Article Text

Statistics from Altmetric.com
The McDonald criteria allow multiple sclerosis (MS) to be diagnosed in patients with a clinically isolated syndrome (CIS) who have MRI evidence of dissemination in time and space.1–3 There have been successive versions of the criteria in 2001,1 20052 and 20103 with different requirements for dissemination in time and space. Although each version has been shown to have a high sensitivity and specificity for the development of clinically-definite MS (CDMS), few studies have investigated how much sooner4 and how more often5 MS can be diagnosed in patients with CIS using the McDonald criteria.
We recruited 178 patients with CIS presenting to Moorfields Eye Hospital and the National Hospital for Neurology and Neurosurgery between 1995 and 2004. The study was approved by ethics committees at both hospitals. Patients were seen at baseline, then for follow-up after 3 months, 1 year, 3 years and 6 years. At each study visit informed consent was obtained. Patients were assessed with a detailed review of neurological symptoms and neurological examination. Relapses were recorded at study visits, but patients were also encouraged to contact the research team at the time of new neurological symptoms. MRI of the brain and whole spine was obtained at each visit on the same 1.5 T Signa scanner, as described elsewhere.6 Each scan was reviewed by a neuroradiologist blinded to the patient's clinical status. The number, location and activity (ie, gadolinium enhancement) of T2 lesions was recorded.
During follow-up CDMS was defined according to Poser criteria. The McDonald criteria were applied retrospectively and MS diagnosed when MRI criteria for dissemination in time/space were met or at the time of a second clinical attack, whichever occurred first.1–3 Only patients with at least one follow-up MRI and at least 36 months of clinical follow-up were included in this analysis. Comparison of within-patient times to MS diagnosis by each diagnostic criterion used the non-parametric one-sample Wilcoxon signed-rank test, since time differences were skewed. Proportions of diagnoses by the different criteria in the same patients were compared using McNemar's test for paired proportions (exact form). Analyses were carried out in Stata 13.1 (Stata Corporation, College Station, Texas, USA). Statistical significance is reported at p<0.05.
One hundred and fifty-seven patients (mean age 32.4 years, 64% female) had sufficient clinical and MRI follow-up to be included in this analysis. CIS locations were optic neuritis in 128, brainstem 18, spinal cord 10 and hemispheric 1. Mean follow-up was 5.8 years (range 3.0–11.9 years). One patient was treated with disease-modifying therapy prior to developing CDMS.
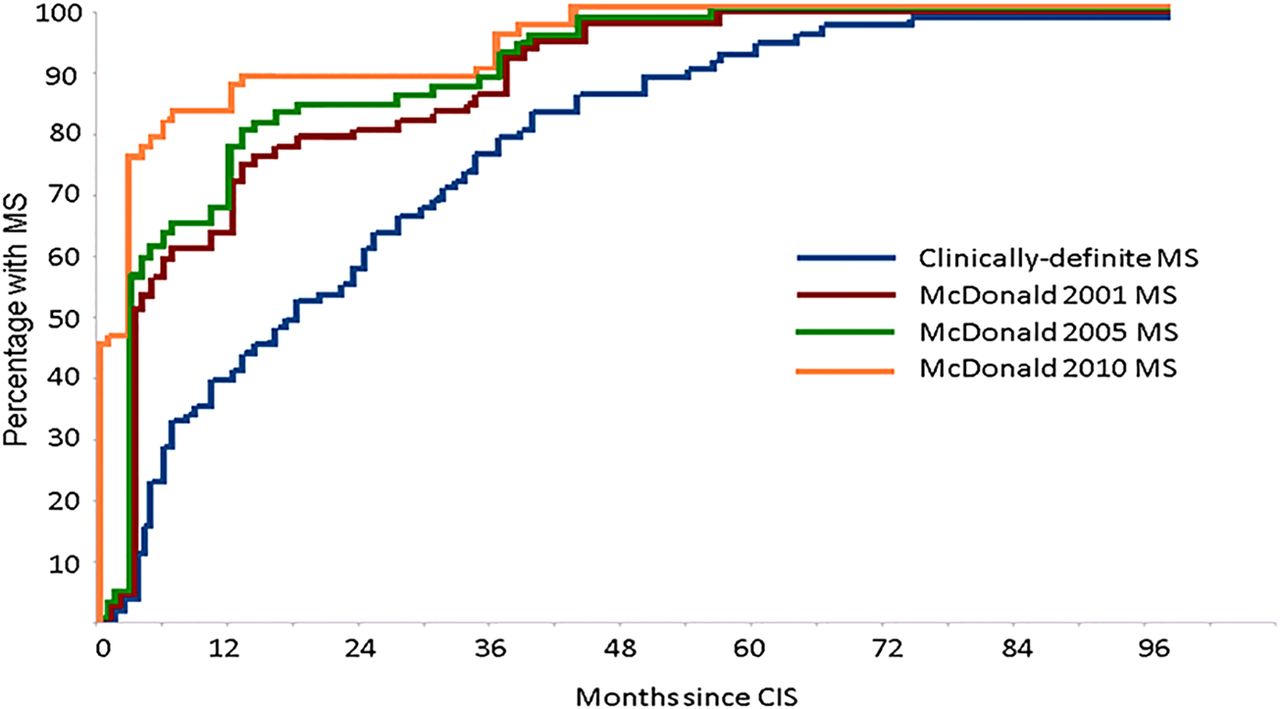
Seventy-one (45%) patients were classified as CDMS, 69 after a second clinical attack and two developed secondary progressive MS following a CIS. Figure 1 shows Kaplan-Meier curves for the time to diagnosis of MS using the Poser and McDonald criteria for patients with CIS who developed CDMS. Mean time to CDMS was 23.1 months compared with 12.0, 10.5 and 6.2 months using the 2001, 2005 and 2010 McDonald criteria (p<0.0001 for comparisons with time to CDMS).

{kind=link}
Kaplan-Meier survival curve showing time to diagnosis of multiple sclerosis (MS) using Poser and McDonald criteria among patients with clinically isolated syndrome who developed clinically-definite MS.
Of 86 (55%) who did not have a second attack, 24 (28%), 26 (30%) and 36 (42%) satisfied 2001, 2005 and 2010 McDonald criteria with MRI evidence of dissemination in time and space (MRI-only MS). Significantly more patients with CIS had MRI-only MS when applying the 2010 criteria, compared with the 2001 (p=0.0002) and 2005 criteria (p=0.001). Most patients with MRI-only MS satisfied the MRI criteria in the first year after CIS; 18 (75%), 18 (69%) and 26 (75%) patients using the 2001, 2005 and 2010 criteria respectively.
When all 157 patients with CIS were considered together, 71 (45%) had CDMS, 36 (23%) had MRI-only MS and 50 (32%) did not have MS using the 2010 McDonald criteria after 6 years.
Establishing a diagnosis of MS at an earlier time point provides an explanation for worrying symptoms and allows for timely discussions about the nature of MS and its management, including use of disease-modifying treatments. In this large CIS cohort, MS was diagnosed significantly earlier using the McDonald criteria. The time gain with each revision of the criteria reflects the less stringent requirements for dissemination in time and space, while retaining high specificity.1–3 Among patients with CIS in this study who ultimately developed CDMS, the mean time to diagnosis of MS halved from 12 months with the 2001 criteria to 6.2 months with the 2010 criteria, a time gain of 16.9 months compared with mean time to CDMS. The time gain using the McDonald criteria was significantly greater in this study than in a previous hospital-based series.4 However, in that study spinal imaging was not performed and not all patients had postcontrast T1-weighted scans or follow-up MRI, both important for demonstrating dissemination in time.
The McDonald criteria identify a significant number of patients with CIS with MRI evidence of dissemination of time and space in the absence of further clinical events,5 and the number has increased as the criteria have been revised. These patients probably have a form of MS that remains largely subclinical. Given the relatively high frequency of MRI-only MS (almost a third of those diagnosed using the 2010 criteria), the possibility arises that the new diagnostic criteria are identifying a milder form of MS than in the past when the diagnosis was based on clinical course alone. There is the potential for the natural history of relapse-onset MS to be being favourably modified by changes to the diagnostic criteria, independent of any effect of disease-modifying treatments.7 These issues are important when counselling patients with CIS about prognosis and in deciding whether to initiate treatment.
One potential limitation of our study is an over-representation of patients with optic neuritis, which may have a more benign prognosis that other CIS types.8 However, almost 80% of patients with optic neuritis had baseline MRI abnormalities, indicating a group at high-risk for developing MS.
In conclusion, the McDonald criteria allow MS to be diagnosed sooner and more often in patients with CIS. While the McDonald criteria facilitate an earlier diagnosis of MS, up to a third of patients with CIS who satisfy the 2010 criteria do not have further clinical events, at least in the medium-term.
Footnotes
-
Contributors WJB and DHM were involved in the conception and design of the study. JKS recruited and obtained consent from participants and conducted the MRI analysis. DRA conducted the statistical analysis. All authors contributed to preparation of the manuscript.
-
Competing interests OC receives grant support from the Multiple Sclerosis Society of Great Britain and Northern Ireland, UCLH-UCL Biomedical Research Centre and honoraria from Novartis, Bayer Schering and GE. She is a member of the editorial board of Neurology. DHM has received honoraria through payments to his employer, UCL Institute of Neurology, for Advisory Committee and/or Consultancy advice in multiple sclerosis studies from Biogen Idec, GlaxoSmithKline, Novartis, Merck, Chugai, Mitsubishi Pharma Europe and Bayer Schering Pharma. He has also received compensation through payments to my employer for performing central MRI analysis of multiple sclerosis trials from GlaxoSmithKline, Biogen Idec, Novartis and Merck.
-
Ethics approval Ethics committees at Queen Square and Moorfields Eye Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Clinical and MRI data are available for collaborative studies and can be requested by non-profit researchers.