Article Text

Abstract
Objective: The clinical significance of microbleeds (MBs) in the development of psychiatric conditions following a stroke is unknown. Lesions located in various cortical and subcortical areas are thought to be involved in the pathophysiology of post-stroke emotional lability (PSEL). This study examined the association between PSEL and MBs.
Methods: A total of 519 Chinese patients with acute ischaemic stroke consecutively admitted to the acute stroke unit of a university affiliated regional hospital in Hong Kong were screened for PSEL 3 months after their index stroke. The number and location of MBs were evaluated with MRI.
Results: According to Kim’s criteria, 74 (14.3%) patients had PSEL. In comparison with the non-PSEL group, patients in the PSEL group were more likely to have MBs in the thalamus as a whole (16.2% vs 6.5%; p = 0.004), its anterior (6.9% vs 2.0%, p = 0.02) and paramedian territories (8.1% vs 3.1%; p = 0.04), and a higher number of MBs in the entire brain (1.7+3.4 vs 1.3+5.0; p = 0.031). MBs in the thalamus remained an independent predictor of PSEL in the multivariate analysis, with an odds ratio of 4.7 (p = 0.002).
Conclusion: Our results suggest that MBs in the thalamus may play a role in the development of PSEL. The importance of MBs in PSEL and other psychiatric conditions in stroke survivors warrants further investigation.
Statistics from Altmetric.com
Cerebral microbleeds (MBs) are focal deposits of haemosiderin that indicate prior micro-haemorrhages. MBs are related to cerebral amyloid angiopathy, hypertension and atherosclerosis.1
MBs are common in ischaemic stroke.2 They may provide useful diagnostic and prognostic information, with potential therapeutic implications for the treatment of stroke.3 MBs are associated with advanced small artery disease of the brain4 and leukoaraiosis,5 and they may also predict recurrent stroke.6
MBs have generally been considered to be clinically silent. Recent evidence suggests that MBs may be one of the important factors that cause cognitive impairments in subcortical vascular dementia7 where they are associated with cognitive dysfunction, particularly executive dysfunction.8 The clinical significance of MBs in psychiatric conditions following a stroke remains unknown.
Emotional lability (EL) is defined as virtually uncontrollable episodes of laughter, crying or both.9 Laughing or crying occurs without a clear relationship to a stimulus or the outbursts can be triggered by minor, non-specific stimuli. In addition, patients may not experience any concomitant or subsequent change in feeling. EL is a distressing and embarrassing complaint for the patient, is often socially disabling10 and may interfere with rehabilitation. Other terms that have been used for this clinical syndrome include emotionalism, pathological laughing and crying, pseudobulbar affect, pathological emotionality and emotional incontinence.9 11 12 Common methods of evaluating EL are clinical interviews, chart reviews, the Pathological Laughing and Crying Scale13 and other questionnaires.11
EL affects 11–52% of all stroke survivors.11 14 Post-stroke emotional lability (PSEL) usually starts within weeks of a stroke,15 may last from 1 week to a few years,15 16 has a fluctuating clinical course12 and may respond to selective serotonin reuptake inhibitors.17
The neuropathological substrate of EL has yet to be determined. Wilson18 proposed that it was caused by bilateral corticobulbar motor tract lesions. Recently, Parvizi and colleagues19 hypothesised that disconnection in the cortico-pontine-cerebellar pathways may also be an important link in the pathogenesis. Black20 suggested three levels of injury (cortical, bulbar and hypothalamic) as possible causes of pathological laughter, with the common factor being disinhibition in the upper brainstem level. House and colleagues21 proposed that frontal lesions may produce disinhibition of emotional control similar to the way that frontal lobe damage produces disinhibition of social behaviour. EL has been found to co-occur with frontal release signs such as grasp reflex.22 Neuroimaging studies have shown that EL may be related to specific frontal areas, such as the anterior cingulate and dorsolateral prefrontal cortices23 and the medial inferior frontal areas.24 PSEL is associated with anterior cortical,9 25 frontal lobe26 and lenticulocapsular lesions,9 particularly those that involve the dorsal globus pallidus.27 Brainstem and parietal lesions can also generate EL.9 24 28
The fronto-subcortical circuits are known to mediate emotion and affective behaviour.29 These circuits link specific areas of the frontal cortex to the striatum, basal ganglia and thalamus.30 Several lines of evidence suggest that the fronto-subcortical circuits are involved in the development of EL.23 24 26 27 Thalamic lesions can give rise to a variety of neuropsychiatric complications following stroke, including disinhibition, affective changes, apathy, amnesia and dementia.31
The role of MBs in PSEL is unknown. The aim of this case control study was to assess the relationship between MBs and PSEL in stroke survivors.
Material and methods
Subjects
In total, 2337 patients with first ever or recurrent acute ischaemic stroke were admitted to the Acute Stroke Unit of the Prince of Wales Hospital from December 2004 to June 2007. The Prince of Wales Hospital is a university affiliated general hospital serving a population of 800 000 in Hong Kong. Of these, 874 of the admitted stroke patients received an MRI examination. Of patients with an MRI, 519 (59.4%) were recruited from patients admitted with a first ever or recurrent ischaemic stroke. The inclusion criteria for the study were: (1) Chinese ethnicity; (2) age 18 years or above; (3) well documented (clinical presentation and CT scan of the brain) first or recurrent acute stroke occurring within 7 days before admission; (4) Cantonese as the primary language; and (5) ability and willingness to give consent. Exclusion criteria included: (1) transient ischaemic attacks, since MBs are rare in transient ischaemic attacks4; (2) cerebral haemorrhage, subdural haematoma or subarachnoid haemorrhage; and (3) history of a central nervous system disease such as tumour, trauma, hydrocephalus, multiple sclerosis, Parkinson’s disease, etc. All participants were screened for PSEL by a qualified psychiatrist (WKT).
The study protocol was approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong. Consent of all subjects was obtained in accordance with the Declaration of Helsinki.
Collection of demographic and clinical data
A research nurse, who was blind to the psychiatrist’s diagnoses, collected the demographic data (age, sex and education level) and assessed the severity of stroke with the National Institute of Health Stroke Scale (NIHSS).32
Assessment of PSEL
Psychiatric interviews were conducted 3 months after the stroke at a research clinic. A psychiatrist (WKT) administered a brief questionnaire to all participants. The diagnostic criteria of PSEL were based on those proposed by Kim. 27 33 PSEL was considered to be present if patients exhibited excessive or inappropriate laughing, crying or both compared with their premorbid state. If the patient agreed that excessive or inappropriate laughing or crying occurred on two or more occasions since the latest episode of stroke, the diagnosis of PSEL was established. A research assistant (RA), trained by the principal author, administered the Chinese version of the Mini-Mental State Examination (MMSE)34 to measure the participants’ global cognitive function.
Radiological examination
MRI, including diffusion weighted imaging (DWI) and sequence of proton density, was performed on each participant with a 1.5 T system (Sonata, Siemens Medical, Erlangen, Germany) within 7 days of admission.
DWI spin echo EPI (TR/TE/excitation = 180/122/4, matrix = 128×128, FOV = 230 mm, slice thickness/gap = 5 mm/1 mm, EPI factor = 90, acquisition time = 55 s) with three orthogonally applied gradients were used with a b value of 1000 and 500. Axial gradient echo images were acquired as the second sequence with imaging parameters of TR/TE/excitation = 350/30/2, flip angle of 30°, slice thickness/gap = 5 mm/0.5 mm, FOV = 230 mm, matrix 256×256 and acquisition time = 5 min 4 s. Axial SE T1 (TR/TE/excitation = 425/14/2, FOV = 230 mm, slice thickness/gap = 5 mm/0.5 mm, matrix = 256×256 and acquisition time = 4 min 28 s) and TSE T2 (TR/TE/excitation = 2500/120/1, turbo factor of 15, FOV = 230 mm, slice thickness/gap = 5 mm/0.5 mm, matrix of 256×256 and acquisition time = 1 min 39 s) images were also acquired.
A neurologist (YKC), who was blind to the psychiatric diagnoses, assessed the MRIs, which included the following.
Brain infarcts. Acute infarcts affecting the frontal, temporal, parietal and occipital lobes, coronary radiata, centrums semiovale, internal capsule, basal ganglia, thalamus, brainstem and cerebellum were recorded.35 The presence or absence of acute infarcts in these locations was recorded. Multiple infarcts or infarct(s) involving more than one location were counted in all locations they occurred. The total area of acute infarcts on DWI was measured with manual outlines, with restricted water diffusion identified on diffusion weighted images with b values of 1000. The total volume was calculated by multiplying the total area by the sum of the slice thickness and gap.
MBs. MBs were defined as small (2–10 mm) hypointense lesions on T2 weighted gradient echo sequence but symmetric basal ganglia calcification and flow void artefacts of the pial blood vessels were excluded.36 The locations of MBs included the frontal, parietal, temporal and occipital lobes, basal ganglia, thalamus as a whole and its anterior, paramedian, lateral and posterior territories,37 brainstem and cerebellum. The number of MBs in each location was recorded. Inter-rater and intra-rater reliability tests of the measurement of MBs were performed on 30 participants. Inter-rater and intra-rater agreement was good (presence of MBs: inter-rater kappa = 0.78; intra-rater kappa = 0.85; number of MBs: inter-rater intraclass correlation coefficient (ICC) = 0.91; intra-rater ICC = 0.95).
White matter lesions (WML). The severity of WMLs was graded using the four point scale developed by Fazekas and colleagues.38 Periventricular and deep white matter hyperintensities were scored on axial proton density images. Inter-rater and intra-rater reliability tests were performed on 20 participants resulting in good agreement (kappa = 0.70–1.00).
Statistical analysis
All statistical tests were performed by SPSS for Windows (release 14.0; SPSS Inc, Chicago, Illinois, USA). Demographic and clinical variables (age, sex, education level, and NIHSS and MMSE scores) and the scores of the psychometric tests of the PSEL subjects were compared with those of matched controls using the χ2 test, Fisher’s exact test, Student’s t test and the Mann–Whitney U test, as appropriate. Risk factors with a value of p<0.10 were then analysed by multivariate logistic regression analysis using a forward stepwise selection strategy. If the correlations between any of these putative risk factors were ⩾0.50, then additional models were examined to rule out co-linearity. In the analysis, the odds ratio of any independent risk factor was interpreted as the risk of subsequent PSEL when all other risk factors were held constant. The level of significance was set at 0.05.
Results
Patient who were excluded from the study were older (73.9 (12.0) vs 66.0 (11.7) years; p<0.001), were more likely to be female (52.8% vs 39.3%; p<0.001) and had a higher NIHSS score (10.1 (9.3) vs 4.5 (3.4); p<0.001).
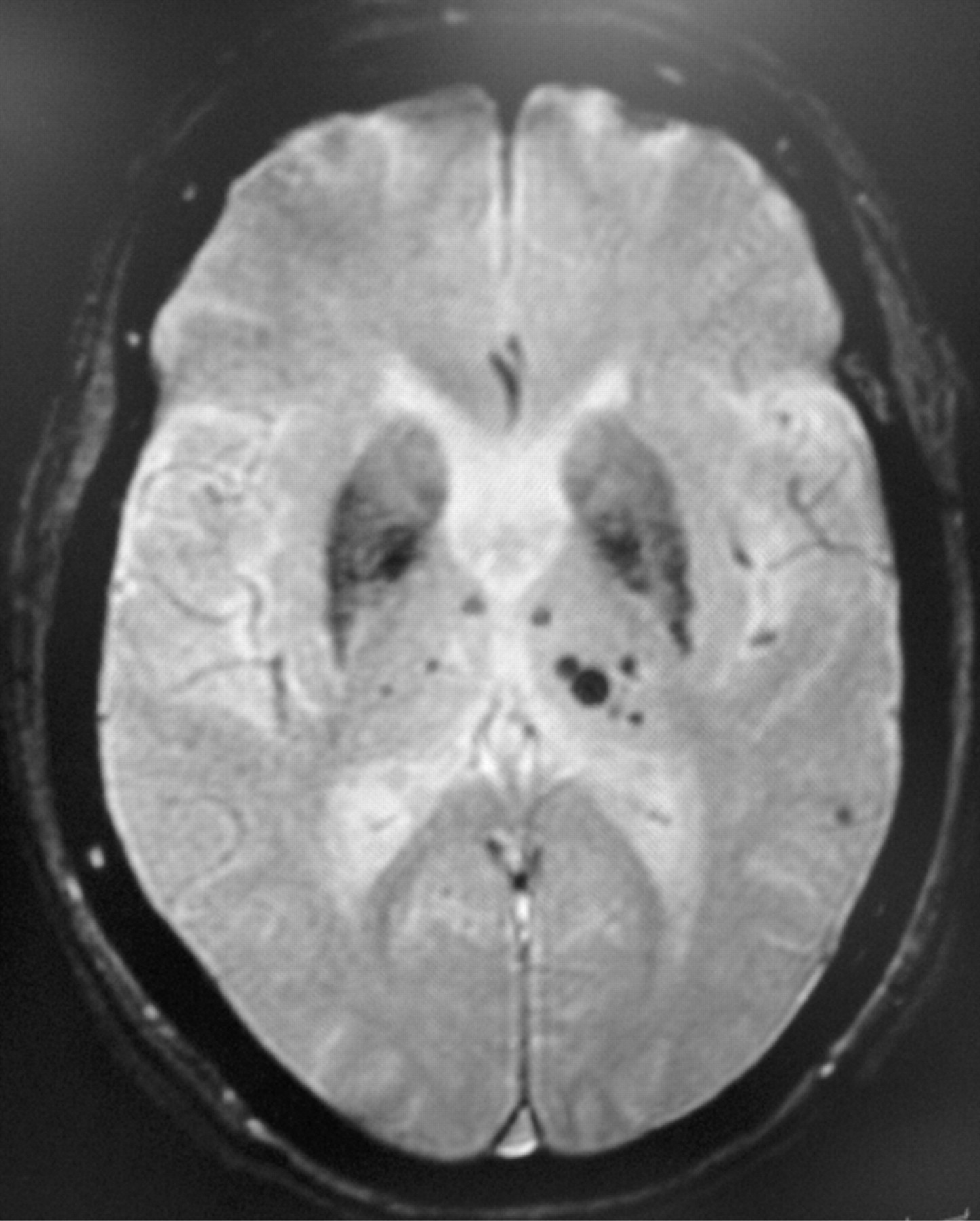
Of the 519 patients screened, 74 (14.3%) had PSEL. The demographic and MRI characteristics and stroke related data stratified by PSEL status are shown in tables 1 and 2. The PSEL group had significantly more female subjects, a lower level of education and lower MMSE but higher NIHSS scores. The number of MBs was significantly higher in the PSEL group. MBs located in the thalamus were associated with PSEL, particularly the anterior and paramedian territories (fig 1). The number of MBs in the thalamus of subjects with PSEL ranged from 1 to 10, with a mean of 3.2 (2.7). The association between MBs in the entire brain and in the frontal lobe and PSEL was of borderline significance. PSEL was not associated with the volume and location of infarcts, number of lacunar infarcts or the extent of WMLs.
{kind=link}
T2* weighted gradient echo MRI of a 78-year-old woman with post-stroke emotional lability shows multiple microbleeds in bilateral thalami (most in the left), ranging from 2 to 8 mm in diameter.
Demographic, clinical and MRI variables of subjects with and without post-stroke emotional lability
Demographic, clinical and magnetic resonance imaging variables of subjects with and without post-stroke emotional lability
MMSE score and education were correlated (r = 0.569, p<0.01). The correlation between MBs in the thalamus and MBs in the entire brain was 0.524 (p<0.01). The following variables were entered into the regression model: sex, MMSE, NIHSS and MBs in the thalamus, and the frontal lobe and number of MBs. MBs in the thalamus and MMSE were significant independent predictors of PSEL. The odds ratio of MBs in the thalamus was 4.7 (table 3).
Multivariate logistic model of the clinical and radiological determinants of post-stroke emotional lability
Discussion
To the best of our knowledge, this was the first study to examine the role of MBs in stroke patients with EL. This observation challenges the prevailing view that microbleeds are clinically silent.4 The histopathological data revealed that MBs involve not only haemosiderin deposition but also affect the surrounding gliosis and cause frank necrosis or infarction, which means that they may be of clinical importance.39
The findings of this study suggest that microhaemorrhages are important components of the pathomechanism of PSEL. PSEL was associated with MBs in the thalamus, particularly the anterior and paramedian territories. The thalamus can be divided into different regions, according to the pattern of blood supply. The paramedian territory is supplied by the thalamoperforating arteries, which originate from the first part of the posterior cerebral artery.37 The paramedian thalamic territory has connections between cortical (prefrontal, orbitofrontal and mediofrontal cortex) and subcortical (ventral pallidum and internal globus pallidus) structures.40 41 Paramedian thalamic lesions can cause personality changes and disinhibition,42 such as crying spells, labile affect and even frank manic symptoms.43 It is thought that these behavioural symptoms were due to thalamofrontal disconnection.31 A wide range of behavioural and personality changes have been associated with lesions in the anterior territory, including euphoria, lack of emotional concern and emotional central facial paralysis. The latter is characterised by a facial weakness during emotional displays such as laughing or crying.44 Patients with executive dysfunction have more microbleeds in the frontal region.8 There is evidence suggesting that executive functions are impaired in patients with EL.44 45 Further exploration of the relationship between MBs in the frontal lobe, executive functions and PSEL is warranted.
The main limitation of this study is its relatively small sample size, which resulted in a low power in detecting the potential differences between groups with respect to frontal lobe MBs. Furthermore, the assessment of PSEL was made only once, at the 3 month follow-up. As patients who died before the 3 month follow-up were not included in the study, the sample was biased to an unknown degree. In addition, patients who could not give consent due to dementia or aphasia associated left side infarcts were excluded. The excluded group had more female patients, they were older and had more severe stroke. As cognitive impairment,21 left side lesions,21 female sex,9 younger age14 and neurological deficits9 were associated with PSEL, this selection bias may limit the generalisability of the findings.
It is interesting to note that thalamic MBs, a pre-stroke lesion, can contribute to the development of an event such as EL after stroke. It is well known that pre-stroke abnormalities do contribute to post-stroke psychiatric problems, including dementia and depression. WMLs and cerebral atrophy predict post-stroke dementia.46 Similarly, WMLs predict post-stroke depressive symptoms.47
In conclusion, the results of this study suggest that MBs at the thalamus may contribute to the development of PSEL. This assumption, while biologically plausible, should be regarded as speculative at this point. Further exploration of the importance of MBs in PSEL and other psychiatric sequels in stroke survivors is clearly warranted.
REFERENCES
Supplementary materials
Lay Summary 80;10:1082
Files in this Data Supplement:
Footnotes
Funding This work was supported by a direct grant for research 2005/2006 from the Chinese University of Hong Kong.
Competing interests None.
Ethics approval The study protocol was approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong.
Provenance and Peer review Not commissioned; externally peer reviewed.