Article Text

Abstract
Objective The purpose of this study was to assess the risk factors of prospective symptomatic haemorrhage in a large series of adult patients with cerebral cavernous malformation (CM).
Methods Three hundred twenty-six patients >18 years of age with 410 CMs were evaluated retrospectively. Symptomatic haemorrhage was defined as new clinical symptoms with radiographic features of haemorrhage. Clinical data and the characteristics of CM were analysed. MR appearance was divided into three groups according to Zabramski's classification.
Results The overall haemorrhage rate of CM was 4.46% per lesion-year. The overall annual haemorrhage rate according to MR appearance was as follows: type I, 9.47%; type II, 4.74%; and type III, 1.43%. A multivariate analysis revealed that prior symptomatic haemorrhage (p<0.001) and MR appearance (p<0.001) were statistically significant. After multiple comparisons, type I (p<0.001) and type II (p=0.016) showed higher haemorrhage risk than type III. However, no significant difference in haemorrhage rate was observed between type I and type II (p=0.105). Other variables including female gender, age, location, multiplicity, hypertension, size and associated venous angioma were not significant. The haemorrhage rates based on risk factors were estimated at 3 years as follows: 33.77% in patients with prior haemorrhage versus 7.54% in patients without prior haemorrhage (p<0.001); type I, 27.62% vs type II, 15.44% vs type III, 5.38% (p<0.001).
Conclusions Prior symptomatic haemorrhage and MR appearance could be related to prospective symptomatic CM haemorrhage in adults. A prospective multicentre observational study is necessary to confirm our results.
- Neurosurgery
Statistics from Altmetric.com
Introduction
The haemorrhage rate of cavernous malformation (CM) has been reported as 1.6–3.1% per patient-year in some prospective studies.1 ,2 However, no consistent conclusion has been made for risk factors of prospective CM haemorrhage except for prior history of haemorrhage. Such a discrepancy could originate from the relatively limited number of enrolled patients, the characteristics of CM that include haemorrhagic events with low prevalence,3 self-limited symptoms and de novo formation of CM,4 differences in the definition of haemorrhage, the calculation methods (person-years vs lesion-years), and the study method (retrospective vs prospective). In addition, surgical intervention can be primary or secondary treatment, making an accurate estimation for prospective CM haemorrhage difficult.
Recently, two large studies revealed the natural history and related factors of CM haemorrhage.5 ,6 Gross et al5 reported that prior haemorrhage increased the risk of subsequent CM haemorrhage based on their meta-analysis. However, those studies were limited because of the differences in the definition of haemorrhage and the various calculation methods used in each study. Flemming et al6 suggested that previous haemorrhage, multiple CM, and male gender were significant risk factors for future haemorrhage. However, because the patients who underwent radiosurgery were not censored in their analysis, the results might not be accurate enough to interpret the natural history of CM with conservative treatment. In addition, both studies included patients regardless of their age at the time of diagnosis. Previous reports have described differences in clinical features and origins of CM between adult and paediatric patient groups4 ,7 ,8; therefore, these groups cannot be assessed together. Accordingly, the results of the previous studies might not reflect the assessment of the haemorrhage risk in an adult CM population.5 ,6
The impact of CM haemorrhage development on clinical outcome is not life threatening in most cases. Although the history of haemorrhage is not a statistically significant risk factor for unfavourable postoperative outcomes in patients with brain and spinal CMs,9 haemorrhage development can lead to acute exacerbation of clinical symptoms and neurological deficit, which requires early aggressive surgical treatment. Accordingly, assessing haemorrhage risk prior to intervention can be useful in treatment planning.
The purpose of this study was to assess the risk factors of prospective symptomatic haemorrhage in a large series of adult patients with cerebral CM.
Patients and methods
This retrospective study was approved by the institutional review board of Seoul National University Hospital (H-1305-627-491). Patients with cerebral CM presenting at our institution from 1998 to 2010 were considered for inclusion in the study. Those who were ≤18 years of age, had undergone surgical resection or gamma knife surgery as an initial therapy, had a CM associated with other diseases such as an aneurysm, tumour or arteriovenous malformation, or had spinal CM, were excluded from the study. Overall, 326 patients with 410 cerebral CMs were followed. CMs with the following criteria were treated conservatively: (1) asymptomatic lesions, (2) critical brain areas such as the brainstem and functional cortices with minimal neurological deficit, (3) medically controlled seizures and (4) undetermined symptomatic lesions in multiple CMs.10 When the patient experienced progressive neurological deficits or repeated CM haemorrhage during the follow-up, a surgical intervention was carried out. During the follow-up period the patients who had surgical intervention were censored at the time of the treatment. A telephone survey was conducted for patients without a recent follow-up.
Their medical records were reviewed which included sex, age, hypertension, diabetes mellitus, pregnancy, smoking and the occurrence of symptomatic haemorrhage. Their initial presenting symptoms were categorised into two groups: haemorrhage-related and haemorrhage-unrelated. Patients were included in the haemorrhage-related group when radiological haemorrhagic evidence with consistent clinical signs was observed on the MRIs. Symptoms (seizures, focal neurological deficits, headaches, vertigo or diplopia) without evidence of CM haemorrhage on the MRIs or incidental lesions were considered as haemorrhage-unrelated. The end point of the study was the occurrence of prospective symptomatic CM haemorrhage during the follow-up period. Prospective symptomatic CM haemorrhage was defined as new clinical symptoms with radiographic evidence of haemorrhage including intralesional11 or extralesional signal change or a size increase >20%.1
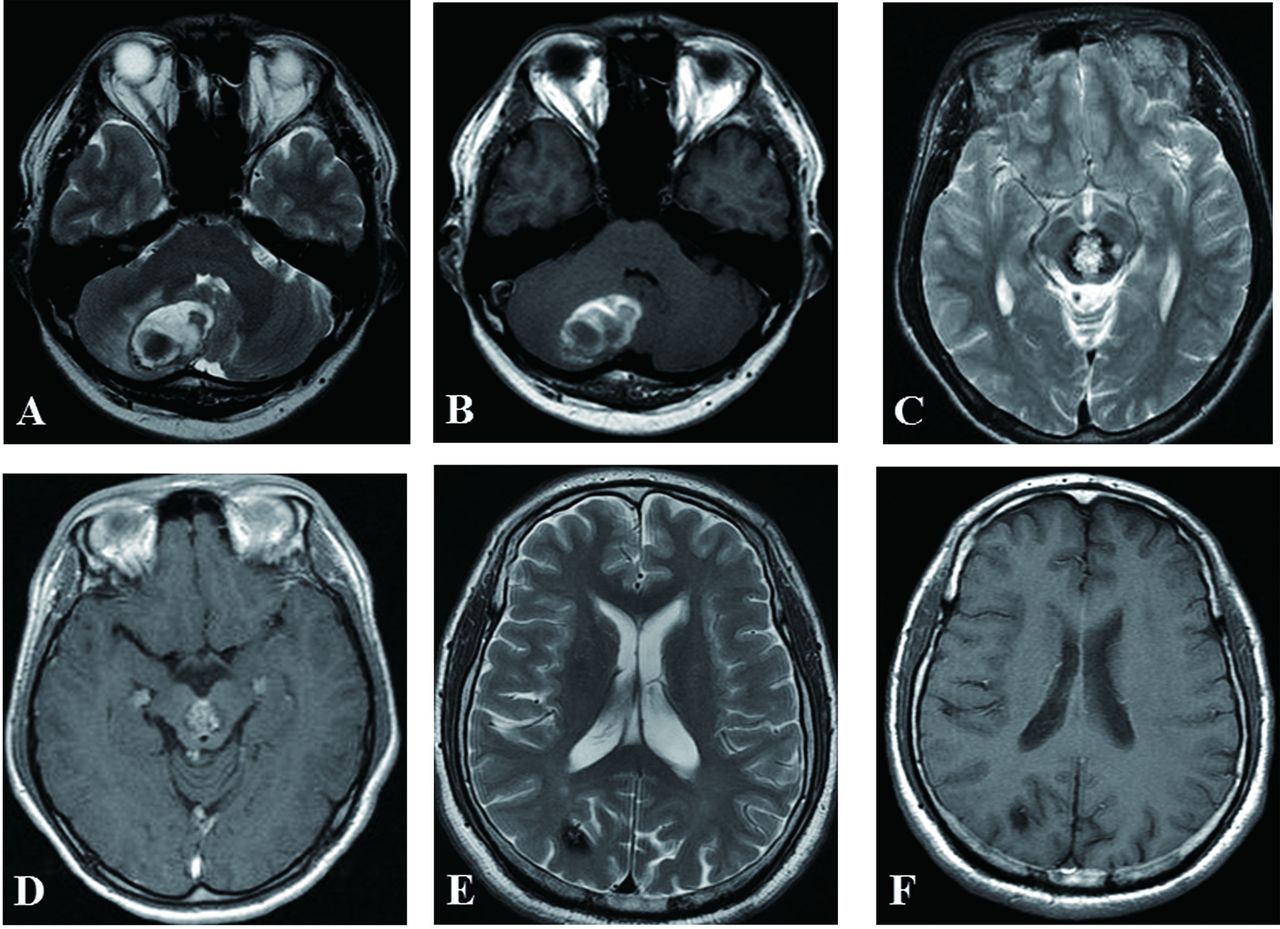
Regarding the radiological data, the size, location, MR appearance, multiplicity and combined venous anomaly were investigated. Location was divided into two groups: superficial and deep location. Deep location refers to CM in the brainstem, cerebellar nuclei, thalamus or basal ganglia.1 MR appearance was divided according to Zabramski's classification.12 However, Zabramski's type IV CM lesion visible only on susceptibility weighted imaging or gradient-echo imaging was not included in this analysis because not all patients underwent susceptibility weighted imaging or gradient-echo imaging MR sequences. Accordingly, MR appearance was categorised into three groups: type I, type II and type III. Type I was defined as CM showing acute or subacute haemorrhage. Uniloculated lesions had primarily a hyperintense lesion on the T1-weighted and T2-weighted images, with an extralesional haemorrhage or fluid-fluid level (figure 1A,B).4 ,13 Type II was defined as loculated haemorrhage lesions with a typical mulberry appearance and thrombosis (figure 1C,D). Type III was defined as showing chronic resolved haemorrhage without typical mulberry appearance and a small punctuate lesion surrounded by a residual haemosiderin rim with or without a hyperintense core on the T2-weighted image (figure 1E,F).4 In the cases of visually indistinguishable lesions from other vascular malformations, a catheter angiography was done to confirm the absence of other vascular malformations. All medical and radiological data were reviewed by one neurosurgeon and one radiologist blinded to the clinical information of the patients, and any discrepancies were re-evaluated by a third reader.
{kind=link}
Types of MR appearance according to Zabramski's classification. (A,B) Type I was defined as uniloculated lesions with primarily hyperintense lesions on T1-weighted and T2-weighted images, extralesional haemorrhage or fluid-fluid level. (C,D) Type II was defined as loculated haemorrhage lesions with a typical mulberry appearance and thrombosis. (E,F) Type III was defined as showing uniloculated lesions without typical mulberry appearance and small punctuate lesion surrounded by a residual haemosiderin rim with or without a hyperintense core on T2-weighted images.
Statistical analysis
Continuous data are presented as the mean±SD. The χ2 and independent t tests were used for categorical and continuous data, respectively. Univariate analysis for related factors of prospective symptomatic CM haemorrhage was conducted with Cox proportional hazards regression. Then multivariate analysis was carried out to confirm the statistical independence of the same variables from each other. Bonferroni correction was used for the correction of multiple comparisons. The annual symptomatic haemorrhage rate was calculated by the number of CM haemorrhagic lesions divided by the number of lesion-years during the follow-up periods. p Values less than 0.05 were regarded as statistically significant. Statistics were performed with SPSS V.19 (SPSS, Chicago, Illinois, USA).
Results
Enrolled and censored patients
A total of 326 patients (female, n=181, 55.5%) were examined. Their mean age was 54.1 years. One hundred and seven (32.8%) and 219 (67.2%) patients presented with haemorrhage-related symptoms and haemorrhage-unrelated symptoms (seizure, n=95, 29.1%; neurological deficit, n=54, 16.6%; headache or vertigo, n=48, 14.7%; asymptomatic or incidental, n=22, 6.8%), respectively. Six patients were lost to follow-up. Two patients died without any relation to CM. Surgical management was carried out in 79 patients, with 27 cases of surgical resection and 52 cases of gamma knife radiosurgery during the follow-up period. The causes of intervention included sustained symptomatic haemorrhage (n=34), intractable seizure (n=26) and progressive neurological deficits (n=19). Calculation of the observation period was from the date of the diagnosis to the date of the intervention or last follow-up.
Clinical characteristics of the CM lesions
Table 1 presents the CM information including location, MR appearance, multiplicity, combined venous anomaly, size (maximum diameter) and incidence of prospective symptomatic haemorrhage in 410 CM lesions during a follow-up of 34.7±24.7 months. One hundred and sixteen (28.3%) and 290 cases (70.7%) of CM that experienced prior haemorrhage or had a superficial location were observed respectively. Multiplicity was noted in 133 (32.4%) cases of CM. Forty-four cases (10.7%) of associated venous angioma were accompanied by CM. Ten cases of new CMs were observed during the follow-up period. Type I MR appearance was noted in 112 (27.3%) lesions. Fifty-three (12.9%) CM lesions experienced prospective symptomatic haemorrhage during the follow-up period.
Clinical characteristics of cavernous malformations (n=410)
Risk factors for prospective symptomatic CM haemorrhage
An univariate analysis revealed that the presence of prior haemorrhage (p<0.001), MR appearance (p<0.001) and deep location (p=0.001) were associated with the occurrence of prospective symptomatic haemorrhage. No statistical difference was observed according to female gender (p=0.486), age (p=0.990), venous angioma (p=0.840), CM size (p=0.173), multiplicity (p=0.123) and hypertension (p=0.522). A multivariate analysis disclosed that prior haemorrhage (adjusted HR, 7.13; 95% CI 3.88 to 13.10; p<0.001) and MR appearance (p<0.001) were significant risk factors of prospective CM haemorrhage (table 2). After multiple comparisons, type I (adjusted HR, 6.05; 95% CI 2.47 to 14.82; p<0.001) and type II (adjusted HR, 3.09; 95% CI 1.24 to 7.72; p=0.016) showed a higher risk of haemorrhage than that of type III. However, no statistically significant difference in the prospective haemorrhage rates was observed between the type I and type II (p=0.105).
Risk factor analysis of prospective symptomatic haemorrhage of cavernous malformations (CMs)
Prospective CM haemorrhage rate in adults
The overall prospective CM haemorrhage rate was estimated at 4.46% per lesion-years. The overall annual haemorrhage rate according to MR appearance was as follows: type I, 9.47%; type II, 4.74%; and type III, 1.43%. The prospective haemorrhage risk decreased after the first 3 years (table 3). Detailed haemorrhage rates based on risk factors were estimated at 3 years as follows: 33.77% in patients with prior symptomatic haemorrhage vs 7.54% in patients without prior symptomatic haemorrhage (p<0.001); type I MR appearance, 27.62% vs type II, 15.44% vs type III, 5.38% (p<0.001).
Prospective haemorrhage rate according to MR appearance in adult patients with cavernous malformations
Discussion
Various factors including different CM haemorrhage definitions, calculation methods and a heterogeneous spectrum of patients with a limited number of subjects can cause discrepancies in assessing risk factors of CM haemorrhage among previous studies. In addition, age could result in different CM haemorrhage rates because of the differences in brain plasticity and clinical manifestations between adult and paediatric patients with CM. However, many studies have addressed CM haemorrhage without taking into consideration the age of the patients. Therefore, a more detailed prospective symptomatic CM haemorrhage rate cannot be given when counselling adult patients.
CM morphology has been categorised into three12 or four4 groups by their radiographic appearance and haemorrhage period. Zabramski et al12 suggested that patients with type I or type II MR appearance are most likely to be symptomatic. Kim et al4 reported that CM lesions with acute haemorrhage or subacute haemorrhage had a bleeding rate of 3.1% or 2.0% per patient per year, respectively. Regarding the CM lesions that were poorly visualised on the T1-weighted or T2-weighted images, only CM lesions surrounded by residual haemosiderin with hyperintensity had a future haemorrhage rate of 1.0% per patient per year. In their study, a statistical difference in the haemorrhage rate was noted according to the MR appearance; however, CM lesions that had acute haemorrhage showed a higher haemorrhage rate than the other CM lesions which had a typical MR appearance or chronic resolved haemorrhage. In this study, we analysed the haemorrhage rate according to Zabramski's classification in a homogenous population of adult patients with CM. The results show that type I CM (adjusted HR, 6.05; p<0.001) and type II CM (adjusted HR, 3.09; p=0.016) were associated with a significantly increased risk of haemorrhage than that of type III CM. Although, no significant difference in the prospective CM haemorrhage rate was observed between type I and type II (p=0.105), type I CM appeared to have higher haemorrhage events than that of type II CM. It is not clear what factors would affect the high haemorrhage rates in CM with a type I MR appearance. Barker et al14 reported that patients with untreated CM tend to experience the phenomenon of haemorrhage clustering, especially within a 2–3 year period after the first haemorrhage event. Therefore, we suspected that prospective haemorrhage events of type I CM that show acute or subacute haemorrhage in the initial image could be observed more during the follow-up period than those of type II CM which are characterised by thrombosis and haemorrhage of varying age. Nevertheless, a static MR appearance for a particular time period could not fully reflect the true haemorrhage rate because type I lesions could appear as type III lesions many years later. Therefore, this shortcoming of assuming a static MR appearance to estimate the prospective haemorrhage rate should be considered.
Pertaining to location, a meta-analysis revealed the detection frequency of CM in the cerebral hemisphere (66%), brainstem (18%), basal ganglia or thalamus (8.2%) and cerebellum (6.0%).5 Although, location can be related to initial presenting symptoms and clinical aggressiveness,5 the relationship with prospective haemorrhage is still controversial. Porter et al1 suggested deep-seated CM as the most relevant factor for CM haemorrhage, but other studies have not shown a meaningful correlation between location and CM haemorrhage.2 ,10 ,11 Our results also showed that haemorrhage risk according to location did not reach statistical significance (p=0.120). A deep location could be related to being symptomatic due to the compression of adjacent structures within a limited space. Accordingly, it is possible that a deep location may exaggerate the inherent risk of haemorrhage, and this should be taken into consideration.
Patients who presented with haemorrhage initially accounted for 36% of the total population with CM.5 Many studies have concluded that prior CM haemorrhage can cause subsequent haemorrhage significantly.1 ,6 ,10 Our data also support the substantial influence of prior CM haemorrhage on prospective symptomatic haemorrhage in an adult population (adjusted HR, 7.13; p<0.001).
A recent prospective study reported that multiple CM had a significant effect on future CM haemorrhage.6 On the contrary, some studies1 ,10 did not show any statistical correlation between multiplicity and prospective haemorrhage. In our cohort, multiplicity was not a significant risk factor for future haemorrhage (HR, 1.13; p=0.711).
Most studies have not found a meaningful association between age and subsequent symptomatic haemorrhage.1 ,10 ,15 On the other hand, Aiba et al11 reported that age under 40 years was a significant factor for subsequent haemorrhage. When comparing the mean age in the included patients among various studies,3 ,12 ,15 ,16 younger patients experienced haemorrhage more. Because CM showed a different clinical presentation and prevalence between the age groups,4 ,7 ,8 a more accurate assessment of future haemorrhage could be achieved in a homogenous population with a certain age range. However, when recruiting patients, age has not been considered as an inclusion criteria in previous studies. Therefore, we only included patients older than 18 years to reduce selection bias. In our study, age was not a relevant factor for prospective CM haemorrhage in adults (p=0.613).
Sex also has been debated in CM haemorrhage. Some researchers suggested that hormonal effects could increase the risk of CM haemorrhage in female patients.15 ,17 On the other hand, Flemming et al6 showed a statistically significant correlation between men and future CM haemorrhage. However, they did not provide a reason for the male predominance in CM. Gross et al5 suggested that no sex predilection was observed based on their meta-analysis. Our results also support that sex has no statistical significance in predicting CM haemorrhage (p=0.445).
Our study had a higher CM haemorrhage rate at 4.46% per lesion-year than that of previous reports.10 ,11 ,15 ,17 Such a result could be due to the relative short follow-up period of 34.7±24.7 months. Flemming et al6 showed that haemorrhage risk can be significantly reduced after 2 years. Barker et al14 also reported that the prospective haemorrhage rate can be exaggerated due to temporal clustering of haemorrhage because the rehaemorrhage rate was initially high and decreased 2–3 years after the first haemorrhage event. Accordingly, a relatively short highly variable follow-up period may exaggerate the haemorrhage risk. In addition, a haemorrhage definition that includes intralesional signal change or a size increase over 20% as well as an extralesional signal change could result in a higher CM haemorrhage rate in our cohort. Ethnic differences may also affect the haemorrhage rate because different genetic predispositions have been recognised according to ethnic group.
Conclusions
Prior symptomatic haemorrhage and MR appearance could be related to prospective symptomatic CM haemorrhage in an adult population. Therefore, patients with a prior history of haemorrhage and type I or type II MR appearance should be monitored closely. The limitations of a relatively short follow-up period and the retrospective nature of this study should also be taken into account. A prospective multicentre observational study is necessary to confirm our results.
Acknowledgments
The authors thank Sung-Eun Kim for her help with the data collection, and her valuable contribution to the statistical analysis.
References
Footnotes
-
JSJ and YSC contributed equally.
-
Contributors JEK devised the original study design. JSJ, JHA, YSC, C-HS and SO performed the data collection and statistical analyses. Y-JS, W-SC, JSB and H-SK interpreted the results. JSJ and JEK wrote the manuscript. CWO made revisions.
-
Funding This study was supported by a grant from Seoul National University (800-20120402) and by a grant from Seoul National University Hospital (0320120310, 2012-0581).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was approved by the Institutional Review Board (IRB) at the participating institution.
-
Provenance and peer review Not commissioned; externally peer reviewed.