Article Text

Abstract
Background Exogenous sexual steroids together with pregnancy have been shown to influence the risk of relapses in multiple sclerosis (MS). Treatments used during assisted reproductive techniques may consequently influence the short term evolution of MS by modifying the hormonal status of the patient. The objective of this study was to determine if there was an increased risk of developing exacerbations in women with MS after in vitro fertilisation (IVF).
Methods MS and IVF data were either automatically extracted from 13 French university hospital databases or obtained from referring neurologists. After matching databases, patient clinical files were systematically reviewed to collect information about MS and the treatments used for IVF. The association between IVF and the occurrence of MS relapses was analysed in detail using univariate and multivariate statistical tests.
Findings During the 11 year study period, 32 women with MS had undergone 70 IVF treatments, 48 using gonadotrophin releasing hormone (GnRH) agonists and 19 using GnRH antagonists. A significant increase in the annualised relapse rate (ARR) was observed during the 3 month period following IVF (mean ARR 1.60, median ARR 0) compared with the same period just before IVF (mean ARR 0.80, median ARR 0) and to a control period 1 year before IVF (mean ARR 0.68, median ARR 0). The significant increase in relapses was associated with the use of GnRH agonists (Wilcoxon paired test, p=0.025) as well as IVF failure (Wilcoxon paired test, p=0.019).
Interpretation An increased relapse rate was observed in this study after IVF in patients with MS and may be partly related both to IVF failure and the use of GnRH agonists.
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is an autoimmune disease characterised by a female to male ratio of 3:1.1 ,2 To date, the mechanisms underlying this female preponderance are not fully known. Sex hormones might play a major role in this setting, given their interactions with the immune system.3 Clinical observations support the influence of sex hormones in MS. The predominant female to male ratio of the disease seems to be closely linked to the occurrence of puberty.4 A large prospective study reported a correlation between hormonal status and the risk of MS relapse after pregnancy and delivery.5 ,6 A recent study showed that oral contraceptives could be associated with a short term reduction in the risk of MS.7 Treatment with the pregnancy hormone oestriol led to a significant decrease in the radiological activity of patients with MS.8
Infertility has not been shown to be increased in women with MS. However, a lower birth rate was reported9 and patients may be willing to use assisted reproductive techniques in the case of conception difficulties. Given the effect of sexual hormones on disease activity, one may hypothesise that manipulation of hormones could affect at least the short term course of the disease. In a previous case series, we reported an increased relapse rate after in vitro fertilisation (IVF) in six patients with MS.10 As they were mostly treated with gonadotrophin releasing hormone (GnRH) agonists, we challenged the role of this treatment in the observed increased relapse rate. Other case reports have also suggested an increased rate of relapses after IVF or ovarian stimulations.11 ,12 However, a larger systematic study to confirm these preliminary results and to investigate the influence of IVF treatments on MS relapses is still lacking.
We conducted a larger and systematic epidemiological study to investigate the influence of IVF treatments on the risk of relapse in women with MS.
Material and methods
Source data
In France, the reasons for a patient's hospitalisation are systematically recorded in a local database called PMSI (Programme de Médicalisation des Systèmes d'Information), using a universal disease classification provided by the WHO.
Thirteen French university public hospitals participated in the study. Lists of patients admitted between 1 January 1998 and 31 December 2008 with a diagnosis of MS or IVF were automatically extracted from these databases. The authorisations were obtained from the departments of medical information housing the data, as well as the National Commission for free access to computerised data (CNIL, Commission Nationale Informatique et Libertés, accession No 906245).
Data collection
The departments of medical information provided a list of partly anonymised data for a total of 9768 MS patients and 27 895 IVF procedures. After matching these two lists, 21 patients with both diagnoses were identified. The whole medical record of these patients was reviewed (by LM, MJF and FL). The collected data contained information on demographics, medical history, MS (clinical course, dates of relapses, symptoms and signs at the time of relapses, relapse, immunoactive treatments) and IVF (date, type of protocol used, outcome of IVF).
A relapse of MS was defined using standard criteria.13 ,14
Each IVF procedure involves an initial step of ovarian desensitisation with either GnRH agonists or antagonists, followed by ovarian stimulation with FSH.
Considering the small number of cases, we additionally put together a group of 14 MS patients that were recruited following referral by their neurologists who were aware of the study. These women were not identified by the department of medical information because they were followed in private hospitals for the IVF procedures. The whole medical record of these patients was reviewed (by LM, MJF and FL). To avoid potential recruitment (recall) bias in this latter group, the two groups were compared in terms of their demographic and clinical parameters. Given that no differences were observed, the two groups were pooled to increase the power for further analysis. Hence all multivariate results were adjusted on the recruitment procedure to take into account this potential recall bias.
Patients
Inclusion criteria
Patients had to have a diagnosis of MS according to the McDonald 2005 revised criteria.15 All types of clinical courses were included in the study. They also had to have undergone at least one IVF treatment during the study period (1998–2008) and after MS onset.
Exclusion criteria
To have the most homogeneous cohort, patients who had been treated only by ovarian stimulation or intrauterine insemination were excluded from the analysis.
Outcomes and statistical analyses
As explained in detail by the European Medicine Agency in the guidelines on clinical trials in small populations,16 simple statistical methods may often be adequate when a large amount of data is available, but when very few data exist, it is imperative that the most efficient and informative analytical methods be used. These methods involve assumptions that may not be testable. Hence sensitivity analyses consisting of various models should be presented. In accordance with these guidelines, we performed three different statistical methods (Wilcoxon paired tests, mixed Poisson regression analysis and frailty model). More precisely, two outcomes were analysed to evaluate the association between IVF and relapses.
The difference between the number of relapses before and after the IVF procedure regarding two similar time intervals. We performed two different analyses to evaluate this outcome. First, a non-parametric and non-adjusted analysis using the Wilcoxon test for paired data. The interest in this method is that it is reliable for small sample sizes. The main judgement criterion was the comparison of the Annualised Relapse Rate (ARR) over a period of 3 months before and immediately after IVF and in a control period 1 year before IVF. The control period began 1 year before IVF and had the same duration as the period tested (3 months for the main criterion of judgement). A control period was used because one may hypothesise that the IVF procedure was performed during a low risk period of relapse and that consequently, the following periods are of higher risk. A sensitivity analysis was also performed, comparing the ARR for other lengths of time (2 and 6 months) immediately before and after IVF and on a similar control period 1 year before IVF. The Wilcoxon test was used because it is reliable when comparing small cohorts, as in our study. The drawback is that it does not take into account the fact that a patient may have undergone several IVFs, which probably impacts on type I or type II errors. This is the reason why we also performed multivariate analyses to compare the ARR before and after IVF using a mixed Poisson regression analysis with three adjusting variables: age at IVF, disease duration at IVF and type of recruitment. Random effects were used to take into account repetition of observations. The analyses were also stratified according to the outcome of IVF, as pregnancy is known to lead to a significant decrease in relapse rate. The same analyses were performed to study the type of fertility treatment used for IVF in each subgroup, defined by the treatment protocol (GnRH agonists or GnRH antagonists). Using this method, the hierarchy of the data is taken into account and the possible confounding factors are taken into account without subgroup analysis. Nevertheless, the major flaw is that the model is parametric and requires assumptions not evaluable on small samples.
The association between IVF and the time between two relapses. We performed a multivariate model using a frailty Cox regression, with IVF taken into account as a time dependent covariate. For that purpose, all time intervals between two relapses were calculated for the whole cohort of patients, from the beginning of their MS to the last date recorded in the medical file. The association between IVF and the time between two relapses was assessed by a multivariate frailty model. This model takes into account the censored measures of relapses, recurrence of relapses for a given patient and the time dependence of the variables. All variables (IVF procedure, type of IVF protocol, outcome of IVF, type of recruitment) were analysed separately but always adjusted for the patient's age at the last relapse before IVF, disease duration at the last relapse before IVF and recruitment procedure. The assumption of hazard proportionality was evaluated according to the weighted residuals.17 ,18 The major flaw of this method is that it would need a large amount of data to be efficient, which is not the case in this study.
R software, V.2.9.2, was used for all multivariate analyses and Prism software V.4 was used for the Wilcoxon paired test. Results were considered significant when p<0.05.
Results
Patient characteristics
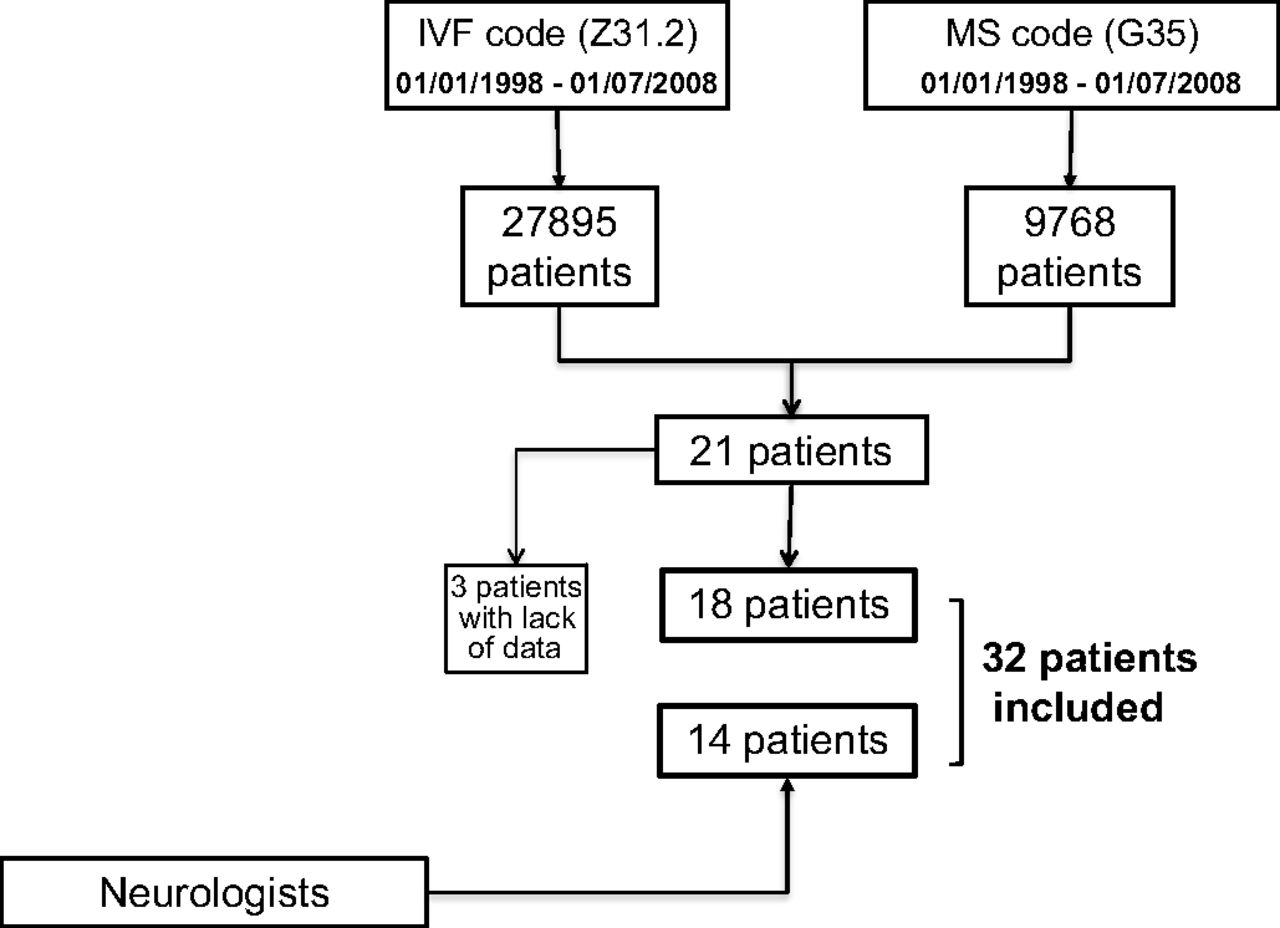
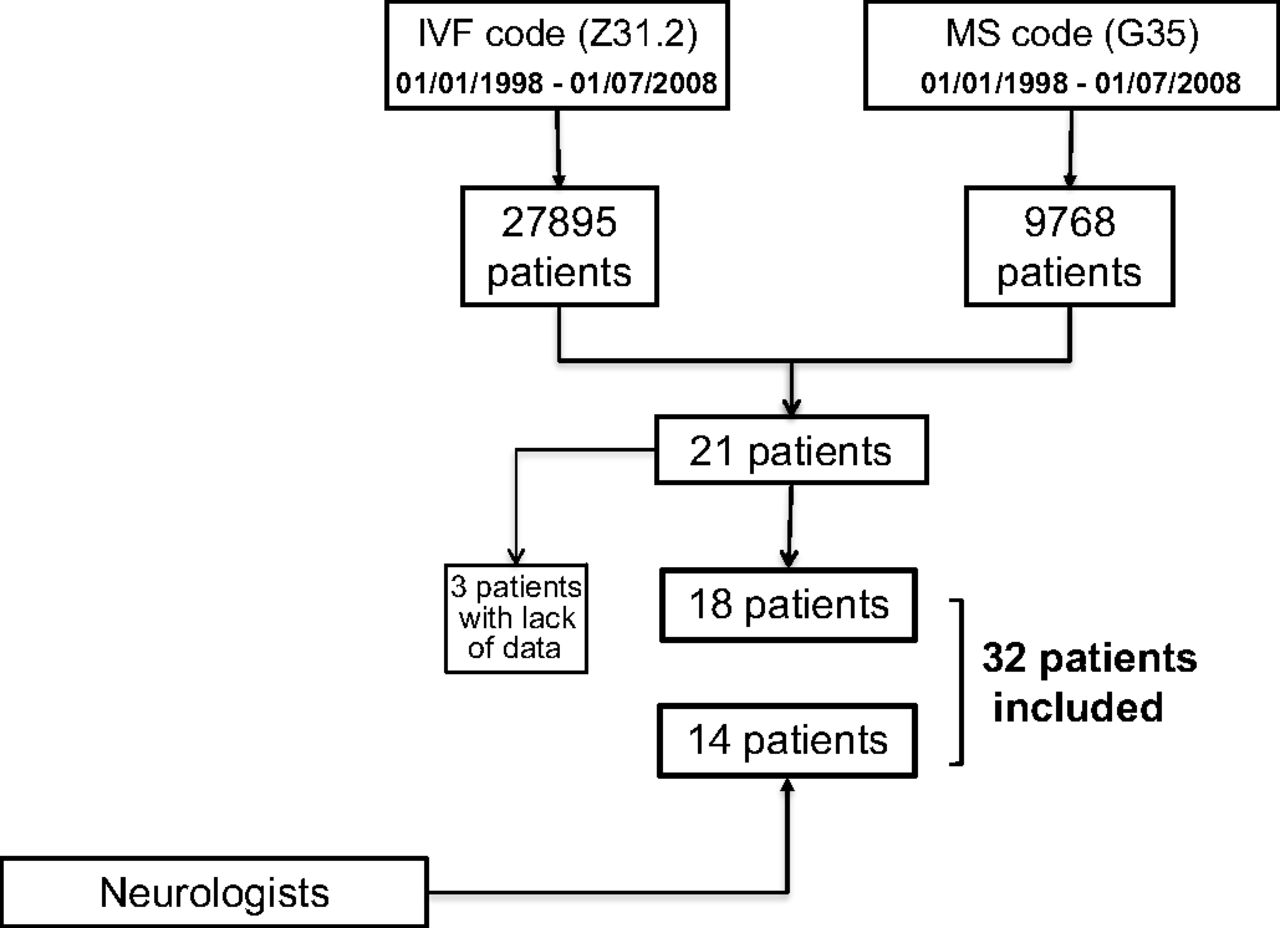
After matching the two lists of patients provided by the departments of medical information of 13 French university hospitals, 21 patients were identified with both a diagnosis of MS and IVF, but three were excluded from the analysis because we did not have access to their medical records (figure 1). Fourteen additional patients were recruited after spontaneous referral by their consultant neurologists. The clinical and demographic characteristics of all patients are presented in table 1. Because no significant difference was observed between these two groups of patients, they were pooled for further analyses. Moreover, the possibility of selection bias as a confounding factor was taken into account in the multivariate analyses.
{kind=link}
Recruitment of the 32 patients. In the 13 participating French university hospitals, a list of 9768 multiple sclerosis (MS) patients (from 1998 to 2008) was obtained. In the same way, a list of 27 895 patient names was obtained corresponding to patients treated with in vitro fertilisation (IVF) procedures in the same university centres at the same time. By matching these two lists, 21 patients were found and three patients were excluded because we did not have access to their medical records. Fourteen more patients were recruited by referral, thanks to neurologists aware of the study.
Comparison of different demographic and disease related parameters between the two groups of patients
Multiple sclerosis characteristics
Mean age at onset of MS in the 32 patients was 26.3±4.8 years. At the time of the first IVF, mean duration of MS was 6.6±4.7 years; 27 patients had a relapsing–remitting form of MS, four patients had a secondary progressive form of MS with relapses and one patient had a progressive–relapsing form of MS. Mean duration of follow-up after IVF was 6.6±4.7 years. Eighteen patients had never received any immunomodulatory or immunosuppressive drugs before their first IVF. At the time of their first IVF, four patients had continued on immunoactive treatment (glatiramer acetate in two patients, interferon β in one and azathioprine in one) while the other 10 patients had stopped their treatment 19±5.0 months before. The time intervals between stopping therapies for MS and IVF ranged from 1 to 31 months. However, only two patients stopped their treatment in the year before IVF, and among the two patients, one was treated for only 2 months. The other patient was treated with interferon and stopped 6 months before IVF.
In vitro fertilisation characteristics
The aetiologies of infertility were diverse, with eight cases of male origin, five of female origin, eight of mixed origin and six of unknown origin. This information was lacking for the other five patients. Seventy IVF procedures were performed in 32 patients, with a mean of 2.1±1.2 IVF procedures per patient. Thirty-two procedures were simple IVF whereas 35 were intracytoplasmic sperm injection. For one patient (corresponding to four IVF procedures), these data were not found. Treatments used for ovarian desensitisation consisted of either GnRH agonists (18 patients, 48 cases) or GnRH antagonists (14 patients, 19 cases). For three IVF procedures, the type of drug used could not be retrieved. Twenty-one pregnancies were obtained with 18 births and three spontaneous miscarriages during the first trimester.
Increased relapse rate after IVF
In our cohort of patients, 19 women suffered a relapse during the 3 months following IVF and 26 relapses were noted in the 3 month period following the 70 IVF procedures. When a relapse was treated (62%), it was always using corticosteroids at high doses by the intravenous route. However, these data were missing for two patients. In the 3 month period following IVF, the ARR significantly increased to 1.60±2.40 (median ARR 0, range 0–8) compared with both the 3 month period before IVF (mean ARR 0.80±1.61; median ARR 0, range 0–4; p=0.011, Wilcoxon paired test) and the control period 1 year before (mean ARR 0.68±1.51; median ARR 0, range 0–4; p=0.035, Wilcoxon paired tests) (table 2). These results were confirmed by a multivariate Poisson regression analysis (tables 3 and 4). When taking into account only the first IVF for the 32 patients, the same results were noted. Indeed, in the 3 month period following the first IVF, the mean ARR was 2.06 (median ARR 0) and was significantly increased compared with the 3 month period preceding IVF (mean ARR 0.62, median ARR 0; p=0.008, Wilcoxon test) and with the control period (mean ARR 0.55, median ARR 0, p=0.008, Wilcoxon test).
Comparisons of the annualised relapse rates in the 3 month period before IVF, after IVF and during a control period 1 year before IVF, in several groups of patients
Differences between the number of relapses during the 3 month period before and after IVF
Differences between the number of relapses during the 3 month period after IVF and a control period 1 year before IVF
For patients who had a relapse in the 3 months following IVF, the mean time between IVF and the first post-IVF relapse was 42.2±28.3 days while the median time was 45 days (range 7–90 days).
When shortening the period of interest to 2 months, the post-IVF ARR similarly increased to 1.71±3.09 (median ARR 0, range 0–12) compared with 0.77±2.02 (median ARR 0, range 0–6) in the 2 months preceding IVF and 0.74±1.99 (median ARR 0, range 0–6) in the control period (p=0.022 and p=0.062, respectively, Wilcoxon paired tests; see supplementary table 1, available online only). The same significant results were obtained when using the multivariate Poisson regression analysis (see supplementary tables 2A and 2B, available online only).
When increasing the study period to 6 months, there was a persistent increase in the ARR observed after IVF (mean ARR 1.15±1.48; median ARR 0, range 0–4) compared with 0.8±1.61 (median ARR 0, range 0–4) and 0.92±1.06 (median ARR 0, range 0–4) during the pre-IVF and the control periods, respectively, but the difference was no longer significant (p=0.126 and p=0.556, respectively, Wilcoxon paired tests; supplementary table 1, available online only) and confirmed by multivariate Poisson regression analysis (supplementary tables 3A and 3B, available online only).
However, using multivariate frailty model analysis, while an increased risk of relapse was still observed after IVF, this increased risk was no longer significant (RR=1.18, 95% CI 0.78 to 1.45, p=0.43) (table 5).
Analysis of the relationship between each covariate (IVF, success or failure of the IVF, type of protocol) and the time between the relapses, in a frailty model
Influence of IVF outcome on relapse rate
We performed the same analyses after stratification based on IVF outcome. Among 70 IVF procedures in 32 patients, 49 had failed while 21 resulted in pregnancy.
In cases of IVF failure, the ARR in the 3 month post-IVF period significantly increased to 1.96±2 (median ARR 0, range 0–8) compared with the pre-IVF period (mean ARR before IVF 0.98±1.74, median ARR 0, range 0–4, p=0.019). There was only a tendency on comparison with the control period (mean ARR in the control period 0.82±1.63, median ARR 0, range 0–4, p=0.076, Wilcoxon paired tests, table 2). Similarly, a significant difference was observed for the 2 month periods (supplementary table 1, available online only). For the 6 month periods, an increased number of relapses was also observed after IVF but the differences from the pre-IVF and the control periods were not significant (supplementary table 1, available online only). Additionally, when comparing the risk of relapse during the 3 month period following IVF in the ‘success of IVF’ versus ‘failure of IVF’ groups, a tendency for an increased risk of relapse was observed in the group ‘failure of IVF’ (mean 1.96 vs 0.76, p=0.06, Mann–Whitney test). Using the multivariate frailty model, the increased number of relapses in cases of IVF failure was confirmed, with an RR of 1.67 (95% CI 1.06 to 2.63, p=0.026, table 5).
In the 21 cases in which IVF led to pregnancy, the ARR increased in the post-IVF period regardless of its length (2, 3 or 6 months) but this increase was not significant. For the 3 month period, ARR after IVF was 0.76±1.61 (median ARR 0, range 0–4) compared with 0.38±1.20 (median ARR 0, range 0–4) before IVF and with 0.38±1.20 (median ARR 0, range 0–4) in the control period (p=0.375 and p=0.562, respectively, table 2). When the three miscarriages were excluded from the analysis, the same results were obtained (data not shown).
Influence of drug type on relapse rate
Forty-eight IVF procedures were performed using GnRH agonists and 19 with GnRH antagonists. Data were missing for three procedures. The pregnancy rate was lower in the group treated with GnRH antagonists (10%, two pregnancies) compared with those treated with GnRH agonists (40%, 19 pregnancies). A significant increase in ARR was observed in the 3 month period following IVF in the group of patients treated with GnRH agonists, with a mean ARR of 1.60±2.29 (median ARR 0, range 0–8) compared with 0.75±1.58 (median ARR 0, range 0–4) in the 3 months preceding IVF (p=0.025, Wilcoxon paired test) and 0.6±1.47 (median ARR 0, range 0–4) in the 3 month control period (p=0.025, Wilcoxon paired test, table 2). The same observation was made for the 2 month period (supplementary table 1, available online only). For the 6 month period, this significant difference disappeared (supplementary table 1, available online only). Using the multivariate frailty model, an increased relative risk after IVF using GnRH agonists was observed but without reaching significance (RR=1.35, 95% CI 0.83 to 2.18, p=0.22, table 5).
In contrast, IVF performed with GnRH antagonists did not lead to a significant difference in ARR, regardless of study period length (table 2 and supplementary table 1, available online only). This lack of association was confirmed in the multivariate analysis based on the frailty model (RR =0.73, 95% CI 0.35 to 1.53, p=0.409, table 5).
Discussion
Our paper presents the first systematic study of the relationship between IVF and risk of subsequent relapse in MS. We found a significant increase in the relapse rate after IVF, especially in patients for whom IVF had failed. Further, the influence of GnRH agonists was also tested, showing a positive correlation in some statistical tests. To avoid any selection bias, we intended to include patients in a systematic way, by matching databases from 13 French university hospitals for a common diagnosis of MS and IVF, between 1998 and 2008. However, because such patients were very rare, we also included a cohort of patients spontaneously referred by their treating neurologists. As there was no difference between the two groups, we pooled the data, enabling the study of 32 patients. Further, we adjusted all of the results obtained by multivariate models for this possible confounding factor. We tested various statistical models to ensure the robustness of the results, following the recommendations of the European Medicines Agency for therapeutic trials in small cohorts. To our knowledge and to date, this is the largest cohort analysis of the short term relationship between IVF and the risk of relapse in MS patients.
IVF was previously reported to worsen the relapse rate in MS in three smaller case series. Our own team was the first to describe a significant increase in relapses in six MS patients following IVF,10 and later Hellwig et al confirmed this observation in a larger cohort of 23 patients.11 ,12 However, in these latter studies, patient recruitment was based either on adverts or on neurologists/gynaecologists aware of the study. This mode of recruitment might have favoured the inclusion of patients with relapses after IVF procedures by a recall bias. Additionally, patients were asked to answer a questionnaire to provide the number and dates of MS relapses, which again could have introduced recall biases. In our study, the medical records of the patients included were systematically reviewed to avoid any memory bias.
In our cohort analysis, we observed an increased relapse rate after IVF during all periods tested (2, 3 and 6 months) but without reaching significance for the 6 month period. Thus it is difficult to conclude whether IVF may provoke additional relapse or only shorten the delay between IVF and the following relapse. The increase in the relapse rate is probably multifactorial and we observed a significant increase in patients for whom the IVF procedures failed. Failure of IVF led to a decrease in sex hormones that might be similar to that observed in the postpartum period where an increased relapse rate has been demonstrated,5 thus providing a plausible explanation for the results observed in our multivariate analysis. This hypothesis is also strengthened by the observed difference in terms of risk of relapse between the groups ‘failure of IVF’ and ‘success of IVF’ in our cohort of patients.
Another factor that may play a role in the increased relapse rate is the stress induced by such a procedure, as hypothesised by Hellwig et al.12 While the role of stressful life events is still debated as a triggering factor for MS relapses, several studies have shown an increased exacerbation rate under stress in MS patients.19 ,20
Another explanation for the particular increase in the risk of relapse following IVF may come from the drugs used for ovarian desensitisation. Indeed, we found a relationship between the use of GnRH agonists and the increased relapse rate, at least with a univariate statistical approach. Using the multivariate frailty model, the link was no longer significant but it has to be kept in mind that these statistical approaches would need large amounts of data to be powerful. Several studies have shown that GnRH agonists can have a direct effect on the proliferation of B and T cells, trigger gene transcription, adhesion, chemotaxis and homing to specific organs.21–25 Furthermore, Jacobson et al demonstrated in lupus prone mice that GnRH administration led to disease exacerbation whereas GnRH antagonists significantly improved survival.24 Finally, GnRH may directly stimulate the immune system and this may partly explain the increased risk of relapse observed in this study in patients treated with GnRH agonists. Moreover, the protocols using GnRH agonists are very different than those using antagonists in terms of duration and adverse events (higher dosages of gonadotrophins used, higher incidence of hyperstimulation syndrome, longer duration of treatment and more aggressive protocol compared with antagonists).26 All of these points may possibly influence the rate of relapse after IVF. Another interesting point comes from the fact that GnRH antagonists are associated with a lower birth rate that appears to increase the risk of relapse. Then, these two factors appear to be opposite and may provide an underestimation of the risk of relapse after failure of IVF or of the decreased risk of relapse after using GnRH antagonists in our study.
Despite the direct conclusions that might be made by our study and that would impact on patient counselling in daily practice, limitations to our results have to be discussed. The cohort was small and it is difficult to draw definitive conclusions based only on 32 patients. Obviously, a prospective study would be of interest but the rarity of IVF procedures in MS patients would make such a study highly difficult to perform. Potential memory bias may come from the pooling of two different cohorts, one of them based on neurologists who might have selected unintentionally the more active diseases. Indeed, comparison of the ARR after IVF in the two different cohorts is different, while not reaching statistical significance. Because it may have an impact on our results, particularly on the Wilcoxon tests we used, we also performed multivariate analyses which took into account this possibility. Using these multivariate analyses we were able to see a significant increase in the ARR after IVF, particularly in patients with IVF failure, suggesting that this observed increase is not due to an imbalance between the two groups of patients. We also noticed that the ARR before IVF was higher in the IVF failure group than in the IVF success group. The reason for this difference is not clear but we can hypothesise that patients suffering from a more severe disease are more prone to IVF failure for several external reasons (such as the treatment of the relapses or the stress induced by the relapses). Finally, another limitation in the interpretation of the data may come from the absence of a control group. We made the choice of studying several periods of time in the same cohort of patients rather than studying another cohort as a control group in order to decrease the interindividual variability.
However, despite these limitations, MS patients should be aware of a possible increased risk of MS relapse after IVF, particularly if the procedure does not result in a pregnancy. Furthermore, because there is a reasonable doubt that GnRH agonists may make patients more prone to such an increase in relapse rate, GnRH antagonists might be preferred for IVF protocols.
Acknowledgments
The authors thank Professor Ph Damier for reviewing and corrections, and Britt House for English language editing.
Appendix
The patients included in the study came from the following centres:
Nantes (seven patients): S Wiertlewski, DA Laplaud; Clermont-Ferrand (five patients): P Clavelou; Lyon (four patients): F Durand-Dubief, C Confavreux, S Vukusic; Strasbourg (four patients): J de Sèze; Marseille (three patients): J Pelletier, A Ali Cherif; Nice (three patients): C Lebrun-Frenay; Bordeaux (three patients): JC Ouallet, B Brochet; Toulouse (two patients): D Brassat, M Clanet; Rennes (one patient): E Le Page, G Edan.
However, we also obtained lists of MS patients and IVF patients from the following centres. Unfortunately, no positive matching was found between the two lists: F Dubas (Angers), G Defer (Caen), P Labauge (Nîmes), L Magy (Limoges) and J-M. Vallat (Limoges).
In addition to the authors, participants in the study were as follows:
Neurologists: O Godefroy (Amiens), L Rumbach (Besançon), G Defer (Caen), T Moreau (Dijon), P Vermersch (Lille), J Touchon (Montpellier), M Debouverie (Nancy), O Heinzleff (Poissy), R Gil (Poitiers), S Bakchine (Reims), B Mihout (Rouen), O Lyon-Caen (Paris), E Roullet (Paris).
Departments of medical information: P Six (Angers), R Salamon (Bordeaux), MJ D'Alche-Gautier (Caen), B Aublet-Cuvelier (Clermont-Ferrand), E Benzenine (Dijon), A Vergnenegre (Limoges), S Couray-Targe (Lyon), M Fieschi (Marseille), R Sambuc (Marseille), T Boudemaghe (Nîmes), Roeslin (Strasbourg), F Boutault (Toulouse), D Petiot (Toulouse), MC Turnin (Toulouse).
Gynaecologists and medically assisted procreation departments: M Boudineau (Nantes), P Descamps (Angers), N Commenges (Bordeaux), C Hocke (Bordeaux), I Parneix (Bruges), M Herlicoviez (Caen), JL Pouly (Clermont-Ferrand), P Sagot (Dijon), D Dewailly (Lille) C Decanter (Lille), P Piver (Limoges), B Sale (Lyon), M Gamerre (Marseille), L Cravello (Marseille), P Mares (Nîmes), B Pfister (Nîmes), S Viville (Strasbourg), J Ohl (Strasbourg), J Parinaud (Toulouse), F Lesourd (Toulouse).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
Funding This work was supported by a grant from the PHRC Inter-régional 2005 (French Ministry of Health).
Competing interest None.
Ethics approval Ethics approval was provided by the National Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.