Article Text

Abstract
Purpose To assess the relationships of sun exposure history, supplementation and environmental factors to vitamin D levels in multiple sclerosis (MS) patients and to evaluate the associations between sun exposure and MRI measures.
Methods This study included 264 MS patients (mean age 46.9±10 years, disease duration 14.6±10 years; 67.8% relapsing–remitting, 28% secondary progressive and 4.2% primary progressive MS) and 69 healthy controls. Subjects underwent neurological and 3 T MRI examinations, provided blood samples and answered questions to a structured questionnaire. Information on race, skin and eye colour, supplement use, body mass index (BMI) and sun exposure was obtained by questionnaire. The vitamin D metabolites (25-hydroxy vitamin D3, 1, 25-dihydroxy vitamin D3 and 24, 25-dihydroxy vitamin D3) were measured using mass spectrometry.
Results Multivitamin supplementation (partial correlation rp=0.29, p<0.001), BMI (rp=−0.24, p=0.001), summer sun exposure (rp=0.22, p=0.002) and darker eye colour (rp=−0.18, p=0.015) had the strongest associations with vitamin D metabolite levels in the MS group. Increased summer sun exposure was associated with increased grey matter volume (GMV, rp=0.16, p=0.019) and whole brain volume (WBV, rp=0.20, p=0.004) after correcting for Extended Disability Status Scale in the MS group. Inclusion of 25-hydroxy vitamin D3 levels did not substantially affect the positive associations of sun exposure with WBV (rp=0.18, p=0.003) and GMV (rp=0.14, p=0.026) in the MS group.
Conclusions Sun exposure may have direct effects on MRI measures of neurodegeneration in MS, independently of vitamin D.
- Multiple Sclerosis
- MRI
Statistics from Altmetric.com
Introduction and background
Multiple sclerosis (MS) is a degenerative, chronic inflammatory disease of the CNS that causes demyelination, lesion formation and CNS atrophy. The CNS damage in MS results from abnormal immune responses but there is also neurodegeneration and progressive neuronal loss.1 ,2
Latitude is a prominent environmental factor associated with the risk of developing MS, which increases with increasing distance from the equator in both the northern and southern hemispheres. Latitude is an important determinant of sun exposure, and areas at higher latitudes receive less potent ultraviolet radiation (UVR) exposure.3 Climate and seasonal variation also affect UVR exposure. Outdoor temperature and sunny weather are also important determinants of human activities and behaviours that could result in sun exposure. Sun exposure is also being minimised as a consequence of public health education campaigns, which are promoting the use of sun blocking agents in order to reduce the incidence of skin cancer.4 ,5
UVR exerts an immunosuppressive effect on the immune system through multiple mechanisms and has been associated with the risk of autoimmune disease such as MS, type 1 diabetes and rheumatoid arthritis.6 ,7 UVR causes local immunosuppression, resulting in less hypersensitivity reactions. Secondly, it helps limit melatonin secretion, which can modulate T cell proliferation and activity.8–10 More importantly, UVR increases vitamin D production, and vitamin D has been shown to have pleiotropic immunomodulatory activities. There are challenges in assessing the relationship of sunlight exposure to clinical outcomes in MS because disability progression can affect sun exposure. Furthermore, sunlight exposure can affect vitamin D levels, making it difficult to assess which of the two exposures is relevant for modulating pathophysiological mechanisms of brain injury.
Vitamin D levels are dependent on sun exposure because ultraviolet light is required for the first step in the synthesis of vitamin D from 7-dehydrocholesterol in the skin. Several studies have examined the associations of vitamin D with clinical and MRI measures in MS patients. These studies have reported associations with relapse rates.11–14 Adverse disability and disability changes on the Extended Disability Status Scale (EDSS) and the MS Severity Scale are associated with low vitamin D levels.13 ,15 The associations of vitamin D levels with MRI measures in MS patients have been examined but the associations appear more modest.15 ,16
The goal of this study was to assess the interdependencies of sunlight and vitamin D supplementation to vitamin D metabolite levels in MS patients and to evaluate the associations between sun exposure to MRI measures of brain injury in MS.
Methods
Patient population
Study design
Data from an ongoing prospective study of clinical, genetic and environmental risk factors in MS at the MS Center of the State University of New York at Buffalo were used. The University at Buffalo Human Subjects Institutional Review Board approved the study protocol and all participants provided written informed consent.
The study included patients with MS, clinically isolated syndrome (CIS), healthy controls and controls with other neurological diseases. A total of 499 subjects were enrolled, including 289 MS, 21 CIS, 163 healthy controls and 26 subjects with other neurological diseases.
In this analysis, MS patients and controls, aged 18 years and older and those 65 years and under, were included. Children under 18 years of age, subjects over 65 years of age and those with CIS, neuromyelitis optica or other neurological diseases were excluded. Controls without MRI were excluded.
Based on these inclusion and exclusion criteria, we included 264 MS patients and 69 healthy controls: 166 subjects were excluded (21 CIS, 26 other neurological diseases, six neuromyelitis optica, 15 subjects aged <18 years, 16 subjects aged >65 years and 80 healthy subjects without MRI).
Patients and controls underwent neurological and MRI examinations, provided blood samples for genetic analyses and answered questions to a structured questionnaire administered in person by an interviewer.17 The responses were transcribed directly to computer by the interviewer.
Information on race, skin and eye colour, supplement use, body mass index (BMI) and sun exposure was obtained by questionnaire. The sun exposure data were obtained by questionnaire for the preceding 2 years. Subjects were asked to provide information on time of sun exposure from ‘job’, ‘exercise’, ‘leisure’, ‘beach’, ‘sun bathing’, ‘tanning bed’ and ‘other’ activities during the summer and winter months. The cumulative summer and winter sun exposure in days was calculated from the responses. The sun exposure values for summer and winter were binned into four groups using observed quartiles. Buffalo, a city in the western part of New York State, USA, is located at 42°54′17″N latitude and 78°50′58″W longitude.
Subjects provided yes–no answers on whether they had consumed multivitamin, vitamin D and calcium plus vitamin D supplements. The responses to vitamin D and calcium plus vitamin D supplements were pooled into a single variable.
Subjects also provided information on eye colour, which was recorded on an ordinal scale (level 0: light blue, grey or green; level 1: blue, grey or green; level 2: dark blue, grey or green; level 3: brown). Likewise, skin colour in an unexposed area of the body was recorded on the 6 level Fitzpatrick Scale.
Vitamin D and vitamin D metabolites
Vitamin D metabolites (25 hydroxy vitamin D3 (25(OH)VD3); 1, 25 dihydroxy vitamin D3 (1, 25(OH)2 VD3); and 24, 25 dihydroxy vitamin D3 (24, 25(OH)2 VD3)) were measured using liquid chromatography–tandem mass spectrometry methods with stable isotope labelled internal standards, as published previously.18
The raw 25(OH)VD3, 1, 25(OH)2 VD3 and 24, 25(OH)2 VD3 levels were logarithm transformed and deseasonalised using sinusoidal regression. The month of blood draw was used as the independent variable in the sinusoidal regression. The form for the regression equation for 25(OH)VD3 was:
T represents the month of blood draw (January=1 to December=12 scale with the 0.5 rounding values to the mid-point of the month). The a0, a1, a2 are model parameters and were estimated from the data using non-linear regression. The deseasonalised values of log 25(OH)VD3 were obtained by adding the residuals to the model mean a0. The deseasonalised values of 25(OH)VD3 were calculated via the anti-log transformation. The deseasonalised values of 1, 25(OH)2 VD3 and 24, 25(OH)2 VD3 were obtained from the raw 1, 25(OH)2 VD3 and 24, 25(OH)2 VD3 levels using the same methodology.
HLA genotyping
HLA DR*1501 status was obtained by genotyping DNA from peripheral blood for rs3135005 using an allele discrimination kit (Assays-on-Demand genotyping kit; Applied Biosystems, Redwood City, California, USA).
MRI acquisition and analysis
MRI acquisition protocols and analysis methods are summarised in the online supplementary data. We assessed measures of T2 and T1 lesion volume (LV), and normalised whole brain volume (WBV) and grey matter volume (GMV). In MS patients, the mean time difference between blood sampling and MRI was 30.6 days (95% CI 17.4 to 43.8 days; median 0 days (25th–75th IQR −26 to –56 days)). In controls, the mean time difference was −14.9 days (95% CI −6.6 to −23.2 days).
Statistical analysis
The SPSS (SPSS Inc, Chicago, Illinois, USA) statistical program was used for statistical analyses.
EDSS was categorised into four groups based on experimentally observed quartiles. T2-LV and T1-LV were logarithm transformed. Deseasonalised 25(OH)VD3, 1, 25(OH)2 VD3 and 24, 25(OH)2 VD3 were logarithm transformed.
Linear regression analyses were used to evaluate the associations of individual environmental factors and vitamin D metabolites. Deseasonalised 25(OH)VD3, 1, 25(OH)2 VD3 and 24, 25(OH)2 VD3 were individually evaluated as dependent variables. All of these regression analyses included age and sex as predictors and the following candidate environmental factors were added one by one as the third predictor: BMI, summer sun exposure, winter sun exposure, multivitamin supplement, vitamin D supplement, race (white or not), skin colour, eye colour, HLA DRB1*1501 and present interferon use.
As noted in the introduction above, disability can affect sun exposure, which in turn can affect vitamin D production in the skin. Therefore, we used a two stage analysis strategy to assess the role of sunlight and vitamin D on MRI outcomes in MS patients. In the first step, we assessed the associations of MRI outcomes with sunlight exposure after correcting for age, gender and EDSS quartiles. In the second stage, we included 25-hydroxy vitamin D3 levels as an additional predictor. Linear regression was used for analysis of the MRI measures of MS patients: T2-LV, T1-LV, normalised WBV and GMV. The MRI variable of interest was the dependent variable with age, sex, EDSS quartiles and the summer sun exposure quartiles as predictors. In follow-up analyses, 25 hydroxy-vitamin D3 levels were included as an additional predictor. A similar approach was used to assess MRI measures of controls except that EDSS quartiles were not included as a predictor.
A p value ≤0.05 was considered significant whereas a p value ≤0.15 was considered a trend.
Results
Demographic and clinical characteristics of the patient population are summarised in table 1.
Demographics and clinical characteristics of the patients
Environmental determinants of vitamin D metabolites
We first assessed the relative importance of candidate predictors of deseasonalised vitamin D metabolite levels in regression analyses that corrected for age and sex and the individual predictor of interest. Our candidate list of predictors included: BMI, skin colour, eye colour, multivitamin supplementation in the preceding 3 months, use of vitamin D supplements or calcium plus vitamin D supplements in the preceding 3 months, present use of interferon β, and summer and winter sun exposure in the preceding 2 years. Levels of 25 hydroxy vitamin D3, 1, 25 dihydroxy vitamin D3 and 24, 25 dihydroxy vitamin D3 metabolites were individually assessed as dependent variables. Table 2 shows the partial correlations and corresponding p values for the predictors. The results from the individual analyses indicated that multivitamin supplementation, BMI, summer sun exposure and eye colour had the strongest associations with vitamin D3 metabolite levels. The results from stepwise regression models were similar (data not shown).
Univariate analyses of different candidate vitamin D determinants
Figure 1A compares the relative contributions of multivitamin supplements to vitamin D or calcium plus vitamin D supplements in the preceding 3 months. The group that reported taking multivitamin supplements had an increase in deseasonalised 25 hydroxy vitamin D3 levels. Vitamin D or calcium plus vitamin D supplements did not increase deseasonalised 25 hydroxy vitamin D3 levels in the group also taking multivitamin supplements.

(A) Dependence of deseasonalised 25-hydroxy vitamin D3 levels (in ng/ml on the left axis and nmol/l on the right axis) on the presence or absence of multivitamin consumption in the preceding 3 months. The dark gray (blue in online version of figure) bars correspond to the group that did not take vitamin D or calcium plus vitamin D supplements and the light gray (green in online version of figure) bars correspond to the group that took vitamin D or calcium plus vitamin D supplements. (B) Dependence of deseasonalised 25-hydroxy vitamin D3 levels (in ng/ml on the left axis and nmol/l on the right axis) on the quartile of summer sun exposure in the preceding 2 years in the absence (dark gray bars/blue bars in online version of figure) or presence (lighter gray bars/green bars in online version of figure) of multivitamin consumption. The bars represent the mean values and error bars are SEs. Access the article online to view this figure in colour.
Figure 1B compares the relative contributions of multivitamin supplements for different quartiles of summer sun exposure. A pattern of increasing deseasonalised 25 hydroxy vitamin D3 levels with increasing quartile of summer sun exposure was found. The higher quartiles of summer sun exposure exhibited a more marked increasing trend in those not taking multivitamin supplements.
Relationships to MRI outcomes
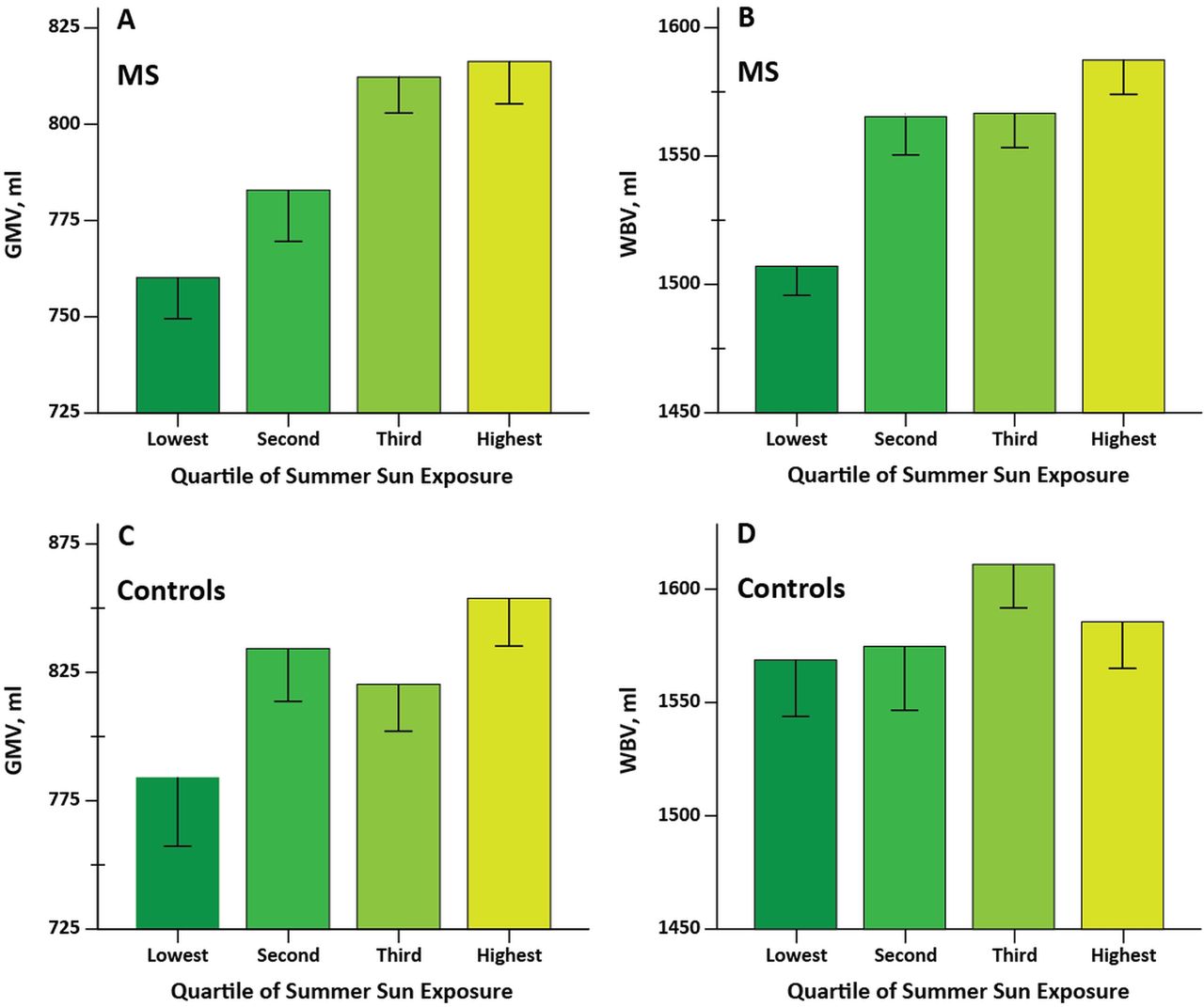
The results from the two stage statistical analyses are summarised in table 2. T2-LV and T1-LV were not associated with sun exposure. The dependence of GMV and WBV for different quartiles of summer sun exposure is shown in figure 2A and B, respectively. Increased summer sun exposure was associated with increased GMV and WBV after correcting for EDSS. Additional analyses with an interaction term between EDSS and summer sun exposure were conducted and did not support a significant interaction. In the second stage of the analysis, the inclusion of vitamin D did not substantially affect the positive associations between sun exposure and GMV and WBV. Interaction analysis between sunlight and 25-hydroxy vitamin D3 is not included given the non-significant main effects for vitamin D. We also separately assessed the associations of sunlight in the subsets of MS patients with relapsing disease and those with progressive disease (secondary progressive or primary progressive MS). The findings are summarised in the online supplementary data.
{kind=link}
{kind=link}
(A) Dependence of normalised grey matter volume (GMV) and (B) normalised whole brain volume (WBV) of multiple sclerosis (MS) patients on the quartile of summer sun exposure in the preceding 2 years. (C) Dependence of GMV and (D) WBV of healthy controls on the quartile of summer sun exposure in the preceding 2 years. The lower quartiles of sun exposure are in darker shades of gray (green in online version) and the highest quartile is lighter shades of gray (more yellow in online version). The bars represent the mean values and error bars are SEs. Access the article online to view this figure in colour.
We had sun exposure and MRI data on 69 controls (mean age 43.7±SD 11.7 years, 55% female). In regression analyses that corrected for sex and age, we found a trend between increased sun exposure and increased normalised GMV (rp=0.21, p=0.087, figure 2C). WBV was not associated (p=0.45, figure 2D).
Discussion
The purpose of this study was to systematically assess the relative contributions of different environmental factors to vitamin D metabolite levels in MS patients and to determine whether sunlight exposure was associated with MRI measures of brain injury. Our results indicate that BMI, multivitamin supplementation, summer sun exposure and eye colour had strong associations with vitamin D metabolite levels. Increased sun exposure was associated with increased WBV and GMV after adjusting for disability and 25-hydroxy vitamin D3 levels. Our results are consistent with the possibility that immunomodulation resulting directly from sun exposure may be a contributing factor to MRI outcomes in MS.
The main limitation of this study is that it is a cross sectional study, which limits the ability to obtain cause–effect assessments from associations. Our findings are consistent with an effect of sun exposure on WBV and GMV but they could potentially also be caused by lifestyle changes consequent to disability. Although we undertook several precautions to address the potential adverse effects of reverse causation by obtaining blood biomarker assessments and using MRI measures, only prospective longitudinal studies can fully eliminate the confounding effects of reverse causation. Both longitudinal MR measures and longitudinal measures of environmental factors are needed, with careful repeated measurements of both summer and winter sun exposure and 25-hydroxy vitamin D levels.
We found that multivitamin supplementation results in greater changes in 25-hydroxy vitamin D3 levels in individuals with lower levels of sunlight exposures. Our results are consistent with the possibility that the active metabolite levels are regulated. Steffensen et al19 also found similar results for supplementation in a randomised clinical trial of vitamin D effects on bone mineral density that involved 60 MS patients. Recent data suggest that interferon beta treatment is more effective against relapses if vitamin D levels are sufficient.14 We also assessed but did not find evidence that present treatment with interferon β increased levels of either 25 hydroxy vitamin D3 or 1, 25 dihydroxy vitamin D3. However, a prospective vitamin D add-on study would be appropriate for directly addressing this issue. Analogously, we also assessed whether the presence or absence of disease modifying treatments (including glatiramer acetate or natalizumab) were associated with vitamin D metabolites but did not find evidence for significant associations (data not shown). One potential criticism of our methodology is that we did not collect information on the precise multivitamin brands used by our subjects, which might have enabled more systematic dose estimation for vitamin D and a better understanding of the role of other vitamins and minerals. Many currently available multivitamin supplements are taken once daily and contain vitamins and minerals at levels close to the required daily allowance.20
Our study complements longitudinal studies that have investigated the seasonal dependence of relapses,21–23 contrast enhancing lesions (CEL)24 and new T2 lesions.25 However, there are studies that did not find evidence to support seasonal dependence of CEL26 or of relapses.27 A study of 28 patients by Killestein et al28 did not find seasonality in the number of active lesions but reported seasonal variation in interferon γ secretion, which was weakly associated with MRI variations. Seasonality in interferon γ secretion was also found in a Tasmanian study of untreated MS and in a study of progressive MS.29 ,30 In our study, we obtained long term self-reported sun exposure measures rather than month of measurement to assess the impact on MRI measures of lesion burden and neurodegeneration. We did not assess CEL because these are transient compared with the period over which the sun exposure measures were obtained. We conducted the analyses (data not shown) but did not find evidence for seasonality for CEL. However, longitudinal serial MRI scanning is necessary to effectively answer this question. Also, the majority of our patients were on disease modifying therapies, which are known to suppress CEL activity.
A critical challenge in assessing environmental factors such as sun exposure is that these measurements are difficult to make and are subject to recall errors. Latitude and meteorological exposure data have frequently been used as objective surrogate measures of incident sunlight exposure in epidemiological studies but these cannot be used for studies such as ours that span a geographically small area. The biological exposure at a given level of sun exposure can further be modulated by skin pigmentation, level of outdoor activity, clothing and sunscreen use. Because our sample contained patients of Caucasian and non-Caucasian racial ancestry who differ in skin pigmentation, we conducted subanalyses of the results shown in tables 2 and 3 for the subset of patients of Caucasian race. The conclusions were not substantively changed (data not shown). Clothing and sunscreen use are more difficult to meaningfully measure although surveys to collect these data have been developed. Silicone skin casts have been used to image skin damage induced by UVR and can serve as a surrogate marker for long term sun exposure to skin.31 We did not obtain silicone skin casts. However, to address these concerns, we included multiple vitamin D metabolites as biomarkers, which are dependent in part on sun exposure, but can be objectively measured. We also focused on obtaining information on sun exposure in the preceding 2 years given the potential recall problems associated with obtaining past sun exposure of longer duration. Systematic studies of sun exposure have shown good test–retest reproducibility in MS.31 Sun exposure and vitamin D were reported to be independent risk factors for CNS demyelination in an Australian multicentre case control study of MS incidence. Greater UV induced skin damage and higher vitamin D levels were associated with a decreased risk of the initial demyelinating event.32
Dependence of MRI measures on sun exposure
The doses of oral vitamin D necessary for achieving therapeutic outcomes in clinical trials and MS prevention remains unclear, given the lack of large randomised placebo controlled studies. In a small 48 week study of 15 patients, 1, 25 (OH)2 vitamin D (calcitriol 2.5 μg/day) treatment reduced the relapse rate compared with the period preceding study entry; treatment discontinuation was associated with an increase in EDSS.33 Two patients experienced hypercalcaemia. An open label randomised 52 week trial of high dose vitamin D escalation (up to 40 000 IU/day) followed by de-escalation, found a trend towards lower relapse rates compared with the control group, which received 4000 IU/day vitamin D supplementation (4000 IU/day). A 6 month, placebo controlled, double blind clinical trial of vitamin D2 in MS patients failed to find improvements on MRI and clinical outcomes despite increasing vitamin D levels in serum.34 A randomised trial of the vitamin D3–interferon β-1b combination therapy (20 000 IU or 500 µg of vitamin D3, once weekly) did not meet its primary MRI endpoint of T2 disease burden; however, CEL burden was significantly reduced.35 Additional preplanned analysis of this study showed a smaller T2-LV growth and less new/enlarging T2 brain MRI lesions in the vitamin D3 treated compared with the placebo treated subgroup.35 ,36 A 96 week trial of vitamin D3 supplementation did not find evidence for a vitamin D effect.37 The Institute of Medicine report,38 which was based on a systematic review of an extensive body of clinical literature, found that there was evidence to support calcium and vitamin D use in bone health but did not find evidence to support its use in other conditions, such as MS.39 The therapeutic potential of vitamin D in MS should therefore be viewed with equipoise until the outcomes of larger randomised clinical trials are available.40
In conclusion, the results from our cross sectional study suggest that sun exposure could have an effect on brain volume in MS. These effects appear to be dissociated from the increased vitamin D levels that result from increased sun exposure. However, it is necessary to overcome the limitations of the cross sectional study design before definitive conclusions can be established. Further prospective longitudinal studies of the effects of sun exposure on brain volume reserve in controls and on neurodegeneration in MS patients are therefore needed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors RZ: study design, MRI data acquisition, data interpretation and manuscript preparation. CNT: data analysis. BW-G: study design, oversaw all clinical aspects of the project including clinical data acquisition, data analysis and interpretation, and manuscript preparation. CT: data analysis. NB: MRI data acquisition. KOC: data analysis. MGD: MRI method development and analysis. EC: MRI data acquisition. DPR: data acquisition. JQ: vitamin D analysis and acquisition. MR: study design, data analysis and interpretation, and manuscript preparation.
-
Funding We gratefully acknowledge support from the National Multiple Sclerosis Society (RG3743 and RG 4836-A-5) and the Department of Defence Multiple Sclerosis Program (MS090122). The funding sources had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; or in the preparation, review or approval of the manuscript.
-
Competing interests RZ has received speaker honoraria and consultant fees from Teva Neurosciences, Biogen Idec, Questcor, Genzyme-Sanofi, Novartis, Bracco, Bayer and EMD Serono. He has received research support from the National Multiple Sclerosis Society, Department of Defence, Biogen Idec, Teva Neuroscience, Teva Pharmaceuticals, EMD Serono, Genzyme-Sanofi, Questcor, Bracco and Greatbatch. BW-G received honoraria for serving in advisory boards and educational programmes from Teva Neuroscience, Biogen Idec, Novartis, Accorda EMD Serono, Pfizer, Novartis, Genzyme and Sanofi. She also received support for research activities from the National Institutes of Health, National Multiple Sclerosis Society, National Science Foundation, Department of Defence, EMD Serono, Biogen Idec, Teva Neuroscience, Cyberonics, Novartis, Acorda and the Jog for the Jake Foundation. JQ received research funding from the Department of Defence, the National Science Foundation, the National Institutes of Health, the American Heart Association, Kinex, CH3, Pfizer, Novartis, Abbott and Amgen. These are unrelated to the research presented in this report. MR received research funding or consulting fees from EMD Serono, Biogen Idec, Allergan, Netezza, Pfizer, Novartis, Monsanto, the National Multiple Sclerosis Society, the Department of Defence, Jog for the Jake Foundation, the National Institutes of Health and National Science Foundation. He received compensation for serving as an editor from the American Association of Pharmaceutical Scientists. These are unrelated to the research presented in this report.
-
Ethics approval The study was approved by the Human Subjects Institutional Review Board of the University at Buffalo.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary