Article Text

Abstract
Objectives To evaluate the very long-term clinical outcome of surgery for mesial temporal lobe epilepsy and unilateral hippocampal sclerosis (MTLE/HS) without atypical features. The impact of surgical technique and postoperative reduction of medication on this outcome was investigated.
Design Prospective longitudinal cohort follow-up study for up to18 years.
Setting Epilepsy surgery centre in a university hospital.
Patients 108 patients who underwent unilateral MTLE/HS.
Intervention Surgery for MTLE/HS.
Main outcome measure Engel classification (I). Clinical evaluations were based on systematic interviews in person or by phone. Kaplan-Maier survival curves estimated the probability of remaining seizure free. The impact of medication management in the postoperative outcome was analysed using Cox regression.
Results The probability of remaining completely seizure-free at 12 and 18 years after MTLE/HS surgery was 65% and 62%, respectively. The risk of having any recurrence was 22% during the first 24 months and increased 1.4% per year afterwards. Type of surgical technique (selective amygdalohippocampectomy vs anterior temporal lobectomy) did not impact on outcome. Remaining on antiepileptic drugs and history of generalised clonic seizure diminished the probability of remaining seizure free.
Conclusions MTLE/HS surgery is able to keep patients seizure free for almost up to two decades. Removal of the neocortex besides the mesial portion of the temporal lobe does not lead to better chances of seizure control. These findings are applicable to the typical unilateral MTLE/HS syndrome and cannot be generalised for all types of TLE. Future longitudinal randomised controlled studies are needed to replicate these findings.
- Anticonvulsants
- Epilepsy
- Epilepsy, Surgery
- EEG
Statistics from Altmetric.com
Introduction
Patients and physicians share the hope that surgical treatment for unilateral mesial temporal lobe epilepsy associated with hippocampal sclerosis (MTLE/HS) will lead to seizure cure.1 Although such goal has been achieved by many,2 differences in postoperative outcome exist3–5 and relapse may occur after many years of being seizure free. The very long-term outcome of such surgery—that is, whether epileptic patients that underwent MTLE/HS surgery remain seizure free for more than a decade—is not well known.
Using a longitudinal design, we performed detailed analyses in a large cohort of patients with MTLE/HS followed for up to 18 years and addressed two major clinical issues: (1) the timing and probability of seizure controls/relapses at long-term follow-up, that is, 8–18 years after surgery and (2) whether long-term antiepileptic drug (AED) management throughout the postoperative period would affect probability of relapse of seizures. Furthermore, we analysed the impact of medication management in the postoperative outcome. If resection of neocortex besides the mesial portion of the temporal lobe were relevant to seizure control, it could be expected from a theoretical point of view that patients undergoing larger resections would do better on the very long term.
Methods
Patients
Longitudinal follow-up data on postoperative seizure control were collected in 108 patients operated for medically refractory MTLE/HS at the Porto Alegre Epilepsy Surgery Center between January 1992 and March 2010.
Patients were followed for a minimum of 8 years to a maximum of 18 years (mean: 11 years and 9 months). They comprise 67% of the original sample of 161 patients followed up to 2003.6 The remaining 53 patients could not be recontacted to assess current status, in spite of multiple efforts. There were no clinical or demographic differences between the present cohort and the subcohort not contacted at the last follow-up, except that the latter had significantly more patients with exclusively unilateral temporal and less often stopped medication. Demographic and clinical characteristics of the current study sample (N=108) are shown in table 1.
Clinical characteristics of the study sample*
All patients had (1) a clinical history and video confirmation of a semiological pattern typical for MTLE, (2) interictal scalp-sphenoidal EEG with unilateral or independent bilateral anterior temporal epileptic discharges, (3) at least one electroclinical seizure recorded during video-EEG monitoring and (4) unilateral HS as indicated by MRI. Patients with atypical auras, early clonic or dystonic manifestations, interictal discharges in the posterior temporal or extratemporal regions and a second lesion on MRI were excluded. See refs. 6 and 7 for more details of patient selection, EEG, MRI and histopathological analyses. For the anterior temporal lobectomy (ATL), the anterior 3–4 cm of the anterior temporal neocortex were resected. Mesial structures were then removed, beginning with aspiration of the amygdala, followed by en bloc resection of the anterior 2–3 cm of the hippocampus and of the parahippocampal gyrus, extending posteriorly to the midmesencephalic level. For the selective amygdalohippocampectomy (SAH), mesial structures were removed according to the technique originally described by Niemeyer.8 Access to the ventricle was obtained through a 1.5–2.5 cm incision in the second temporal gyrus, and excision of the amygdala, hippocampus and parahippocampal gyrus proceeded in the same fashion as performed for ATL. The choice of surgical approach paralleled the advancements in the understanding of the epileptogenic bases of MTLE/HS. At the beginning of our study, all patients had an ATL. This was followed by a period when both techniques were performed without any specific attempts at randomisation. Specifically, the decision to perform ATL or SAH was taken during the operation, based on the anatomic presentation of the superficial temporal veins and the orientation of the second temporal gyrus. Because we realised that surgical results with the selective approach were similar to those obtained with ATL, we always favoured the neocortex-sparing technique.
All surgeries were performed by the same neurosurgeon (EP).
Procedure
Follow-up assessments
During the first year after surgery, follow-up data were obtained through clinical interviews in person via visits to the outpatient clinic or by telephone interviews every 6 months. The interviews were repeated yearly until the fifth postoperative year and at 1–3-year intervals thereafter. At the end of the follow-up period (2010), seizure risk was evaluated by a neurologist (MH) or by the neurosurgeon (EP) by means of a phone interview. At all follow-up assessments, interviews were conducted according to structured interview methods. In most cases the patient and relative were interviewed.
The study was approved by the Ethics Committee of our Institution, following the regulations of the Declaration of Helsinki. It also complies with federal laws governing research studies with humans in Brazil. All patients gave written informed consent to the use of clinical data in research studies.
Treatment regimen and diagnostic classification
Patients were maintained on therapeutic dosages of their habitual AEDs for at least 2 years after surgery. Afterwards, they could (1) remain with the same medication regimen or minimally reduce medication, (2) have a major reduction (switch to monotherapy or bitherapy using less than 50% of preoperative dosages) or (3) completely stop medication. All patients who were seizure-free 2 years after surgery were given the option of progressively reducing medications until discontinuation. Those who continued taking full doses of medication or did not reduce after a certain point, specifically chose to do so. AED management was evaluated on case by case basis and based on clinical judgement.
Outcome in relation to seizure control was based on Engel's classification.9 Briefly, class I describes patients who are free of disabling seizures even if they have or had some auras or intervening episodes strictly related to medication change. The subclass IA specifically describes patients who are completely seizure free, and thus had our primary interest in this study. Class II are those patients who have rare disabling seizures (1–3 per year) or whose seizures occur only during sleep; and classes III and IV describe patients with less favourable outcomes. Recurrence was defined as any seizure 1 month after surgery.
Statistical analyses
Survival analyses were conducted and Kaplan-Meier curves generated to investigate the probability of staying in Engel's outcome classes IA or I (A, B, C, D). Mean survival in each outcome class and 95% CIs were calculated. Furthermore, the statistical outcome relevance of type of surgical technique was tested through univariate and multiple Cox regression analyses. Significance level was set at p<0.05.
Results
Survival analyses: timing and probability of relapses
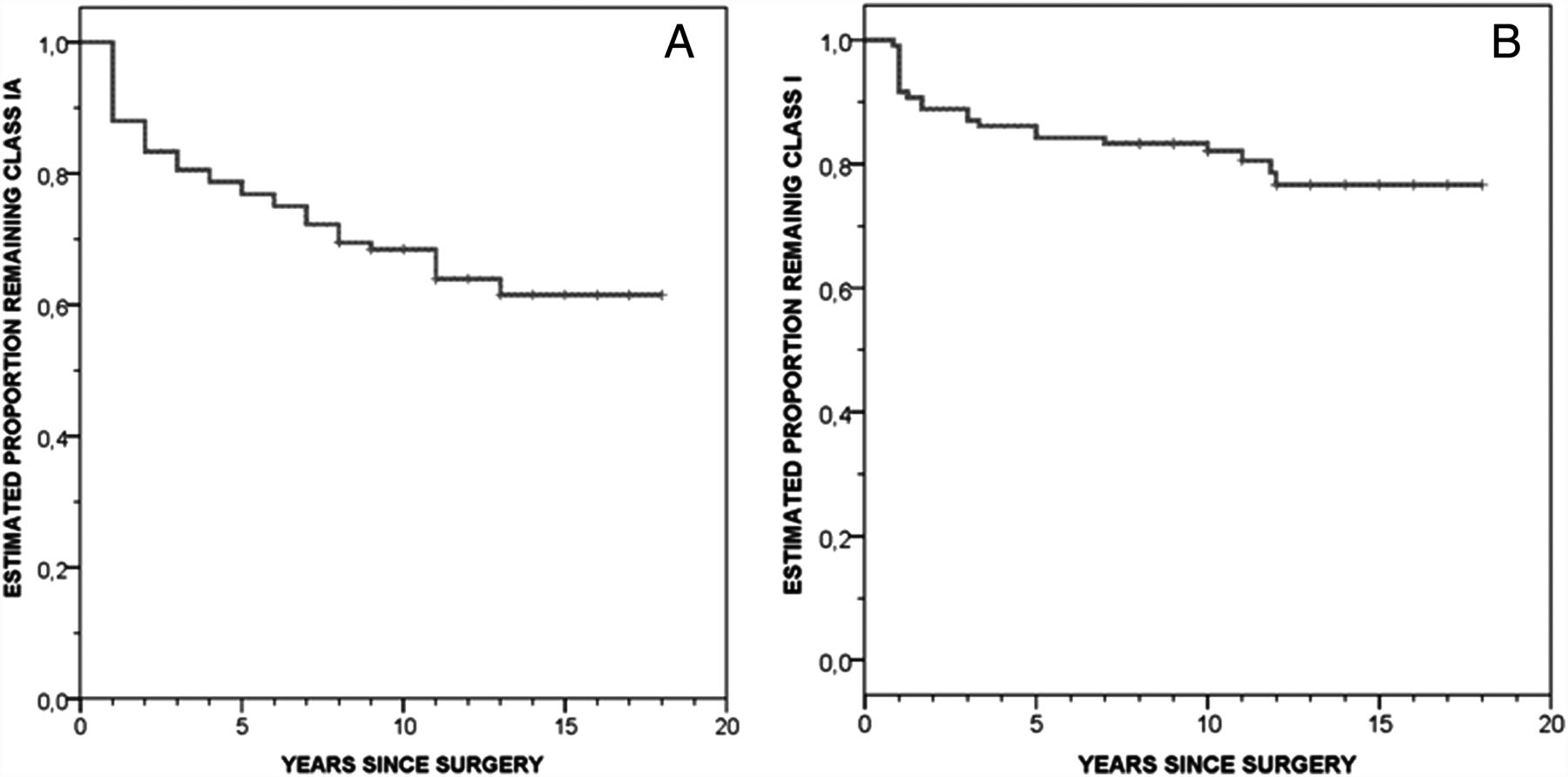
The probability of remaining at class IA at 12 years and 18 years was 65% and 62%, respectively (mean 13 years; 95% CI 11.6 to 14.3). At class I, the corresponding probabilities were 77% and 77%, respectively (mean: 15 years; 95% CI 13.7 to 16) (figure 1). Figure 1 shows that the probability of remaining completely seizure free decreased sharply to 78% in the first 2 years after surgery, and then slowly during the next 16 years, from 78% to 56%. Thus, the risk of having any recurrence, from auras to single to multiple seizures was 22% during the first 24 months and increased 1.4% per year afterwards. Similarly, the probability of remaining in outcome class I decreased to 91% in the first 9 months and then from 91% to 78% in the ensuing 17 years. Hence, the risk of having recurrent seizures not compatible with outcome class I was 12% per year in the first 9 months and increased 0.7% per year afterwards.

Kaplan-Meier cumulative survival curve. Note that recurrences peak early and progress slowly over the years. (A) Engel's outcome class IA (N=108). (B) Engel's outcome class I (N=108).
Sixty-six patients (61%) have always been completely seizure-free and 42 (39%) had any type or severity of seizure recurrence. Nineteen (45% of those who relapsed and 17% of all patients) had recurrence of auras or breakthrough seizures acutely associated with reduction of AED, thus remaining in outcome class I. The other 23 patients progressed to less favourable outcomes. Engel's outcome classification at last visit in 2010 and actual timing of recurrence for each patient is given in tables 1 and 2.
Time of first seizure recurrence and outcome class at last contact*
Seizure control, medication status and other clinical variables
Throughout the follow-up period, 4 of the 85 patients (5%) in class I decided to maintain the preoperative doses of AED, whereas 32 (48%) reduced medication doses to a certain point, but elected not to proceed to discontinuation. Respective figures were 0/66 and 22 /66 (33%), respectively, for those in class IA at the last follow-up. Patients who discontinued medication (55%) more often had a class IA outcome throughout the entire follow-up period than patients who maintained (24%) or reduced (21%) their medication (p=0.03; figure 2). A comparable association was observed for patients who relapsed but remained in class I, though the association was now a statistical trend (p=0.10). The association between medication status and seizure classification was confirmed by Cox regression analyses. Specifically, analyses showed that the need to maintain full or almost full doses of AEDs led to a reduced chance of remaining in class I (Cox regression univariate, p=0.017, CI 1.26 to 10.85; multivariate, p=0.024, CI 1.00 to 9.66; table 3).
Univariate and multivariate analysis of variables associated with seizure recurrence

Kaplan-Meier cumulative survival curve. (A) Engel's outcome class IA in relation to antiepileptic drug (AED) management. (B) Engel's outcome class I in relation to AED management.
Given that the direction of effect of the analyses investigating the association between medication status and class IA classification were somewhat unexpected, secondary Cox regression analyses were performed to examine whether clinical characteristics other than medication status may have accounted for some of these findings. These analyses indicated that any degree of lateralisation of interictal spikes below 100% (ie, with any degree of bitemporality of spikes) significantly diminished the chances of remaining in class IA (Cox regression: p=0.04 CI 0.22 to 4.02). Moreover, a history of generalised tonic-clonic seizure (GTCS) significantly tended to reduce the chances of remaining in class I (Cox regression: p=0.07 CI 1.33 to 9.80). Multivariate analyses retained only a history of GTCS and AED status as significantly reducing the probability of remaining in outcome class I (Cox regression: p=0.003 CI 1.84 to 22.41).
Outcome in relation to surgical technique
Of the 66 patients in Class IA, 35 (53%) had a SAH and 31 (46%) an ATL, while rates of each technique for those 85 patients who were in class I were 50% and 50%. Likewise, there were no significant differences in those with less favourable outcomes (class II, III, IV; figure 3). Furthermore, of the 19 patients who relapsed over the years but remained in class I, 11 (58%) had an ATL and 8 (42%) a selective approach. Finally, of the 23 patients in outcome classes II, III and IV who relapsed early, 14 (60%) had an ATL and 9 (40%) a SAH. Overall, of 42 patients who had any recurrence, 25 (60%) had had an ATL and 17 (40%) a SAH. This distribution was maintained irrespective of the AED status at the time of recurrences, that is, whether patients recurred on full doses of medication, upon acute reduction or after a latent period of significant reduction or discontinuation (data not shown). Hence, overall, both surgical techniques were equally effective in terms of seizure outcome.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier cumulative survival curve. (A) Engel's outcome class IA in relation to surgical technique. (B) Engel's outcome class I in relation to surgical technique.
Discussion
Excellent short-term and medium-term results of epilepsy surgery for TLE/HS have been reported.10–12 A number of long-term outcome studies in TLE however have found that patients may relapse after many years of being seizure free.11 ,13 ,14 McIntosh and colleagues showed that the probability of complete seizure freedom at 2 years and 10 years after surgery was 55% and 41%, respectively, and patients with two seizure-free postoperative years had a 74% probability of seizure freedom by 10 postoperative years.14 In another series, 53% of 371 patients undergoing ATL were seizure free at 10 years15 and in a recent study, the seizure free rate at 5 years was 55% specifically for patients with TLE/HS.3 A very recently published study reports the longitudinal outcome (mean: 26 years) of patients with a variety of seizure types who underwent surgery in the 1960s, 1970s and 1980s using a broad range of epileptic surgical techniques, and showed that about 48% were Engel class I.16 However, neither these nor other studies17–19 had followed a significant number of patients with exclusive TLE/HS for more than 10 years and studied the probability to remain completely seizure-free (class IA). Since most patients are operated in young adulthood, it is important to study clinical outcome beyond the first decade, because this is pivotal to the level of social and professional independence these patients may achieve for most of their lives.
In the present study, patients were followed for 8–18 years after MTLE/HS surgery. We found that 62% were completely seizure free throughout the entire follow-up period, whereas 77% maintained a class I outcome. Our study focused on patients undergoing MTLE/HS surgery and investigated the probability of being completely seizure free (ie, class IA), and showed that that MTLE/HS surgery prevents subsequent seizures for up to close to two decades.
Consistent with previous studies, we found that recurrences occur along two different temporal axes, probably mirroring two distinct underlying ictal mechanisms.15 ,20 ,21 One axis is more acute. Specifically, the slope of the curve is changing direction after 2 years for all types of relapses and after 9 months for severe recurrences, in which patients do not meet the criteria any more for outcome class I. This pattern comprises between half and two-thirds of all relapses and is most likely related to incomplete localisation or resection of the epileptogenic zone. The second axis represents a much more gradual relapse curve, associated with an annual probability of 0.6% to 1.3% for severe or any type of recurrence, respectively. The mechanism(s) of these late recurrences may be related to progressive plastic changes, which in turn leads to reorganisation of vulnerable networks and a slow progression of epileptogenesis.
Notably, we found that patients in whom significant or complete reduction of AED was achieved over the years had greater chances of remaining seizure free. By contrast, patients who had intervening seizures more often continue to use significant doses of AEDs in the follow-up period. Although this finding strictly reflects a naturalistic observation and is certainly biased by the fact that patients who fared less well tended to continue with AEDs, it is nonetheless consistent with our previous observations as well as from others13 ,22 showing that judicious AED discontinuation may not increase the risk of seizure recurrence; instead, underlying epileptogenic features may be much more relevant for the probability of achieving and maintaining seizure freedom. Despite mentioning that patients with seizure recurrence tended to stay on antiepileptic drugs, whereas those who were seizure free did not, we are not implying a causal relationship, that is, continuing to take AEDs did not cause the seizure recurrence and stopping AEDS did not lead to seizure freedom. Specifically, previous studies have shown that clinical characteristics, such as restricted unilateral MTLE/HS, no history of GTCS and no atypical features, are all predictors of seizure remission.14–16 ,19 ,23 ,24 Indeed, our subsequent Cox regression analyses also showed that patients with intervening seizures tended to have presurgery GTCS and bitemporal independent epileptiform discharges. Randomised controlled studies in large samples are needed to further identify clinical predictors of long term surgery efficacy in seizure control.
Notably, we showed that ATL and transcortical SAH were equally effective in terms of long-term outcome. These findings are of particular interest since it could be argued that, even if ATL and transcortical SAH do not differ in degree of seizure control for the first few years after operation,6 ,7 ,25 should the temporal lobe tissue left behind in the selective approach have unequivocal potential to build up epileptogenic activity, survival curves of seizure-free outcomes of the two procedures would diverge after 10 or more years, in favour of the more extensive resection. This was however not the case, even after history of GTCS, bilaterality of EEG discharges or need for intracranial electrodes was controlled for.
The lack of difference in seizure outcome between the techniques is of clinical interest, given previous findings that patients with strictly unilateral MTLE/HS undergoing a selective approach had better chances to improve cognitively after operation.6 Hence, the similar long-term outcome associated with either technique suggests that selective procedures should be preferred in these patients. Similar findings have been recently reported in a comprehensive review,26 although most studies do not report a direct comparison between these two specific techniques, performed by the same surgeon, in a virtually sequential fashion and in a very homogeneous syndrome in all patients. Moreover, these findings suggest that the apparently common association between HS and neocortical temporal microscopic focal cortical dysplasia (FCD)27 probably adds little in terms of epileptogenesis, raising doubts on the ethiopathology and clinical relevance of this abnormality—which, in fact, form the basis for a new classification of FCD.28 ,29 Dysplastic abnormalities in the resected tissue not seen on MRI (ie, invisible dual pathology), have been reported to accompany HS in a variable number of patients in consecutive series of TLE surgery.27 ,30 ,31 If these finds are generalisable for TLE/HS, it would be reasonable to assume that at least in some of our patients operated by the selective technique this invisible dysplastic cortex would have been left behind. As a corollary, should these putative abnormalities be epileptogenically relevant, patients operated through the selective technique would have been unlikely to achieve the same good results as those operated through the more extensive temporal lobectomy technique—which would have resected this dysplastic portion also.
Interestingly, Schijns and colleagues reported seizure outcome following selective or non-selective surgery in patients with MTLE/HS, with and without associated neocortical temporal lobe MRI abnormalities suggestive of FCD—and similarly found that seizure control did not differ with either technique.32 Future studies are needed to further systematically investigate the link between specific clinical characteristics and longitudinal outcome, as a function of surgical technique.
The current study has some limitations, one of them the non-randomised design for the selected surgical technique. Another is the fact that our findings cannot be generalised for all types of TLE epilepsy and even MTLE/HS because we excluded patients with less typical clinical and EEG features, such as atypical auras, early clonic motor manifestations and extension of discharges to posterior temporal electrodes. Admittedly, these latter patients are increasingly seen in tertiary epilepsy centres, but a sizeable proportion of MTLE/HS patients do present the typical picture included in our analysis. Patients with unilateral HS but less typical presentations often demand more extensive evaluation strategies to assess the involvement of neocortical temporal, frontal or perisylvian areas, and even when an anterior mesial temporal epileptogenic zone is confirmed, a non-selective temporal resection technique is probably indicated. Furthermore, since records from early childhood care of a number of patients were not available, data regarding the presence of febrile seizures as initial precipitating injuries were not reliable enough to be included in the analyses. However, because patients were selected on the basis of the electroclinical syndrome of MTLE/HS, it is unlikely that the proportion of patients with febrile seizures would differ from other patient samples.33 Another limitation is that because memory outcome is currently being analysed, we have not included present data on memory performance at this extended follow-up. Interesting findings related to late cognitive plasticity may emerge, particularly from comparisons with the interim results reported some years ago in these same patients.6 Finally, although data had been collected over the years at the clinic, seizure outcome at the very last follow-up was based on a structured phone interview. However, all interviews were done by a neurologist, in a standardised manner and often included more than one informant.
In conclusion, notwithstanding some limitations, the present study demonstrated that surgery for typical unilateral MTLE/HS can provide remarkable seizure alleviation until at least one to two decades after surgery. Our study also showed that removal of the neocortex besides the mesial portion of the temporal lobe does not lead to a better long-term outcome, an observation which is of strong clinical interest. The next major challenge in the field of temporal lobe epilepsy surgery would be to identify specific patient profiles with greater risk for recurrence and adjust treatment strategies accordingly.23 ,34
Acknowledgments
We thank our colleagues of the Severe Epilepsies Outpatient Clinics, including all neurology and neurosurgery residents from these last two decades for helping to take care of the patients included here. We particularly thank Dr Carolina Torres and Dr Jose Victor Martinez for helping out with preceptorship in the Clinic. Finally, we were blessed by the opportunity to develop honest doctor-patient and doctor-family relationships, which provided an exquisite degree of cooperation when collecting outcome data over the years. We cannot thank these people enough for their goodwill. We also thank Dr Renata Kieling for extremely useful suggestions. Linda Booij, PhD is supported by a career award from the Fonds de recherchedu Québec-Santé. None of these funding agencies played a role in the design, data collection, management, analysis, interpretation of the data; and preparation, review or approval of the manuscript.
References
Footnotes
-
Contributors MH, AP and EP designed the study, collected the data and wrote the manuscript. EP operated all patients. EBP, JCdC, LB, MP, NA and MLN critically reviewed the manuscript and directly influenced the final format of the submission. VV helped with data collection and with MH organised the data bank.
-
Funding The study was supported by a grant from CAPES: 00000.058723/2010.
-
Competing interests AP, MD, PhD: holds a grant from CNPQ; receives funds from Novartis, Abbott, Janssenn-Cilag and Eli-Lilly as board member; invited speaker for the development of educational presentations, for manuscript preparation and to cover meeting/travel expenses unrelated to the present study. MH, MD, PhD: has a grant pending from CAPES, PNPD programme. The other authors report no other competing interests.
-
Ethics approval Pontificia Universidade Catolica do Rio Grande do Sul Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.