Article Text

Abstract
Background and purpose Controversy exists over the prognostic significance of the affected hemisphere in stroke. We aimed to determine the relationship between laterality of acute intracerebral haemorrhage (ICH) and poor clinical outcomes.
Methods A subsidiary analysis of the INTERACT Pilot and INTERACT2 studies—randomised controlled trials of patients with spontaneous acute ICH with elevated systolic blood pressure (BP), randomly assigned to intensive (target systolic BP <140 mm Hg) or guideline-based (<180 mm Hg) BP management. Outcomes were the combined and separate end points of death and major disability (modified Rankin scale (mRS) scores of 3–6, 6 and 3–5, respectively) at 90 days.
Results A total of 2708 patients had supratentorial/hemispheric ICH and information on mRS at 90 days. Patients with right hemispheric ICH (1327, 49%) had a higher risk of death at 90 days compared to those with left hemispheric ICH after adjustment for potential confounding variables (OR, 1.77 (95% CI 1.33 to 2.37)). There were no differences between patients with right and left hemispheric ICH regarding the combined end point of death or major disability or major disability in the multivariable-adjusted models (1.07 (0.89 to 1.29) and 0.85 (0.72 to 1.01), respectively).
Conclusions Right hemispheric lesion was associated with increased risk of death in patients with acute ICH. The laterality of the ICH does not appear to affect the level of disability in survivors.
Trial registration number URL: http://www.clinicaltrials.gov. Unique identifier: NCT00226096 and NCT00716079.
- CEREBROVASCULAR DISEASE
Statistics from Altmetric.com
Introduction
Clinical consequences of stroke differ between left and right hemispheric lesions because of the functional lateralisation of the human brain, in particular for language and spatial attention. Several studies report worse outcomes for patients with right hemispheric stroke compared to those with left hemispheric lesions,1–5 but others report either no difference6 or the opposite results.7 Since most studies of hemispheric difference in stroke outcome are mainly based on ischaemic stroke cohorts,1–5 ,7 there has been significant uncertainty about the relevance of their findings to patients with acute intracerebral haemorrhage (ICH). The objective of our study was to elucidate the association of hemispheric lateralisation of lesions with clinical outcomes in approximately 3000 patients with acute ICH, represented by pooling data from the pilot and the main phases of the Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT) studies.8–10 We aimed to test the hypothesis that patients with right-sided ICH would have worse clinical outcomes.
Methods
Study design and participants
INTERACT Pilot and INTERACT2 were international, multicentre, open, blinded end point, randomised controlled trials, as described in detail elsewhere.8–10 In brief, 404 and 2839 patients, respectively, with spontaneous ICH within 6 h of onset and elevated systolic blood pressure (SBP, 150–220 mm Hg) were randomly assigned to receive intensive (target SBP <140 mm Hg within 1 h) or guideline-recommended (target SBP <180 mm Hg) BP lowering therapy.
Procedures
Demographic and clinical characteristics were recorded at the time of enrolment, with stroke severity measured with the Glasgow Coma Scale (GCS) and National Institutes of Health stroke scale (NIHSS) at baseline. CT scans were performed according to standardised techniques at baseline, and centrally without identifying information. In patients with deep or lobar ICH haematoma, laterality was determined on the basis of a baseline scan.
Outcomes of interest in these analyses were death, death or major disability and major disability (modified Rankin scale (mRS) of 6, 3–6 and 3–5, respectively) at 90 days.
Primary causes of death (available only in INTERACT2 participants) were classified into three categories: (1) direct effects of initial ICH, defined as any death after the onset of the randomised ICH event in a patient who had progressive neurological deterioration and either the baseline or follow-up brain scan shows a haematoma with mass effect, midline shift or significant extension of the initial haematoma in the absence of a clear extracranial cause for the death; (2) recurrent cardiovascular event, defined by clear clinical evidence of a recurrent stroke, a coronary vascular event or sudden death, according to standard definitions; (3) other causes, defined by clear evidence of death due to a non-neurological cause, including pneumonia, sepsis or injury.
Statistical analysis
The association of right hemispheric ICH with clinical outcomes was estimated using logistic regression models. Considering the hemispheric bias in the NIHSS score, only GCS was included as a measure of stroke severity and a sensitivity analysis was conducted including NIHSS. Variables were included in the adjusted model if they were either significant in univariable analysis (SBP, GCS score (3 categories of <9, 9–12 and >12)) or prespecified variables determined to be clinically important (age, sex, region, time from onset to randomisation, glucose, baseline haematoma volume, deep (hemispheric) haematoma location, intraventricular extension, trial and randomised treatment). When developing the sensitivity analyses models that included NIHSS, an interaction was found between NIHSS and haematoma laterality; OR of right and left hemispheric ICH were separately calculated for NIHSS split into two categories at the median (<11 and ≥11). Survival probability curves were drawn using the Kaplan-Meier analysis and compared using the Cochran-Mantel-Haenszel log-rank test. A standard level of significance (p<0.05) was used and the data were reported with OR and 95% CIs. All data were analysed with the use of SAS software V.9.3 (SAS Institute, Cary, North Carolina, USA).
Results
Baseline characteristics
Among 3233 participants of the combined INTERACT studies, 2708 (84%) patients with deep or lobar ICH and information on mRS available at 90 days were included in these analyses (see online supplementary figure S1); the main exclusions were unavailability of the baseline scan (n=274) or non-hemispheric site of ICH (n=204). A total of 1327 (49%) patients had right hemispheric ICH; they had lower SBP, higher GCS scores and lower NIHSS scores at baseline compared to left hemispheric ICH (table 1). Distribution of NIHSS scores between hemispheric subgroups is shown in online supplementary figure S2.
Baseline characteristics
Right hemispheric ICH and clinical outcomes
A total of 327 (12%), 1468 (54%) and 1141 (42%) patients had death, death or major disability and major disability at 90 days, respectively. Associations between right hemispheric ICH and clinical outcomes were shown in table 2. Patients with right hemispheric ICH had a higher risk of death at 90 days as compared to those with left hemispheric ICH (OR 1.28, 95% CI 1.02 to 1.62). This increased risk of death remained statistically significant after multivariable-adjustment (OR 1.77, 95% CI 1.33 to 2.37). This model had a C-statistic of 0.814, while the model excluding lateralisation had a C-statistic of 0.809. No clear association was observed for death or major disability (multivariable-adjusted OR 1.07, 0.89 to 1.29). There was a trend towards an association for major disability (OR 0.85, 0.72 to 1.01).
Association between right hemisphere haematoma and clinical outcomes
Sensitivity analysis
There were interactions between NIHSS score and hemispheric lateralisation of ICH in the adjusted models with death (p=0.004) and with death or major disability (p<0.0001) as the outcomes. We developed models for each outcome at 90 days with NIHSS in two categories (low <11, or high ≥11; see online only supplementary table S1 and figure S3). In the high NIHSS score group, patients with right ICH had significantly higher risks for death and for death or major disability, as compared to those with left ICH after adjustment for confounders.
Survival analysis
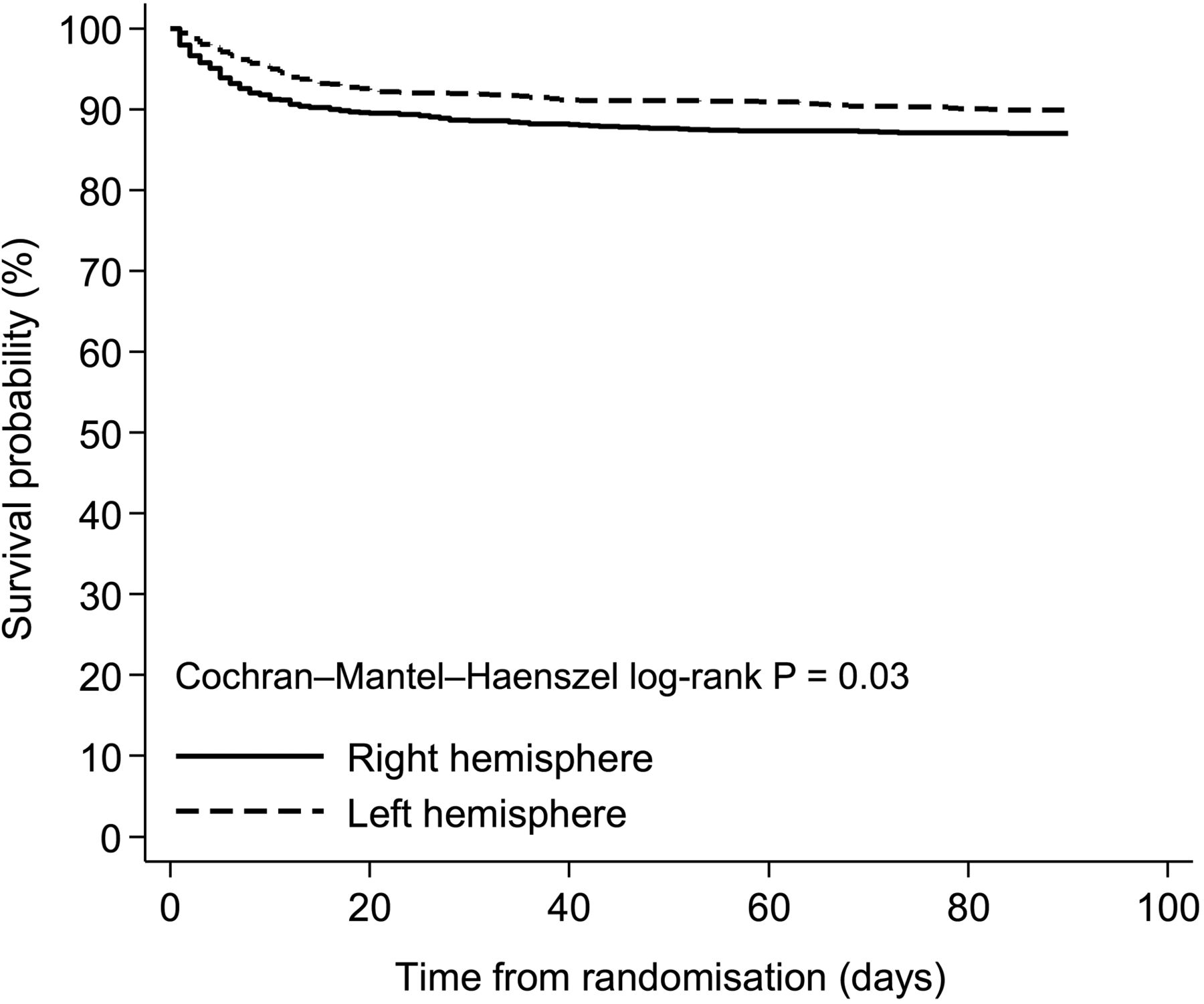
The Kaplan-Meier analysis showed a significant difference between patients with right and left hemispheric ICH for death (Cochran-Mantel-Haenszel log-rank p=0.03; figure 1). Of the patients who died within 90 days of ICH, those with right hemispheric ICH had a shorter time to death, with a median of 6 days compared to 10 days for those with left hemispheric ICH (p=0.009).

{kind=link}
Kaplan-Meier curves for death in patients with right and left intracerebral haemorrhage.
Primary causes of death
Table 3 shows the primary causes of death in INTERACT2 participants (n=297). Patients with right ICH were more likely to die from the direct effects of initial ICH.
Primary causes of death for patients in INTERACT2
Acute stroke care during the first 7 days
Online only supplementary table S2 shows key aspects of acute stroke care during the first 7 days in INTERACT2 participants (n=2361). Patients with right hemispheric ICH were less likely to have been admitted to an intensive care unit, and to have received nasogastric feeding or pulse oximetry.
Discussion
The present pooled analysis of the two INTERACT studies included over 3000 patients with acute ICH and demonstrated an association of right hemispheric ICH with higher mortality. In patients with a high NIHSS score, the right hemispheric ICH was significantly associated with higher risks for death and for death or major disability when compared to those with left hemispheric ICH. Patients with right hemispheric ICH were more likely to die from the direct effect of the initial ICH and less likely to receive several components of stroke care within the first 7 days. However, the laterality of the ICH does not appear to affect the level of disability in survivors.
There have been conflicting reports on the relationship between hemispheric lateralisation of stroke and mortality. Our analysis is the largest study to specifically address this issue in acute ICH where there are limited data. A previous analysis of 337 patients with acute ischaemic stroke in the middle cerebral artery territory found that a right hemispheric lesion was associated with higher mortality at both 6 months and 3 years of follow-up,4 which is confirmed in an earlier study of 162 consecutive patients with stroke2 However, an analysis of 1644 placebo group patients from several clinical trials showed no difference in mortality between the right and the left hemisphere (90% ischaemic).6 Intriguingly, it was reported that the left hemispheric lesion was associated with a greater risk of sudden death in participants of the North American Symptomatic Carotid Endarterectomy Trial (NASCET) in several years of follow-up.7
It has been hypothesised that the increased risk of death in patients with right hemispheric stroke is due to the impairment of autonomic cardiovascular control, especially with regard to the damage of the right insular cortex (or ‘cardunculus’), which might predispose patients to cardiac arrest from ventricular arrhythmia.4 ,11–14 Our study showed no difference in the frequency of death from recurrent cardiovascular events between hemispheric lesions, which is consistent with another study of stroke lateralisation and adverse cardiac events within 7 days.6 Another hypothesis is that there is differential stroke management according to hemispheric location, thereby creating a survival difference. Since the NIHSS awards seven points for tests directly related to language function and only two points for sensory inattention, patients with right hemispheric stroke could receive a relatively low NIHSS score compared to the same-size lesion in the left hemisphere.15 ,16 Thus, the hemispheric bias of NIHSS may affect treatment decisions. It has been reported that patients with right hemispheric ischaemic stroke were less likely to receive thrombolysis as compared to those involving the left hemisphere.17 ,18 In our study, the right hemispheric ICH had less severe stroke scale scores (higher GCS and lower NIHSS scores) and a lower frequency of several treatments (admission to intensive care and nasogastric feeding) compared to the left hemispheric ICH, although the haematoma volumes were identical between them. Thus, clinicians may underestimate the severity of illness in patients with right hemispheric ICH, leading to delays and/or less intensive stroke care compared to those with left hemispheric ICH, resulting in differential survival between them. Another possibility is that patients with right hemispheric ICH had retained capacity for speech and were able to decline treatment, whereas aphasic patients from left hemispheric ICH were more likely to be treated through surrogate consent.
There was a trend towards better functional outcome in patients with right hemispheric ICH in this study. One possible reason is that the mRS could be biased by handedness, such that patients with right hemispheric ICH are less likely to be disabled in dominant hand function so that they scored better on the mRS as compared to those with left hemispheric ICH. Another explanation is survival bias, where patients with right hemispheric ICH had higher mortality as compared to those with involvement of the left hemisphere, resulting in an apparently better functional outcome in the former group.
The strengths of the INTERACT pooled analysis include the large sample size and heterogeneous patient population with rigorous prospective evaluations after acute ICH. However, there are also several limitations. First, as the present analysis was not prespecified, it is open to chance or biased associations, and therefore the findings require further validation. Second, as component scores on the NIHSS were not available in our study, we were not able to confirm the results of another study that removed language-related and inattention-related items from the original 15-item NIHSS to assess hemispheric bias from the NIHSS in multivariable models for outcomes.6 Third, the 90 day mortality in this study is much lower than that reported in most observational studies on ICH where 30 day mortality is estimated to be approximately 40%.19 This is most likely due to the INTERACT studies having eligibility criteria that excluded more severe cases of ICH and where most participants were from China. Additionally, the proportion of deep ICH was as high as 90% in our data set, which most likely reflects the inclusion of ‘hypertensive’ patients in a trial of BP lowering and the exclusion of surgical candidates (more often with lobar ICH). Thus, in the absence of external validation, these findings should be interpreted with caution.
In conclusion, patients with right hemispheric ICH had higher mortality at 90 days than those with left hemispheric ICH in the INTERACT pooled cohort. This was particularly marked in patients with more severe NIHSS scores at presentation. We add to the evidence confirming that the NIHSS underestimates neurological severity for right hemispheric ICH, which may influence the quality of care between patients with right and left hemispheric ICH. Higher mortality in right hemispheric ICH might be avoidable by hemispheric unbiased standardised treatment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
- Data supplement 3 - Online tables
Footnotes
Collaborators INTERACT Investigators (see online only reference ‘Coinvestigators.pdf’).
Contributors SS, EH, HA and CSA contributed to the concept and rationale for the study. SS, EH and HA contributed to data analysis. SS, EH, HA, CD, YH, VP, ZL, QT, YX, MGH, TR, CZ, RIL, JC and CSA contributed to the interpretation of the results. All authors participated in the drafting and approval of the final manuscript and take responsibility for the content and interpretation of this article.
Funding The INTERACT studies were funded by the National Health and Medical Research Council of Australia. SS holds a fellowship from the Uehara Memorial Foundation of Japan. HA holds an Australian Research Council Future Fellowship. CSA holds an NHMRC Senior Principal Research Fellowship.
Competing interests TR reports consultancy payments from Boehringer Ingelheim and Daiichi Sankyo, and his institution has received grant funding from the National Institute of Health Research, British Heart Foundation, Stroke Association and the Engineering and Physical Sciences Research Council. JC reports grants from the National Health and Medical Research Council of Australia during the conduct of the study; grants from Servier International outside the submitted work and being a chief or Co-Chief Investigator for other large stroke trials, including the PROGRESS, INTERACT1 and ENCHANTED trials. CSA reports grant support from the National Health and Medical Research Council; advisory board fees from Pfizer and The Medicines Company, and speaker fees from Takeda China and Covidien; grants; and non-financial support from The George Institute, Sydney, Australia during the conduct of the study.
Patient consent Obtained.
Ethics approval The study protocol was approved by the appropriate ethics committee at each participating site.
Provenance and peer review Not commissioned; externally peer reviewed.