Article Text

Abstract
Objective 61 procedures with selective peripheral denervation for cervical dystonia were retrospectively analysed concerning surgical results, pain, quality of life (QoL) and recurrences.
Methods The patients were assessed with the Tsui torticollis scale, Visual Analogue Scale (VAS) for pain and Fugl-Meyer scale for QoL. Evaluations were performed preoperatively, early postoperatively, at 6 months, then at a mean of 42 (13–165) months. All patients underwent electromyogram at baseline, which was repeated in cases who presented with recurrence of symptoms after surgery.
Results Six months of follow-up was available for 55 (90%) of the procedures and late follow-up for 34 (56%). The mean score of the Tsui scale was 10 preoperatively. It improved to 4.5 (p<0.001) at 6 months, and 5.3 (p<0.001) at late follow-up. VAS for pain improved from 6.5 preoperatively to 4.2 (p<0.001) at 6 months and 4 (p<0.01) at late follow-up. The Fugl-Meyer score for QoL improved from 43.3 to 46.6 (p<0.05) at 6 months, and to 51.1 (p<0.05) at late follow-up. Major reinnervation and/or change in the dystonic pattern occurred following 29% of the procedures, and led in 26% of patients to reoperation with either additional denervation or pallidal stimulation.
Conclusions Selective peripheral denervation remains a surgical option in the treatment of cervical dystonia when conservative measures fail. Although the majority of patients experience a significant relief of symptoms, there is a substantial risk of reinnervation and/or change in the pattern of the cervical dystonia.
- DYSTONIA
- NEUROSURGERY
- MOVEMENT DISORDERS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Spasmodic torticollis is a condition characterised by focal dystonia involving the cervical muscles with an incidence of 1.2/100 000.1
The mainstay of treatment is chemical denervation by means of intramuscular injections of botulinum toxin.2 ,3 However, not infrequently, patients either do not respond to botulinum injections, or develop secondary resistance.4–6 In those cases surgery may be considered. Historically, several surgical techniques have been tried aiming at symptom relief, and keeping in mind that no cure from the disease is to be expected.
Today, there are three main surgical approaches used: two approaches involve extradural selective peripheral denervation (SPD), as suggested by Bertrand, or a modification of the Bertrand technique, which includes intradural C1-2 ventral rhizotomy as suggested by Taira and coauthors.7 ,8 The third approach is posteroventral pallidal deep brain stimulation (DBS), which has emerged following the positive effect of posteroventral pallidotomy on Parkinsonian dystonia-dyskinesias9–13 or, as has recently been suggested, subthalamic nucleus DBS.14 The optimal indication, and the proper selection of patients for the different surgical approaches, are still to be established.
Pallidal DBS for cervical dystonia is relatively new, and encouraging long-term results are emerging.13 ,15 ,16 Although SPD has been available for a longer period of time, it has not been widely practiced, and the published reports are few compared with the number of reports dealing with botulinum injections, or with DBS. Also, the last publication of a large series of patients undergoing SPD is 10 years old,17 and in some of the previous studies, the results were vaguely described using semiquantitative evaluation scales. Other reports have used torticollis scales such as the Tsui scale, the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), or the modified TWSTRS.18–20 Finally, the results in terms of pain relief and quality of life (QoL), and analysis of observed recurrences, have seldom been reported.
At our institution we have performed SPD for cervical dystonia since 1993. In this paper we report on the long-term results of 61 procedures in 54 patients with a mean follow-up time of 42 months (range: 12–165).
Methods
Patients
All except three patients selected for surgery were secondary non-responders to botulinum toxin injections as defined by lack of benefit by the referring neurologist. Preoperatively, all patients underwent MR imaging of the cervicocranial region to exclude pathological conditions that could induce a cervical dystonic state. Preoperative investigations included bilateral simultaneous needle-electromyogram (EMG) of the muscles of the neck during habitual position of the head, to define the muscles involved; EMG targeted the sternocleidomastoideus, the splenius capitis, the semispinalis, the levator scapulae and the upper trapezius muscles. The EMG was performed by the neurophysiologist in the presence of the neurosurgeon(s). Since the denervation surgery would preferably be performed with the patient in a sitting position, with risk for air embolism, an echocardiography was performed to exclude cardiac abnormalities such as a patent oval foramen. Patients with pathological hyperactivity in muscles accessible for denervation were selected for peripheral denervation, while those with involvement in muscles not accessible for denervation, such as the scalene muscles, were selected for pallidal stimulation. Table 1 shows the patients’ demographic data and those muscles that were selectively denervated.
Characteristics of 54 patients with spasmodic torticollis treated with a total of 61 procedures of peripheral selective denervation
Surgery
Peripheral denervation of the splenius, the semispinal, and the sternocleidomastoid (SCM) muscles was performed according to the method of Bertrand, and denervation of the levator scapulae as described by Taira et al and Anderson et al.21–23 In addition, a section of the accessory nerve to the trapezius muscle was performed at the posterior border of the SCM muscle in six patients. Before the sectioning of any nerve, bipolar electrical stimulation at 4 Hz was performed to confirm its selective innervation of the affected muscle. The different denervation procedures are presented in table 1.
All except one patient were operated on in the sitting position with monitoring of eventual air-embolism using transoesophageal echocardiography. One patient was operated on in the prone position due to a cardiac patent oval foramen. For safety reasons, all patients had a central venous catheter installed to allow evacuation of an eventual air embolus, if needed.
Evaluation
All patients were videotaped and evaluated by an experienced physiotherapist (EL) preoperatively and early postoperatively, usually on day 5 after surgery, and at all follow-up occasions, that is, at 6 months postoperatively and onwards until the last follow-up. The Tsui scale for cervical dystonia was used for assessment.18 Since 1999, a Visual Analogue Scale (VAS) was administered to rate pain and the Fugl-Meyer life-satisfaction questionnaire24 was used to rate QoL. The Tsui scale has a range of 0–25, where 25 is the worst possible state of the cervical dystonia. The VAS is a subjective rating by the patient on a scale from 0 to 10, where 10 indicates maximal pain. The Fugl-Meyer questionnaire rates 12 different aspects of life quality on a scale from 1 to 6, where 6 represents maximal satisfaction with life.
In patients with recurrence of their torticollis or with a changed pattern of their cervical dystonia, a neurophysiological examination was performed at follow-up.
Results
A total of 54 patients with cervical dystonia underwent SPD. Demographic data are presented in table 1. In 15 patients the surgery was staged in two sessions, one for denervation of the SCM muscle and the other for denervation of posterior cervical muscles. The two-staged procedures were performed within a few months of each other and were analysed as one surgery. In three patients cervical dystonia was the dominant symptom in a context of a generalised DYT-1 negative dystonia. Six patients with recurrence of torticollis and EMG-verified reinnervation of previously denervated muscles were reoperated on with selective denervation more than 15 months after the initial SPD procedure, and one of them was reoperated on twice. These patients were included in the follow-up, which resulted in a total of 61 surgical procedures.
Since our centre is the only one in Scandinavia performing the Bertrand/Taira procedure, and several patients were referred from other Scandinavian countries, we encountered logistical issues that affected our ability to conduct a long-term follow-up. The 6 months follow-up was available for 55 of the 61 surgical procedures (90%), and evaluation at long-term follow-up at a mean of 42 (13–165) months postoperatively could be completed for 34 procedures (56%). One patient died due to an unrelated cause before long-term follow-up could take place.
Surgical results
The surgical results at different time points are presented in table 2. An immediate improvement of the dystonic state was achieved in all but one patient. The positive effects were still present at further follow-ups in a majority of the patients. Individual results are presented in figure 1. Despite the mean improvement in the Tsui scale ratings, the individual results showed a considerable variability.
Surgical results following selective peripheral denervation for spasmodic torticollis in 54 patients/61 procedures

Surgical results following selective peripheral denervation for cervical dystonia in 54 patients/61 procedures. Assessment performed using the Tsui torticollis severity scale preoperatively, 5 days after surgery, at 6 months and late postoperative at mean of 42 (range: 13–165) months after surgery. Upper figure: individual scores of the Tsui scale. Lower figure: percentage changes in severity of dystonia in individual patients.
Pain and QoL
The evaluation of pain by VAS was performed in the last 48 procedures. Thirty-eight (79%) procedures were evaluated at 6 months and 27 (56%) at long-term follow-up, showing a significant improvement of pain at both follow-up time points (table 2). QoL was assessed in the last 50 procedures, at 6 months in 37 patients (74%) and at long-term follow-up in 27 patients (54%). For life-quality in general, most patients reported a modest but significant and sustained improvement. When analysing the different domains individually, only somatic health and psychological health were rated as improved at 6 months follow-up, but not at longer term. However, the total score was significantly improved at 6-month and also at late follow-up (table 3).
Life satisfaction according to Fugl-Meyer scale before and after selective peripheral denervation
Complications/side-effects
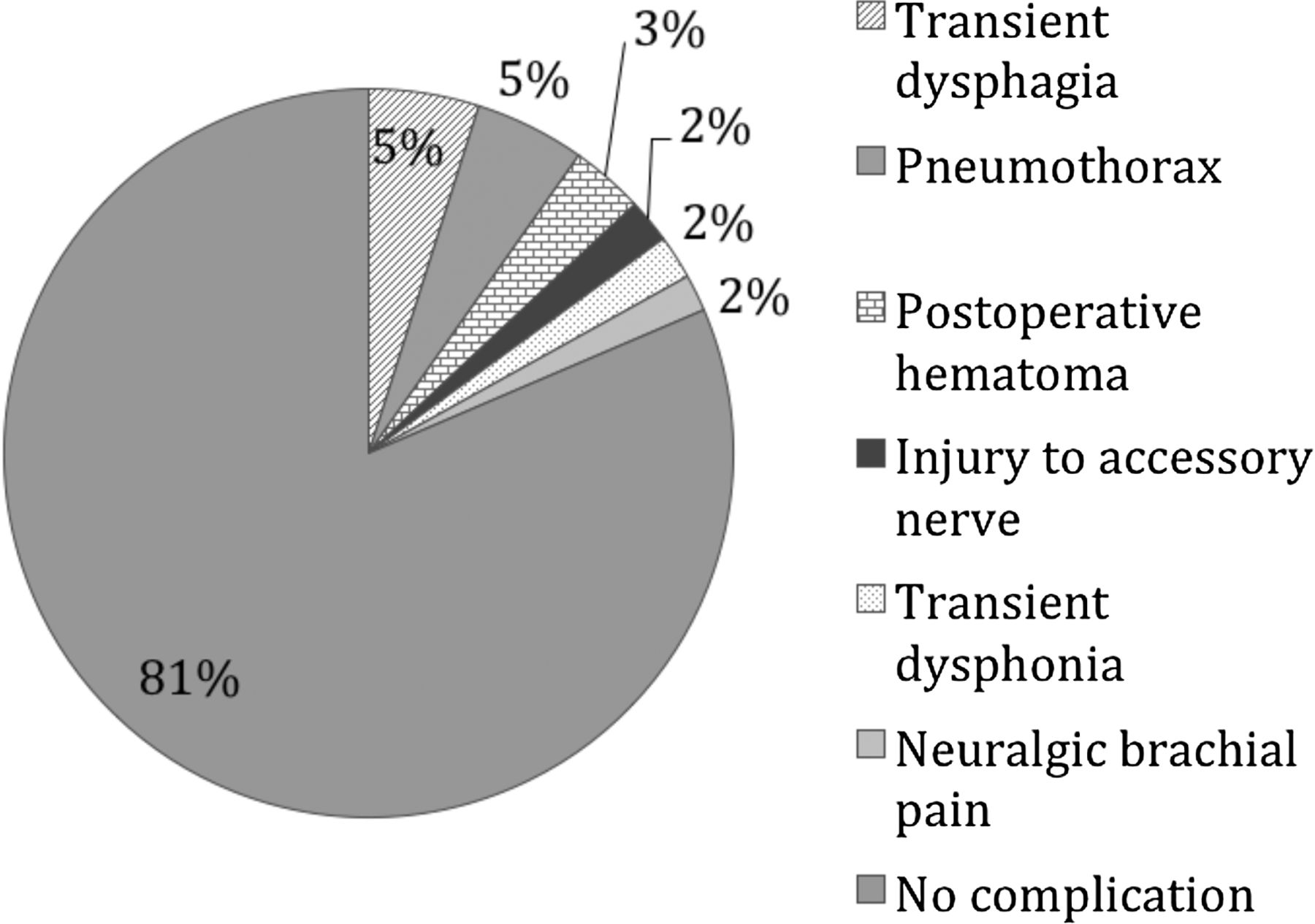
The surgical complications and neurological side-effects were few with exception of the expected sensory loss in the C2 region, which occurred in all patients who had denervation of the posterior C2 branch. A summary is presented in figure 2. Three patients had a transient dysphagia after posterior ramisectomy, and one of those also experienced a transient dysphonia. There were no complications affecting head position. In one patient, the accessory nerve was accidently injured, resulting in a weakness of the upper trapezius muscle, which had partially improved at late follow-up.

{kind=link}
{kind=link}
Postoperative complications following 61 selective denervation procedures in patients with cervical dystonia.
The rate of surgical complications was low, with the most frequent complication being a pneumothorax in three patients (5%), caused by the insertion of the central venous catheter through the subclavian vein. Therefore, the subclavian route for central venous line was abandoned in favour of a peripherally inserted central catheter (PIC-catheter). No case of significant air embolism was encountered in this series.
In two patients, a postoperative haematoma in the SCM region required surgical evacuation. In one patient, the central line inserted through the jugular vein resulted in a postoperative transient severe neuralgic pain in the shoulder region.
Recurrences and changes in pattern of muscular activity
Postoperative recurrences and/or change in the pattern of dystonia are presented in table 4. The major postoperative issue was a change in the pattern of pathological neck muscle activity. Following 31 procedures (51%) there was a change in pattern of dystonia with pathological muscle activity in preoperatively non-active muscles. However, this was mild in most cases (18 patients, 29%). A reinnervation of denervated splenius was found following 20 procedures (33%), and six patients (10%) had a reinnervated SCM muscle. In most patients the change in pattern and/or the reinnervation was mild to moderate as shown in figure 1 and tables 4 and 5, and the patients still showed a significant improvement in their initial torticollis. In total, after 41 (67%) procedures there was a change in muscular pattern, a reinnervation, or both. However, clinically relevant symptoms of major concern, due either to recurrences or changed pattern, occurred after 18 (29%) procedures. The timing of reinnervation and change in muscular pattern was highly individual as demonstrated in figure 1.
The most noticeable findings regarding reinnervation or postoperative progression of disease (change in pattern) following 61 procedures with selective peripheral denervation in 54 patients with cervical dystonia
Numbers and percentages of minor and major re-innervations according to the denervated muscles, following 61 denervation procedures in 54 patients with cervical dystonia
In some patients the recurred symptoms became severe later on and a reoperation was indicated. Eight patients (13%) were reoperated with repeated denervations. Five of those were operated on more than 15 months after primary surgery; they are included in the series and in the follow-up protocol. One of them was reoperated on twice due to aggressive reinnervation of the splenius. After reoperation, three patients (37%) were considerably improved and five were unchanged in their head position at a mean of 29.4 months follow-up (range 12–46). Their mean preoperative Tsui score was 7.4 (range 3–11) and the late postoperative score 5.7 (range 3–11; p=0.104). Their mean total score on the QoL scale improved from 52.8 to 59.3 (p=0.028).
In eight patients (13%) the cervical dystonia progressed and showed a widespread activity involving neck muscles available for denervation. These patients therefore underwent bilateral pallidal stimulation with, in most cases, a positive result as reported in a previous publication.25
Discussion
Surgical results
SPD is a procedure that has been in the neurosurgical armamentarium for dystonia for many years. Lately, pallidal DBS has almost completely supplanted SPD for cervical dystonia. However, DBS is an invasive intracerebral operation and severe complications may occur.26 On the other hand, SPD is a procedure completely outside the central nervous system, being an extradural procedure. Therefore, we believe that a peripheral procedure such as SPD may still be an option to consider for cervical dystonia affecting muscles readily accessible for denervation. However, as with all functional neurosurgery, the selection of patients is important. Almost all patients in our series had strict local pathologic muscle activity in a few muscles accessible for denervation. In patients with widespread cervical activity, that is, with clinically significant muscular activity outside of the muscles accessible for denervation, pallidal DBS should be the surgical procedure of choice.
Owing to the fact that our patients were referred from a very wide geographical area encompassing the Scandinavian countries, we had difficulties in achieving a proper long-term follow-up on all patients. However, as shown in tables 2 and 3, the subgroup of patients who we were able to follow for a longer time had a preoperative status comparable to the overall group, indicating that the patients with long-term follow-up should be representative for the whole series of patients.
In this series of treatment, which included refractory patients in whom surgery was the only remaining option, the outcome can be considered as satisfying for the majority of patients. The long-term results, as assessed by the Tsui torticollis scale, amounted to 45.3% improvement and were as good as, or even better than, what has been shown in studies of patients treated by botulinum injections, in whom improvements were reported to range from 19% to 40%.27 ,28 However, one important drawback with our study is that the evaluations were not blinded.
In many old series of SPD the outcome had been assessed in terms of excellent, marked, moderate, mild and no improvement.17 ,21 Other studies have utilised scales such as TWSTRS29 or the modified TWSTRS that includes functional disability and pain.30–33 We have used the Tsui torticollis scale, which was, at the start of our series, the most frequently used scale in studies on botulinum toxin. The Tsui scale has shown a high degree of congruence with the TWSTRS.34 The mean reduction on the Tsui score in our patients is comparable with the reduction on the TWSTRS severity score in previous studies, which has been reported to range from 22% to 59%.29 ,30 ,35 ,36
Recently, Huh et al37 published a report comparing SPD to pallidal DBS in cervical dystonia, showing no major difference in the results. However, we believe that the surgical treatment should be tailored according to the individual patient, and that the patient groups suitable for either of the two surgical options may differ.
Quality of life
A major goal in all functional neurosurgery is to improve the QoL for patients. The modified TWSTRS includes one section assessing the functional outcome in daily tasks, and studies reporting on this issue indicate a significant improvement in many of the practical tasks of daily life.30 ,36 An improvement in functional outcome may not necessarily imply a better life quality as assessed by patients, and no previous study has specifically addressed this issue. In our study, the patients rated their life quality in general as significantly better postoperatively. Although the outcome according to each specific domain of the QoL scale was not significantly changed at long-term follow-up, the total score encompassing all different domains of life quality was significantly improved. The Fugl-Meyer QoL scale, being a generic scale, may not be ideal for this group of patients, and may fail to capture specific aspects relevant to patients with cervical dystonia.
Complications and side effects
In earlier studies, postoperative dysphagia has been reported to occur in 4–33% of patients.31 ,32 In two of our three patients who postoperatively had dysphagia, we believe the reason for it may have been due to a dramatic change in head position: both patients had a marked retrocollis preoperatively while postoperatively their heads were slightly anteflexed, resulting in changes in the anatomical conditions for swallowing. Another explanation could be a delayed initiation of swallowing, a symptom recognised by Munchau et al.36 The third patient had dysphagia as well as dysphonia. This patient had a retrocollis and underwent a bilateral dorsal ramisectomy. In this patient we believe that strain to the upper cervical nerve roots during surgery may have resulted in oedema of the medulla. Fortunately, all three patients recovered with time.
After sectioning of the posterior branch of C2 all patients developed a sensory loss within the corresponding area. One possible way to avoid this side-effect is to perform intradural posterior rhizotomy according to the description by Taira and Hori.8 However, since in our experience the sensory loss very seldom raises any complaints from patients, we have chosen to remain extradural and thus less invasive.
Recurrences and changes in pattern of dystonia
Reinnervation is known to occur after SPD, possibly caused by incomplete denervation of small nerve branches that may facilitate reinnervation. Munchau et al performed a detailed evaluation of their series and reported a high incidence of 25% for reinnervated SCM muscle and 20% for the splenii. They believed that this problem was related to incomplete denervation of small branches from the cervical plexus, which were overlooked at surgery.38 We have been aware of this problem and carefully looked for such branches by electrical stimulation. In order to find those branches, the SCM muscle has to be sectioned and its medial aspect dissected down to its most caudal part. In all patients where SCM was denervated we also found one or several small branches entering the muscle medially in its lower part. However, in two out of three patients with reinnervation of the SCM, we could nevertheless find a clear reinnervation through one or several pathological thick branches originating from the accessory nerve, indicating that reinnervation does not always depend on incomplete primary denervation.
The splenius seems to be the muscle where most recurrences appear. Munchau et al had reinnervation of the splenii in 20% of patients, a figure close to what we and others have found. This raises the question of the anatomy of the innervation. According to anatomical textbooks the splenius is innervated by dorsal branches from C1 and C2, together with dorsal rami from C3—C7. However, at surgery we have sometimes found nerve branches innervating the splenius from the level of C2—C4, and having a more lateral course than the dorsal rami. We suggest that these may arise from the upper cervical plexus and hence may often be overlooked at surgery. Thus, a double innervation similar to what has been described for the trapezius may be present.39 This could explain the difference in recurrence rate when comparing it with the semispinal muscle, where we had only six cases (9%) with minor reinnervation. In 12 patients the reinnervation of splenii was severe and further surgery was indicated. Nine of those 12 patients also showed an altered pattern in their dystonia. Six patients with reinnervation of splenii were reoperated with repeated denervation and six underwent pallidal DBS due to a simultaneous change in the pattern of their dystonia.
At follow-up, 31 patients showed a change in their pattern of pathological muscle activity with a subsequent change in resting head position, compared to the preoperative position. Although most patients only had minor discomfort out of this, 13 (21%) had major problems, leading to repeated denervation in five patients (8%) and pallidal stimulation in seven (11%). Similar changes after SPD have also been reported previously.32 Indeed, our incidence is high, but on the other hand we have been liberal with performing a postoperative EMG at follow-up, recognising even minor changes. In addition, most of our patients had mild or moderate symptoms. It is difficult to appreciate whether this change in muscular activation pattern is caused by a progress of the disease itself or by a postoperatively induced modulation of the central circuits responsible for the dystonic state.40 A change in pattern has also been reported after successful long-term treatment with botulinum injections, which may suggest common underlying pathophysiological mechanisms in the two treatment situations.41 Since both treatments can be regarded as peripheral denervation by chemical or by surgical means, it is logical that the central response to those treatments can appear rather similar. Additionally, similar changes in dystonic patterns have been reported following long-term pallidal DBS for generalised dystonia, sometimes necessitating a new operation for insertion of additional DBS electrodes in the globi pallidii.42 ,43 However, the eight patients that we reoperated with pallidal DBS due to a more generalised cervical activity did in most cases show a satisfactory outcome, as reported in a previous paper.25
Conclusions
Our results show that SPD may still have a role in treatment of cervical dystonia. A significant number of patients showed satisfactory long-term results. Although no specific domain in ratings of life quality was significantly improved, the patients rated their life quality in general as improved and reported an alleviation of their pain at long-term follow-up. It is noteworthy that our patients all had a severe disease without any relief from botulinum injections or other conservative measures. With this in mind, and considering the documented safety of this procedure, the results of SPD can be considered as satisfactory.
The high incidence of reinnervation of the splenii muscles suggests that special attention to the innervation of this muscle is warranted at surgery.
Acknowledgments
The authors are grateful to Professor Antonio DeSalles who introduced us to the technique of SPD. The Research Foundation of Clinical Neuroscience at Umeå University has supported the work. MIH is supported by the UK Parkinson Appeal and the Monument Trust.
References
Footnotes
Contributors TB and MIH are responsible for preoperative and postoperative surgical evaluation. TB and EL are responsible for data collection. Physiotherapeutic evaluation was done by EL. Interpretation of EMG was performed by EN. The manuscript has been prepared by TB and critically reviewed by all coauthors.
Funding The Research Foundation of Clinical Neuroscience at Umeå University.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data presented in this manuscript was available to all authors.