Article Text

Abstract
Background The relationship between prevalence of multiple sclerosis (MS) and latitude may be due to both genetic and environmental factors. The hypothesis that, in Ireland, MS prevalence is increasing and that north–south differences relate to variation in serum 25-hydroxyvitamin D (25(OH)D) levels was tested in this study.
Patients and methods Patients and matched control subjects were identified in counties Donegal, Wexford and South Dublin through multiple sources. Prevalence was determined. Blood samples were taken for serum 25(OH)D and serum intact parathyroid hormone measurement, and DNA was extracted.
Results Prevalence in 2007 was significantly greater in Donegal (northwest) (290.3/105, 95% CI 262.3 to 321.7) compared with 2001 (184.6/105; 162 to 209.5). In Wexford (southeast), there was a non-significant increase in prevalence in 2007 compared with 2001. Prevalence was significantly higher in Donegal than in Wexford (144.8/105; 126.7 to 167.8, p<0.0001) and South Dublin (127.8/105; 111.3 to 148.2, p<0.0001). Overall, mean 25(OH)D levels were low and did not differ between patients (38.6 nmol/l) and controls (36.4 nmol/l) However, significantly more patients than controls had 25(OH)D levels <25 nmol/l (deficiency) (p=0.004). Levels of 25(OH)D (mean 50.74 nmol/l) were significantly higher in South Dublin (area with lowest prevalence) (p<0.0001) than in Donegal or Wexford. HLA DRB1*15 occurred most frequently in Donegal (greatest MS prevalence) and least frequently in South Dublin.
Conclusion Vitamin D deficiency is common in Ireland. Latitudinal variation in MS probably relates to an interaction between genetic factors and environment (25(OH)D levels), and MS risk may be modified by vitamin D in genetically susceptible individuals.
Statistics from Altmetric.com
Introduction
Numerous studies support the hypothesis that multiple sclerosis (MS) is a multifactorial autoimmune disease arising from a complex interplay between genetic and environmental factors. The HLA-DRB1*1501 allele appears to be the predominant risk allele in northern European populations1 and the HLA DRB1*1501-DQB1*0602 haplotype confers greatest susceptibility to MS in Ireland.2 More recently, linkage to other candidate genes has been demonstrated, including interleukin 2-receptor alpha (IL2-RA), IL7-RA,1 EVI5 (ecotropic viral integration site 5)3 and interferon alpha receptor.4
Many environmental factors have been implicated in the aetiology of MS and may interact with genetic susceptibility. The role of the environment is supported by the distinctive geographical distribution of MS,5–7 with the greatest incidences recorded at high latitudes north and south of the equator.8–10 It is proposed that the latitudinal variation in MS prevalence is inversely related to sunshine exposure and associated vitamin D production.3 The hypothesis regarding the environmental contribution of vitamin D is supported by migration studies which demonstrate an association between place of early residence and MS.11 12 Geospatial analysis in North America and continental USA showed a strong negative correlation between MS distribution and ultraviolet B (UV-B) exposure.13 14 During winter at high latitudes, sun exposure does not generate any vitamin D and thus vitamin D insufficiency is common.14 Lower 25-hydroxyvitamin D (25(OH)D) levels during relapses, in addition to blunted parathyroid hormone (PTH) response,15 suggest that activated vitamin D may have immunomodulatory effects and influence disease activity.16 Activated vitamin D inhibits CD4+T cell and myelin basic protein specific IL17 secreting T cell proliferation.17 Clinically, this is supported by seasonal fluctuation in the number of relapses18 and gadolinium enhancing lesions on MRI.19 20
Few studies on the therapeutic effects of vitamin D in relapsing–remitting MS have been performed. There is no international consensus on optimal 25(OH)D levels or recommended daily intake, and the precise timing of vitamin D action, whether a discrete period or ongoing, remains unknown.
Recent reports suggest that MS prevalence is increasing worldwide.3 21 22 The variation in prevalence with latitude was previously demonstrated in Ireland23 which at 53° North lies in a high risk MS zone where there is minimal skin production of vitamin D between late October and late March due to attenuation of UV-B rays. Based on previous Irish studies, we know that genetic factors contribute to MS susceptibility2 but vitamin D may influence risk. We hypothesised that: (1) the latitudinal gradient in MS prevalence persists in Ireland and (2) greater MS prevalence at higher latitudes relates to lower 25(OH)D levels compared with southern areas and (3) serum 25(OH)D is lower in patients with MS than in healthy controls.
Our aims were to (1) compare the prevalence of MS in three areas in Ireland (two rural areas: counties Donegal (northern latitude) and Wexford (southern latitude); and one urban area: southeast Dublin city (intermediate latitude), (2) determine differences in serum 25(OH)D and PTH levels between MS patients in the three regions and between MS patients and healthy control subjects and (3) examine the frequency of HLA DRB1*15 in people with MS in northern and southern counties.
Patients and methods
Patients of Irish nationality with MS in each area (Donegal, latitude 54°8′–55°43′, Wexford latitude 52°20′–52°44′ and South Dublin, latitude 53°17′) were identified from multiple sources. The ascertainment sources included neurologists and MS nurse specialists, general practitioners, hospital physicians, public health nurses, the MS Society, pharmacies, Cheshire homes and respite facilities. Control participants, frequency matched for age and sex, were recruited in each of the three areas. The prevalence date was established as 31 December 2007. Informed consent was obtained from each participant. For patients with MS, their MS subtype was recorded24 and the Expanded Disability Status Scale was calculated.25 The diagnosis of MS was based on the revised McDonald criteria26 and, where necessary, was confirmed by referring to patients' medical notes. Control participants were recruited in each of the three areas and included spouses and relatives of people with MS in addition to unrelated volunteers. Data from the most recent National Census27 were used to calculate prevalence. Blood samples from patients and controls were taken in winter months from December to March for serum 25(OH)D and serum PTH measurement, and for DNA extraction. A questionnaire regarding environmental factors, including past and current vitamin D supplementation and sun exposure, was completed.28 The ethics committee at St Vincent's University Hospital approved the study.
Serum 25(OH)D and serum PTH analysis
Serum 25(OH)D was measured by a competitive radioimmunoassay (Immunodiagnostic Systems Ltd, Boldon, Tyne and Wear, UK). Interassay coefficients of variations were 6.2% and 7.7% at concentrations of 28.8 nmol/l and 105.4 nmol/l, respectively. The intra-assay coefficients of variations were 3.0% and 2.7% at concentrations of 28.9 nmol/l and 73.9 nmol/l, respectively. Serum 25(OH)D levels of <50 nmol/l were considered to be vitamin D insufficient and levels below 25 nmol/l were considered to be deficient.29 30 Serum intact PTH was measured by electrochemiluminescent immunoassay on the Elecsys 1010 platform (Roche Diagnostics, Basel, Switzerland). Intra-assay CV was <5.8% and interassay CV was <7.1%.
HLA typing
Genomic DNA was isolated from EDTA anticoagulated peripheral blood samples using the GenoM-6 (Genovision, Vienna, Austria) DNA isolation and purification system. Low resolution HLA-DRB1/3/4/5 typing was performed using the PCR sequence specific oligonucleotide probe assay (Invitrogen Dynal Biotech, Bromborough, UK). HLA types were determined using Dynal RELI-SCAN and RELI SSO PMP software.
Statistical analysis
SAS V.9 (SAS Institute Inc) was used. The Z test compared rates of MS in two areas, and the χ2 test was used for comparison of rates in the three areas. Win PEPI31 was used for comparison of rates. For comparison of means and proportions, the Student's t test, analysis of variance and χ2 test were employed, and Pearson's correlation coefficient was calculated for correlation. Age standardised rates were calculated using direct standardisation, with the national population from the most recent census as the standard population.27 For all estimates, 95% CIs were calculated.
Results
Prevalence
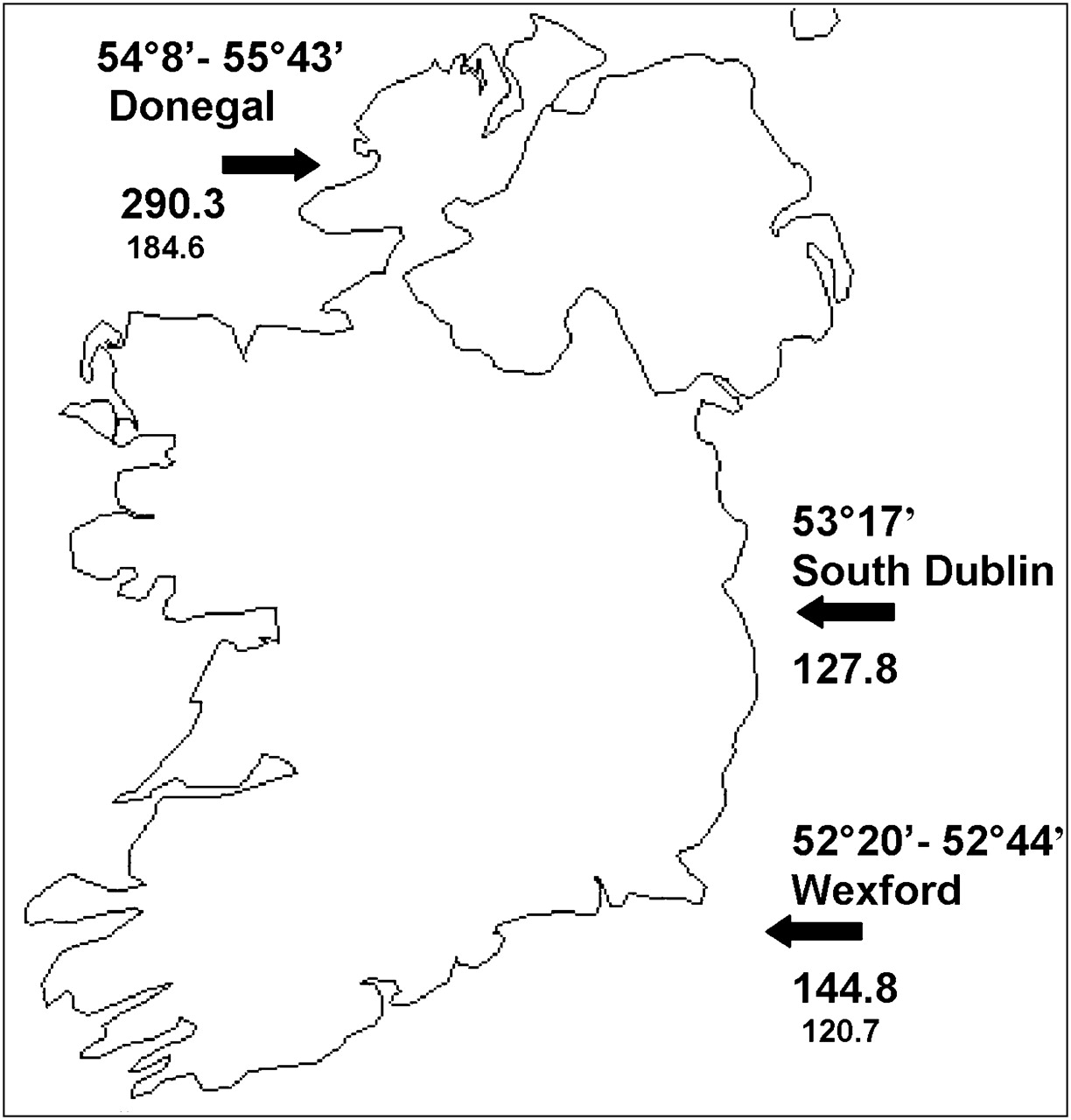
In total, 632 MS patients were identified in the three regions: 329 in Donegal, 173 in Wexford and 130 in South Dublin (table 1). MS prevalence on 31 December 2007 was: Donegal 290.3/105 (95% CI 238.7 to 255.5), Wexford 144.8/105 (95% CI 138.3 to 151.9) and southeast Dublin 127.8/105 (95% CI 131.6 to 146.7). Prevalence was significantly higher in Donegal than in Wexford (p <0.0001) (see figure 1). Although the prevalence in Wexford was higher than that in South Dublin, this did not reach significance (p=0.72).
Demographic data of multiple sclerosis patients ascertained in each region of Ireland on 31 December 2007
{kind=link}
Map of Ireland demonstrating the three areas studied and their latitudes: Donegal county, South Dublin and Wexford county. Prevalence rate is the figure stated per 100 000 population. The figure in small print below the prevalence rate is the prevalence rate in 2001.23 There were no previous prevalence data for the South Dublin area.
Age standardised MS prevalence was: Donegal—all MS patients 257.8/105 (95% CI 253.2 to 262.4), male MS patients 157.6/105 (95% CI 152.7 to 162.6) and female MS patients 358.3/105 (95% CI 350.3 to 366.5); Wexford—all MS patients 152.0/105 (95% CI 148.4 to 155.6), male MS patients 119.0/105 (95% CI 114.8 to 123.4) and female MS patients 176.0/105 (95% CI 170.4 to 181.7); southeast Dublin—all MS patients 123.2/105 (95% CI 120.0 to 126.4), male MS patients 84.2/105 (95% CI 80.6 to 87.9) and female MS patients 160.6/105 (95% CI 155.2 to 166.1). The three counties were significantly different from each other when comparing age standardised prevalence in all MS patients (p<0.001), in males with MS (p<0.001) and in females with MS (p<0.001).
In Donegal, MS prevalence had increased significantly since 2001; prevalence was 184.6/105 in 2001 (95% CI 162.0 to 209.5) and 290.3/105 in 2007 (95% CI 238.7 to 255.5) (p=0.001). There was a non-significant increase in prevalence in Wexford; prevalence was 120.7/105 in 2001 (95% CI 100.6 to 143.8) and 144.8/105 in 2007 (95% CI 138.3 to 151.9) (p=0.117). Prevalence was lowest in southeast Dublin (130.0/105 in 2007) but we did not have previous data for comparison (table 2). We could not compare age standardised prevalence rates over time because these data were not included in the 2001 prevalence study.
Population and multiple sclerosis prevalence data in Donegal, Wexford and South Dublin in 2001 and 2007
Overall, the female to male ratio in MS patients was 2.0:1. In Wexford, the ratio was 1.5:1 (2.2 in 2001), in Donegal 2.1:1 (2.48 in 2001) and in southeast Dublin 2.6:1 (no earlier data).
25(OH)D and PTH levels
Levels of 25(OH)D and PTH were determined in 329 MS patients (61.3% of all ascertained patients) and 226 healthy control subjects (table 3).
Winter serum 25-hydroxyvitamin D levels, winter serum parathyroid hormone levels and HLA-DRB1*1501 frequency in multiple sclerosis patients and control subjects
The mean level of serum 25(OH) D was similar in MS patients (38.6 (SD 22.5) nmol/l) and controls (36.4 (SD 16.4) nmol/l; p >0.05)). Mean 25(OH)D levels in patients in Donegal were 36.9 nmol/l (range 13–97), in Wexford 39.7 nmol/l (15–114) and in southeast Dublin 50.7 nmol/l (13–161). Mean levels were significantly higher in southeast Dublin, the area with the lowest MS prevalence, than in Donegal (p<0.0001) and Wexford (p<0.0001).
There was no significant difference between mean 25(OH)D levels in patients in Donegal and Wexford (Donegal 36.9 nmol/l and Wexford 39.7 nmol/l; p=0.284). The proportion of MS patients from all three study areas with vitamin D deficiency (<25 nmol/l) (28.3%) was significantly higher than the proportion of control subjects (19.2%) (p=0.004).
There was a significant inverse correlation between 25(OH)D and PTH levels in MS patients (r=−0.17; p<0.002) and in controls (r=−0.24; p<0.0003). Vitamin D deficiency (<25 nmol/l) was observed in 93 patients (28.3%) with a mean of 20.3 nmol/l (range 13.3–24.6) and a mean PTH of 44.8 ng/l (range 16.7–86.3). There was a non-significant inverse correlation between 25(OH)D and PTH in this group of patients (p=0.28). Vitamin D deficiency (<25 nmol/l) was observed in 44 control subjects (19.2%) with a mean of 20.8 nmol/l (range 14.3–24.6) and a mean PTH of 48.3 ng/l (range 5.0–131.5). A significant inverse correlation between 25(OH)D and PTH in control subjects with 25(OH)D <25 nmol/l (r=−0.47; p=0.0013) indicated a normal response to vitamin D deficiency.
Overall, significantly more patients (18.2%) than controls (11.5%) were taking vitamin D supplementation of >800 IU/day (800–1500 IU/day) (p=0.04) but there was no significant difference in proportions of patients (5.7%) and controls (8.6%) taking vitamin D supplementation of 1300–1500 IU/day (p>0.05). None of the cohort took >1500 IU vitamin D supplementation/day.
We stratified serum 25(OH)D results, looking separately at patients and controls not taking vitamin D supplementation. Mean serum vitamin D level was similar in patients (38.4 nmol/l) and controls (37.7 nmol/l) after stratification (p>0.05). There was no significant difference in mean 25(OH)D levels between patients (41.0 nmol/l) and controls (38.4 nmol/l) who were taking up to 800 IU vitamin D/day (p>0.05). The difference was significant only in those with very low levels (‘deficiency’=≤25 nmol/l), as before, with a greater proportion of MS patients having very low levels (p=0.004).
Mean serum 25(OH)D levels overall (patients and controls) were significantly lower in those taking no supplements or <800 IU vitamin D/day (38.1 nmol/l) than in those taking >800 IU/day (53.1 nmol/l) (p<0.001). Mean serum 25(OH)D were also significantly lower in those taking no supplements or <1000 IU vitamin D/day (39.9 nmol/l) than in those taking 1000–1500 IU/day (47.9 nmol/l) (p=0.03). Vitamin D supplement data are displayed in table 4.
Vitamin D supplement doses taken by multiple sclerosis patients and controls
Although we did not observe significant relationships between serum 25(OH)D levels and age at MS onset (p=0.26) or the presence of relapse in the previous 2 years (p=0.7), our data were underpowered to address questions regarding these factors or to comment on any association between MS risk and season of birth, early sun exposure (2 h or more of daily summer sun exposure in childhood; p=0.21) or vitamin D supplementation (current or up to age 15 years; p=0.76).
Frequency of HLADRB1*15 allele
The HLADRB1*15 allele was present in 62.9% of MS patients compared with 35.2% of control subjects (p<0.01). The frequency was significantly higher in Donegal patients (69%) compared with South Dublin patients (52%) (p<0.04). Homozygosity for the HLADRB1*1501-DQB1*0602 haplotype occurred significantly more frequently in Donegal compared with Wexford (p=0.032).
Discussion
In keeping with recent epidemiological studies of MS,3 21–23 we have observed an increase in the prevalence of MS nationally between 2001 and 2007, with a significant increase in the most northerly region of Donegal. We confirmed the latitudinal gradient found in 2001,23 with a significantly greater MS prevalence in the Northwest compared with the Southeast. This latitudinal gradient has been attributed to genetic factors, based on ancestral differences in each area (Celtic in the Northwest and Anglo-Norman in the Southeast) and the heterogeneity in distribution of HLA class II associations (specifically the HLA DRB1*1501–DQB1*0602 haplotype) in between these areas. The ethnic makeup of the study cohort was relatively homogenous. Although Dublin county has experienced significant migration over the past decade, the particular area studied is not an area of marked migration, and population ethnicity was comparable with both Donegal and Wexford. Increased prevalence may be influenced by numerous factors in addition to increased incidence but our case ascertainment and diagnostic techniques have not changed greatly since the last prevalence study in 2001.23 Incidence could not be calculated due to inability to ascertain year of (MS) onset data in all identified cases. These particular cases were identified from at least two sources but exact timing of MS onset was not clearly recorded and patients declined interview.
Our study hypothesis is based on the idea that serum vitamin D levels in adulthood, after MS has presented, are relevant, or at least reflect what has happened previously, a limitation imposed by the nature of our study. Evidence from monozygotic (MZ) twin studies in MS32 supports the hypothesis that MS is strongly influenced by environmental factors in genetically susceptible individuals, that vitamin D levels are genetically regulated and that MS itself is not the cause of low vitamin D (eg, limited sun exposure imposed by indoor lifestyle). Adoptee33 step sibling34 and half sibling studies35 indicate that the environmental component is ubiquitous, rather than limited to the shared family environment. However, the exact timing of vitamin D action, and whether adult levels reflect those in the past, is as yet unknown. Chronic low concentrations, seasonal fluctuation or acute effects may all increase risk, and this limits our ability to draw clear conclusions. Insufficient pre- and perinatal vitamin D levels may imprint on functional characteristics of various tissues, increasing the risk of adult onset MS by interacting with other genetic susceptibility factors36 and adult exposures (including hypovitaminosis D during adult life).
MS displays a month of birth effect, with an excess of patients being born in spring and a deficit in winter; the effect is most pronounced in familial cases,37 implicating interactions between genes and environment related to climate. A recent Scottish study38 showed a marked difference (50%) in MS risk between being born in April versus November, and this month of birth association implicates interaction of a seasonal risk factor with loci at or near HLA-DRB1, the region exerting the single strongest genetic effect in MS, during gestation or shortly after birth.39 Our study was not sufficiently powered to address month of birth. The nature of this timing of birth effect remains unknown but maternal vitamin D deficiency is one plausible candidate.37 40 36
Although MZ twins share a common genotype, epigenetic differences may cause phenotypic discordance (including disease susceptibility). Examination of differences in DNA methylation and histone acetylation in a large cohort of MZ twins41 showed that, although epigenetically indistinguishable during the early years of life, marked differences in content and genomic distribution of 5-methylcytosine DNA and histone acetylation in older twins affected their gene expression portrait. The divergence of epigenetic modification patterns with age may be influenced by intrinsic and extrinsic factors, such as smoking and diet, and epigenetic drift may occur with ageing itself. Fraga et al showed that approximately one-third of twins studied displayed epigenetic differences in DNA methylation and histone modification, distributed throughout their genomes and impacting on gene expression. These markers were more distinct in older twins with different lifestyles, highlighting the role of environmental factors in modifying a common genotype to a different phenotype (eg, discordant MS onset in MZ twins). Environmental modulation of genetic information, by altering the pattern of epigenetic modifications, supports the environment (vitamin D)–genetic interaction findings in our study, and suggests that adult exposures, including vitamin D levels, may play a role in both MS risk and disease modification, even if the critical exposure period began prenatally.
Despite our hypothesis that the prevalence gradient would relate to lower 25(OH)D in MS patients, 25(OH)D levels between the north (Donegal) and south (Wexford) were not significantly different and did not differ from control subjects; winter levels were low in all participants. It is important to remember that optimal levels remain undefined (and may be much higher than current laboratory reference ranges—for example, ≥100 nmol/l).42 Our view of sufficiency is arbitrary, and we cannot assume that all individuals require the same levels. However, mean winter levels in our Irish cohort were low overall (<50 nmol/l) and significantly more MS patients than controls had very low levels (<25 nmol/l). As previously described by others,15 there was a blunted PTH response only in MS patients with vitamin D deficiency (<25 nmol/l) but its meaning is unclear. Only a small percentage took >1000 IU vitamin D3 daily; maximum intake was <1500 IU but it is likely that at least 4000 IU daily are required to achieve levels of 100 nmol/l.43 Despite differences in solar radiation (UV-B) exposure between areas, the northwest of Ireland experiences on average 319 875 joules/cm2 solar radiation annually compared with 331 683 joules/cm2 solar radiation in the southeast44; it is probable that the latitudinal range in a small country such as Ireland is insufficient to demonstrate such an effect. Higher 25(OH)D in southeast Dublin may be genetically regulated or relate to more widespread use of vitamin D supplements (39%) compared with Wexford (24%), and greater availability and consumption of fortified milk in Dublin.45 Differences in socioeconomic group distribution between these areas may influence supplementation practices.27 However, in 52% of patients and 55% of controls taking vitamin D3 supplements, the dose of ≤400 IU/day was unlikely to alter serum levels significantly.
The HLA DRB1*15 allele, associated with MS susceptibility, was significantly overrepresented in MS patients compared with controls, and HLA-DRB1*15 frequency was significantly lower in southeast Dublin compared with areas of higher MS prevalence. Active vitamin D (1, 25-dihydroxyvitamin D) binds the intranuclear vitamin D receptor (VDR) whose gene locates to chromosome 12q13.1. The resulting complex binds the retinoid X receptor (RXR), resulting in a VDR–RXR complex, which then binds the vitamin D response element (VDRE).46 Recently, a VDRE was found on HLA DRB1*1501, the major MS susceptibility allele. Insufficient HLA DRB1*1501 expression—in the setting of low vitamin D and suboptimal binding to the VDRE, with poor upregulation of HLA DRB1*1501—could affect central deletion of autoreactive T cells. Thus people possessing HLA DRB1*1501 may be at high risk of autoimmunity (MS) in the setting of vitamin D deficiency and this combination may explain the high prevalence of MS in the Irish population.
The latitudinal variation in MS in Ireland is not explained by 25(OH)D levels alone but most likely the interaction with genetic susceptibility. In a gene–environment interaction, lacking either component can prevent clinical expression of disease, leaving one factor apparently unrelated to risk when both are required. Therefore, similar overall serum 25(OH)D levels in patients and controls does not outrule the role of low vitamin D in MS pathogenesis in our cohort.
In addition to the previously discussed limitation imposed by the nature of our study (ie, hypothesis based on the idea that serum vitamin D levels in adulthood are relevant in MS), we acknowledge that inclusion of spouses as controls is not always ideal, as they are usually in the same environment as affected cases and may modify their risk by taking vitamin D supplements more readily. However, we found that significantly more patients (18.2%) than controls (11.5%) were taking vitamin D supplements (≥800 IU) (p=0.04), despite this potential spousal influence. Spousal controls were included because they were more willing to give samples than people without affected family or partners.
In conclusion, although unproven, one might hypothesise that combined high frequency of HLADRB1*15 and widespread vitamin D insufficiency may explain the high, increasing MS prevalence in the Irish population. Vitamin D may only be one factor in a common mechanism by which environment interacts but it is a potentially modifiable risk. Vitamin D insufficiency is common throughout the population, an important public health observation. The MS prevalence gradient in Ireland is not explained by variation in 25(OH)D levels alone but differences in the frequency of the MS risk allele HLADRB1*1501 and risk haplotype HLADRB1*1501-DQB1*0602 combined with low serum vitamin D levels probably influence latitudinal variation.
Acknowledgments
The authors would like to thank sincerely the consultant neurologists Dr R Murphy and Dr D McCabe at AMNCH, Tallaght, Dr J Redmond and Dr C Doherty at St James' Hospital, Professor O Hardiman, Dr N Delanty and Dr J Moroney at Beaumont Hospital, Professors T Lynch and P Kelly at the Mater Misericordiae hospital in Dublin, Dr K Murphy at Sligo General Hospital and Dr Peter Boers at the Western Regional Hospital, Limerick, Dr P Crowley at Waterford Regional Hospital, Dr D Costigan, Dr H Galvin and also the general practitioners in each region, for granting access to data of MS patients in our study areas. We would also like to thank Dr Bannan, Consultant Physician at Letterkenny Hospital and Dr Quigley Consultant Physician at Wexford General Hospital, who allowed us to use their clinic rooms for weekend research clinics. We are also grateful to MS Ireland for much help during the study, and for ongoing support. We also thank the patients with MS and the control volunteers who agreed to participate in this study.
References
Supplementary materials
Lay Summary 82/3/317
Files in this Data Supplement:
Footnotes
See Editorial Commentary, p 237
Linked article 234237.
Funding MS Ireland contributed funds towards the study.
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of St Vincent's University Hospital, Dublin, Ireland.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary