Article Text

Abstract
Background In recent years, a relationship between Helicobacter pylori and many disease conditions has been reported, however, studies in its relationship with multiple sclerosis (MS) have had contradictory results.
Objective To determine the association between the H. pylori infection and MS.
Methods 550 patients with MS were included in the study and were matched by gender and year of birth to 299 controls. Patients were assessed for clinical and demographic parameters. An enzyme immunoassay was used to detect the presence of specific IgG antibodies against H. pylori in the serum sample of both groups.
Results H. pylori seropositivity was found to be lower in the patients with MS than in controls (16% vs 21%) with the decrease pertaining to females (14% vs 22%, p=0.027) but not males (19% vs 20%, p=1.0). When adjusted for age at onset, year of birth and disease duration, H. pylori seropositive females presented with a lower disability score than seronegative females (p=0.049), while among males the reverse was true (p=0.025). There was no significant association between H. pylori seropositivity and relapse rate.
Conclusions Our results could reflect a protective role of H. pylori in the disease development. However, it may be that H. pylori infection is a surrogate marker for the ‘hygiene hypothesis’, a theory which postulates that early life infections are essential to prime the immune system and thus prevent allergic and autoimmune conditions later in life. The fact that the association between H. pylori seropositivity and MS risk was seen almost exclusively in females requires further investigation.
- MULTIPLE SCLEROSIS
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is a heterogeneous, immune-mediated demyelinating disease of the central nervous system.1 Pathogenesis involves a complex interaction between genetic and environmental factors.2–6 Recently, many studies indicated a steady increase in autoimmune disease incidence in developed countries, which could suggest that the concurrent decline in infectious disease prevalence might explain the increased autoimmune disease incidence.7 ,8 About half of the world's population is infected with Helicobacter pylori.9 H. pylori infection is more prevalent in developing countries, while the incidence is decreasing in Western countries. The lower rate of infection with H. pylori in the West is largely attributed to higher hygiene standards and widespread use of antibiotics.10
While the majority of H. pylori hosts remain asymptomatic, infection with it has a role in chronic gastritis, peptic ulcer disease, low-grade gastric mucosa-associated lymphoid tissue lymphoma and non-cardia gastric adenocarcinoma.11–13 H. pylori may also play a role in some extragut conditions.14 Paradoxically, there are many studies reporting benefits of infection, including a reduction in the likelihood of developing atopic disorders later in life if infected with H. pylori in childhood.15 Relatively unclear is any association it may have with a potentially autoimmune demyelinating condition such as MS.
The contradictory findings concerning the association between H. pylori infection and MS based on low numbers of patients16–21 led us to study a large group of Western Australian patients.
Methods
Research participants
A total of 550 Caucasian patients enrolled into the Perth Demyelinating Disease Database (PDDD)22 with a diagnosis of MS according to the McDonald criteria23 were included in the study. The study population included 412 (75%) female cases and 138 (25%) male cases. Serum samples were collected from these patients between the years of 2007 and 2011 with an average age at time of collection of 47.7 (range 15–83). Patients with MS were matched based on gender and year of birth (within 2 years) to the control group consisting of 299 individuals of Anglo-Celtic descent from the Busselton Community Health Study (BCHS). The study protocol was approved by the Sir Charles Gairdner Hospital Human Research Ethics Committee, and informed consent was obtained from all participants in the PDDD cohort. Approval for use of control samples was provided by the BCHS ethics committee.
Data recorded
Patients were assessed in the MS clinic by the same two neurologists (AGK and WMC) at the time of collecting samples. Data recorded included: gender, age at onset of initial symptoms, disease duration and clinical course, relapse rate, and Extended Disability Status Scale (EDSS) score at the last visit.
Serology
Anti-H. pylori serology was performed on patients and on controls at the PathWest Automated Serology Laboratory at the Queen Elizabeth II Medical Centre. An enzyme immunoassay was used to detect the presence of specific IgG antibodies (Ab) to H. pylori in the test sample according to the manufacturer's protocol using a BEP2000 system (Enzygnost, Germany). Briefly, serum samples were diluted in a ratio 1:20 using sample buffer then added to the test plate containing inactivated H. pylori antigen. Sample buffer was added along with positive and negative controls and the plates were incubated at 37˚C for 30 min. After washing, rabbit antihuman peroxidase-IgG Ab was added and samples were incubated for 30 min at 37° C. Following washing, colourimetric substrate was added and samples were incubated at 20˚C for 30 min in the dark. The reaction was terminated by adding stopping solution. The test plates were read at 450 nm with a reference wavelength of 650 nm. A positive result for anti-H. pylori Ab was accepted for samples with a concentration greater than 10 U/mL.
Statistical analysis
Comparisons of cases and population-based controls matched 1:1 on the basis of gender and year of birth were carried out via an exact binomial test on the paired differences and also using conditional logistic regression to incorporate additional covariates. Within the cases, associations of seropositivity rates with multiple covariates were assessed by logistic regression. The EDSS from the last visit was analysed by censored Gaussian regression to accommodate six censored values whose lower bounds only were available. EDSS values were approximately proportional to the square roots of disease duration, hence analyses were based on the ratios EDSS/sqrt (Disease Duration). Analyses were carried out using TIBCO Spotfire S+8.2 (TIBCO Software, Inc, Palo Alto, California, USA).
Results
Frequency of H. pylori seropositivity in patients with MS and healthy controls
Demographic and clinical data of patients with MS and healthy controls is presented in table 1.
Demographics and clinical features of patients with MS and HC from Western Australia
The rate of H. pylori seropositivity in the 299 matched cases was marginally lower than among the controls (p=0.056 unadjusted, p=0.045 adjusted for gender). However, the differences in H. pylori seropositivity pertained almost exclusively to the females (p=0.03), while there was no significant difference in cases versus controls for the males (p=1.0; figure 1A). Comparison of the rates of seropositivity between the matched and non-matched cases did not find any significant differences after adjusting for gender (p=0.2), nor was there any difference in the male/female ratio between matched and unmatched cases (p=0.2). The sampling design did not allow disentanglement of the effects of age of sampling and year of birth, and there was little overlap in birth years for the non-matched cases and the controls. To increase numbers in the comparisons we therefore also created strata based on 2-year age-at-sampling intervals using all the data and carried out case–control analyses using conditional logistic regression, including only those strata in which cases and controls were both represented. In these analyses, cases had a significantly lower seropositivity rate after adjusting for gender (p=0.005), with the effect again notable among the females (p=0.002) and not males (p=0.79; figure 1B).

Frequency of Helicobacter pylori seropositivity in patients with multiple sclerosis and healthy controls. (A) H. pylori seropositivity rate was significantly lower in cases than in healthy controls (p=0.045) when matched by year of birth. The difference was significant in females (p=0.03) but not in males (p=1.0). (B) H. pylori seropositivity was overall significantly lower in cases (p=0.005) than in controls when matched by age at sample collection. The effect was significant among females (p=0.002) but not males (p=0.79). *p Values based on matched groups and adjusted for gender in the overall comparison.
Association of H. pylori seropositivity with EDSS and relapse rate
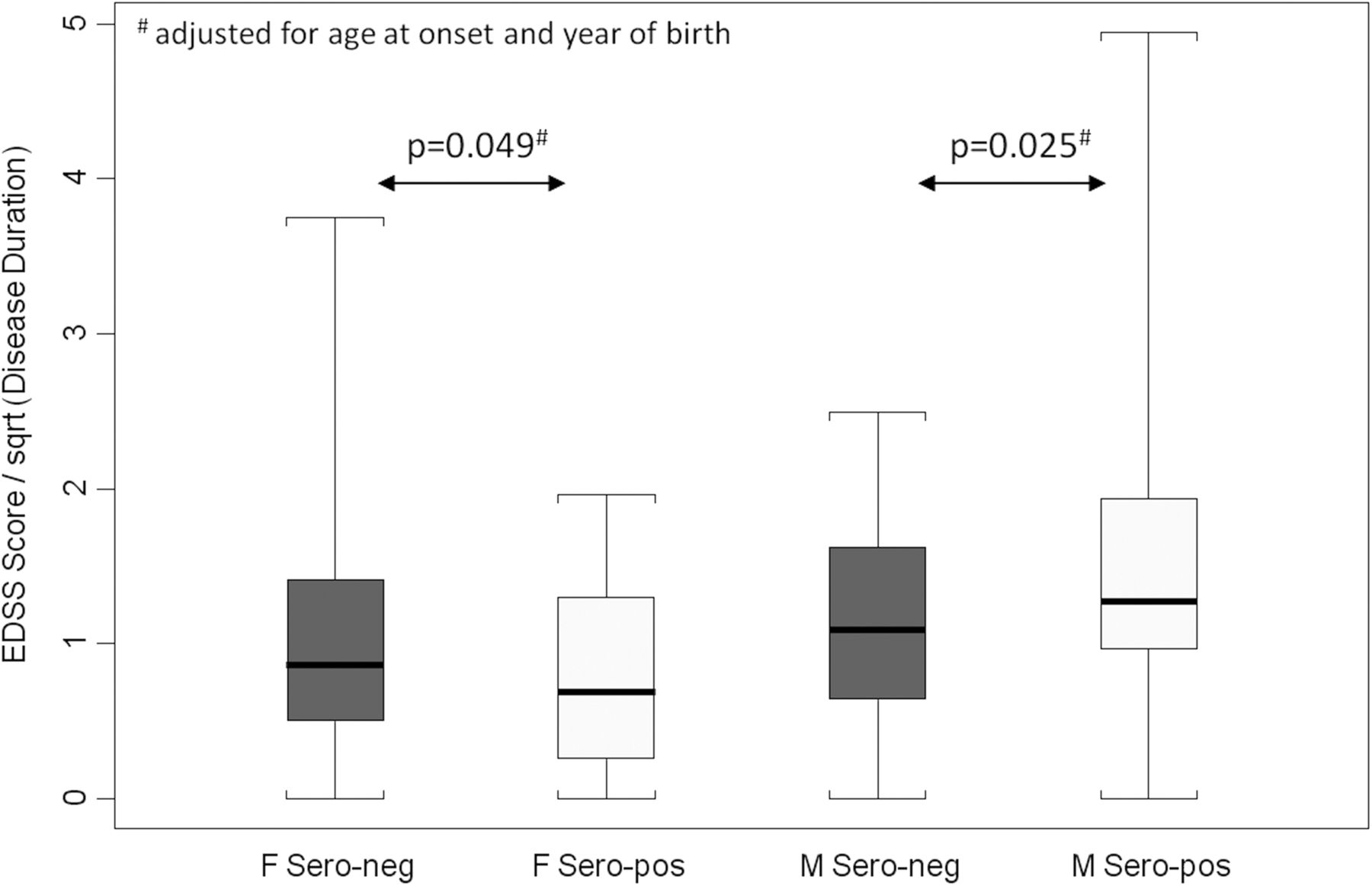
When adjusted for age at onset and year of birth there was a significant interaction effect of gender and H. pylori seropositivity on the scaled EDSS/sqrt (Disease Duration) values (p=0.003). There was only marginal evidence of difference between the female and male seronegative cases (p=0.066). However, the female seropositive cases were lower than the corresponding female seronegative cases (p=0.049) while the male seropositive cases were higher than the male seronegative cases (p=0.025), figure 2. There was no significant association between H. pylori seropositivity and relapse rate after adjustment overall (p=0.61) for females (p=0.63) or for males (p=0.99).

Association of Helicobacter pylori seropositivity and EDSS score/sqrt (Disease Duration). On adjustment for age and year of birth, EDSS score/sqrt (Disease Duration) significantly interacted with gender and H. pylori seropositivity (p=0.003). The effect was present in females in whom seropositivity was significantly higher than seronegativity (p=0.049), and males in whom seropositivity was significantly lower than seronegativity (p=0.025; EDSS, Extended Disability Status Scale; F-sero-neg, female seronegative; F-sero-pos, female seropositive; M-sero-neg, male seronegative; M-sero-pos, male seropositive; sqrt, square root).
The rate of H. pylori seropositivity is related to the primary progressive course of MS for females
Rates of H. pylori seropositivity were assessed among cases for association with age at sample collection, age at onset, year of birth, gender and primary progressive (PP) status using all the case data. After adjustment for the other variables, there was a significant interaction between gender and PP status (p=0.037), with a significant increase in seroprevalence rates for PP cases compared with non-PP cases among females (p=0.026), but not among males (p=0.88; figure 3).

Frequency of Helicobacter pylori seropositivity in primary progressive (PP) and not PP multiple sclerosis cases. Rates of H. pylori seropositivity were assessed among cases for association with age at sample collection, age at onset, year of birth, gender and PP status using all the case data. After adjustment for the other variables H. pylori seropositivity was associated with PP disease course overall (p=0.082). When broken down by gender the effect was significant among females (p=0.026), but not among males (p=0.88).
Overall, there was no significant association among MS cases of carriage of DRB1*1501 and seroprevalence rate (p=0.16). However, within the males there was a significant association (p=0.028), with DRB1*1501 males having higher seroprevalence (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between Helicobacter pylori seropositivity and a carriage of DRB1*1501. Significant association between DRB1*1501 carriage rate and H. pylori seroprevalence was seen in males only (p=0.028), but not the group as a whole (p=0.16). *p Values exact.
Discussion
A steady decrease in H. pylori infection has been observed in most populations in recent decades, more accentuated in wealthy Western countries. The prevalence of H. pylori infection in Australian adults is lower than that in other developed countries. The overall seroprevalence of H. pylori infection in Australia in 2002 was 15.1%, with no statistical difference between genders.24 H. pylori infection is most common among those living in areas of socioeconomic disadvantage or those who were born overseas.25
The present study demonstrates that H. pylori infection is lower in female patients with MS than in healthy controls. It is important to point out that the incidence of MS is increasing over the last decades, and this is mainly driven by an increase of MS in women, resulting in a higher female/male (F/M) rate. In this study, the F/M ratio was 2.7/1 (matched cases) or 3/1 (non-matched cases).
In our study, we enrolled 550 patients with conventional MS and 299 carefully selected community-based controls. Such numbers represent the largest number ever evaluated in regard to association between H. pylori infection and MS. Rates of H. pylori seropositivity were assessed among cases for association with disease course. We found evidence of an association with PP course, but interestingly, again only among females. Previous much smaller studies on the association between H. pylori and MS were contradictory. Some authors stated strong positive association between H. pylori infection and MS,18 and others found that patients with MS presented with lower H. pylori seroprevalence than healthy controls,16 ,17 ,20 while some did not find any correlation.19 ,21 ,26 Our large controlled study indicates a difference in H. pylori seropositivity between Western Australian patients with MS and healthy controls, but only among females. Our observations suggest that infection with H. pylori can be a protective factor against MS risk in Western Australian females.
A protective role of H. pylori infection is consistent with the hygiene hypothesis, which postulates that infections in early life may prime the immune system, and suppress allergic and autoimmune conditions in later life.27 Also in favour of a protective effect is the finding that infection with H. pylori can reduce the prevalence of allergic disorders by 30% compared with non-infected individuals,15 and likewise infection with a parasite could be a protective factor in MS.6 One simplistic explanation for this may be that a bacterial infection can promote a T helper type 1 (Th1) response, shifting the balance away from Th2 cells. Given that it is Th2 cells that are involved in hypersensitivity and atopic disorders, it is reasonable to conclude that this shift may be responsible for the aforementioned reduction in incidence of atopic disorders. Additionally, a study by Lynch et al28 found that individuals infected with parasites experienced recurrence of allergic symptoms when treated with antiparasitic agents. These findings lend weight to the hypothesis that past infections have a protective effect on autoimmune disease. It has already been hypothesised that should H. pylori be confirmed to have a protective effect against MS, H. pylori pharmaceutical products could provide a novel means of treatment via nanoparticle delivery to neuron-specific targets.29
In a number of studies it has been shown that the major histocompatibility complex class II genes are important genetic factors that influence MS susceptibility. In Caucasians, the HLA-DRB1*1501 allele is strongly associated with MS,30 but we found little evidence of association between HLA-DRB1*1501 allele and H. pylori seroprevalence that was limited to males only.
In summary, H. pylori infection is associated with a slight but significant reduction of MS risk in Western Australian women. Prior publication differences concerning the association between H. pylori infection and disease risk could be due to differences in the size of sample groups, differences in ethnicity, time of infection, or perhaps different subtypes of MS. A lower frequency of H. pylori infection might be a reflection of good sanitation in developed countries. One weakness of our study might be that we were not able to control for country of birth and ethnicity. This could result in spurious findings. However, most of our patients with MS were born in Australia, UK or other Western countries. Even if we did not have this information for our community-based controls, it is known that Western Australia has a relatively stable population, largely of Anglo-Celtic descent, thus it would be unlikely that we would find significant differences in country of birth between patients with MS and controls. Future studies could address this issue. The differences observed here were not due to changes in behaviour after MS onset, as infection usually occurs in early childhood. The reason why the influence of H. pylori infection on MS risk affects females only is unknown and warrants further investigation.
Acknowledgments
The authors thank all participants in the Perth Demyelinating Disease cohort as well as the Busselton cohort participants for their involvement.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
MJFP and AS contributed equally to this study.
Contributors MJFP contributed in the drafting and revising of the manuscript, and in the analysis and interpretation of the data. AS and KAB contributed in the analysis and interpretation of data, and in the revising of the manuscript. AJTW was involved in the clinical data collection and revising of the manuscript. IJ participated in the statistical analysis and manuscript preparation, and in the revising of the manuscript. JB was involved in the consultation for neurology patient care, and in the revising of the manuscript. BJM performed critical revision of the manuscript. WMC was involved in the consultation for neurology patient care, and in the critical revision of the manuscript. AGK was involved in the consultation for neurology patient care, and contributed in the study conception and designing, analysis and interpretation of data, and critical revision of the manuscript.
Competing interests BJM has received funding from The University of Western Australia and from NHMRC Sir Macfarlane Burnet Fellowship grant (572723). He is a substantial owner of Ondek, a company attempting to develop biological delivery systems from Helicobacter. WMC received speaker honoraria and membership of scientific advisory boards from Bayer Schering, Novartis, Merck Serono, Sanofi, and Biogen-Idec. AGK received speaker honoraria and scientific advisory board fees from Bayer, Biogen-Idec, Novartis, Sanofi-Aventis, Merck, Sanofi-Genzyme and Innate Immunotherapeutics. Dr KAB and Dr AJTW were supported by Multiple Sclerosis Research Australia Vacation Scholarships.
Patient consent Obtained.
Ethics approval Sir Charles Gairdner Hospital Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.