually performed T2 weighted 2D and T1 CINE imaging did provide additional information in patients with dissection and aortic thrombi and point towards the importance of both multi-contrast and functional MR imaging. These sequences were not applied routinely because of the currently low image quality in the aortic arch of most patients and the confined scan time in acutely ill patients. Thus future reduction of total scan time and implementation of robust T2 and additional PD weighted pulse sequences into the MRI protocol may ameliorate diagnostic accuracy and plaque characterisation.7
SUMMARY
The utility and quality of an MR imaging protocol for high spatial resolution 3D examination of aortic high risk pathologies at 3 T was successfully evaluated in comparison with TOE in acute stroke patients. The reasonable expenditure of time for MRI examination and in particular independence from the breath holding capacities of the imaged subjects allow the implementation of this technique even in acute stroke. The high sensitivity of 3D MRI for the detection of aortic high risk plaques makes it a promising tool in patients with contraindications for TOE and particularly in those with cryptogenic stroke despite extensive routine diagnostics. However, before this novel MRI technique can be generally recommended, its diagnostic value needs to be evaluated rigorously at various imaging sites.
REFERENCES
Footnotes
Funding: MM is supported by the Deutsche Forschungsgemeinschaft (DFG), grant No MA 2383/3-1 and the Bundesministerium für Bildung und Forschung (BMBF), grant No 01EV0706.
Competing interests: None.
Ethics approval: The study was approved by the local ethics committee.