Article Text

Abstract
Objectives We recently showed that diminished motor cortical excitability is associated with high levels of post-stroke fatigue. Motor cortex excitability impacts movement parameters such as reaction and movement times. We predicted that one or both would be influenced by the presence of post-stroke fatigue.
Methods 41 first-time stroke survivors (high fatigue n=21, Fatigue Severity Scale 7 (FSS-7) score >5; low fatigue n=20, FSS-7 score <3) participated in the study. Movement times, choice and simple reaction times were measured in all participants.
Results A three way ANOVA with fatigue (high and low), task (movement time, simple reaction time and choice reaction time) and hand (affected and unaffected) as the three factors, revealed a significant difference between affected (but not unaffected) hand movement times in the high compared to low fatigue groups. Reaction times, however, were not different between the high-fatigue and low-fatigue groups in either the affected or unaffected hand.
Conclusions Previously, we showed that motor cortex excitability is lower in patients with high post-stroke fatigue. Our current findings suggest that post-stroke fatigue (1) is a problem of movement speed (possibly a consequence of diminished motor cortex excitability) and not movement preparation, and (2) may have a focal origin confined to the lesioned hemisphere. We suggest that low motor cortex excitability in the lesioned hemisphere is a viable therapeutic target in post-stroke fatigue.
- STROKE
Statistics from Altmetric.com
Video abstract
Introduction
Post-stroke fatigue is a common disabling symptom described as the ‘feeling arising from difficulty in initiation of or sustaining voluntary effort’. Identifying therapeutic targets for interventions requires a better understanding of its neurobiological basis.1 We recently showed that high post-stroke fatigue was associated with low motor cortical excitability2 but was not related to finger dexterity, grip strength, sustained attention index and information processing speed. However, suppressing motor cortical excitability can alter movement times as well as reaction times.3 Movement time reflects efficiency of cortical control of musculature that depends on primary motor cortex excitability,4 whereas reaction times reflect movement preparation along with a small component of the time for movement initiation.5 Based on our previous finding of reduced motor cortex excitability in the lesioned hemisphere of those with high post-stroke fatigue,2 we hypothesised that (1) patients with significant fatigue would have slowed movement times; (2) reaction times would be less affected as the movement component is small; (3) these behavioural effects would be unilateral, reflecting lesion specific alteration in corticomotor processing.
Methods
This is a cross-sectional observational study approved by the Riverside Research Ethics Committee (12/LO/1474). Stroke survivors were recruited consecutively via the Stroke Research Networks from 11 NHS Trust hospitals and community stroke groups.
Forty-one stroke survivors (see online supplementary table) with first-time ischaemic or haemorrhagic lesion with either high or low fatigue participated following informed written consent. Fatigue Severity Scale (FSS-7), a validated fatigue scale,6 was used to quantify fatigue. Stroke survivors with a FSS-7 score of ≥5 were defined as high fatigue and ≤3 as low fatigue. The cut-off points for high and low fatigue were derived from our previous study.2 Exclusion criteria: centrally acting medication, high Hospital Anxiety and Depression Scale (>11) and poor function as described previously.2 Those with poor function were excluded from the study as high functioning stroke survivors, both physically and cognitively, generally report higher levels of fatigue.7
Participants performed two visually cued reaction time tasks: simple reaction and movement time task (SRT) and choice reaction time task (CRT).
SRT task: participants pressed down on home button (H) until a light emitting diode (LED) (see online supplementary figure) flashed. In response to the LED, participants were instructed to move their hand as quickly as possible to a target button (T), press T and return to H. 25 trials were performed. Cues were 10 s apart (±20% random variance in the inter-cue interval). The events of cue presentation, H release and T press down were recorded using Spike software (Spike 2 V.6.15).
CRT task: participants placed their right and left index fingers on buttons Rt and Lt, respectively (see online supplementary figure). The task was to respond to an LED flash with the appropriate button press. 50 such trials were performed, 25 for each hand. The order of presentation was randomised, inter-cue interval and recording software were similar to SRT software.
Average across 25 trials of time between cue presentation and H release was SRT. Average across 25 trials of time between H release and T press was movement time (MT). Choice reaction time (CRT) was the time between presentation of cue and button press. An average across 25 trials was taken as the Rt and Lt CRT.
Three way between-groups ANOVA was used to examine the main effects and interactions of the following three factors. Factor 1: ‘arm’: affected and unaffected. Factor 2: ‘fatigue’: high and low fatigue. Factor 3: task: SRT, CRT and MT. Post hoc pairwise multiple comparisons procedures were performed using the Holm-Sidak method. Between group analyses were performed for the factors ‘age’, ‘time post stroke’, ‘NHPT’, ‘ARAT, ‘grip strength’ and ‘SDMT’.
Results
There were no significant differences between the high-fatigue and low-fatigue groups for the factors ‘age’, ‘time post stroke’, ‘NHPT’, ‘ARAT’, ‘grip strength’ and ‘SDMT’.
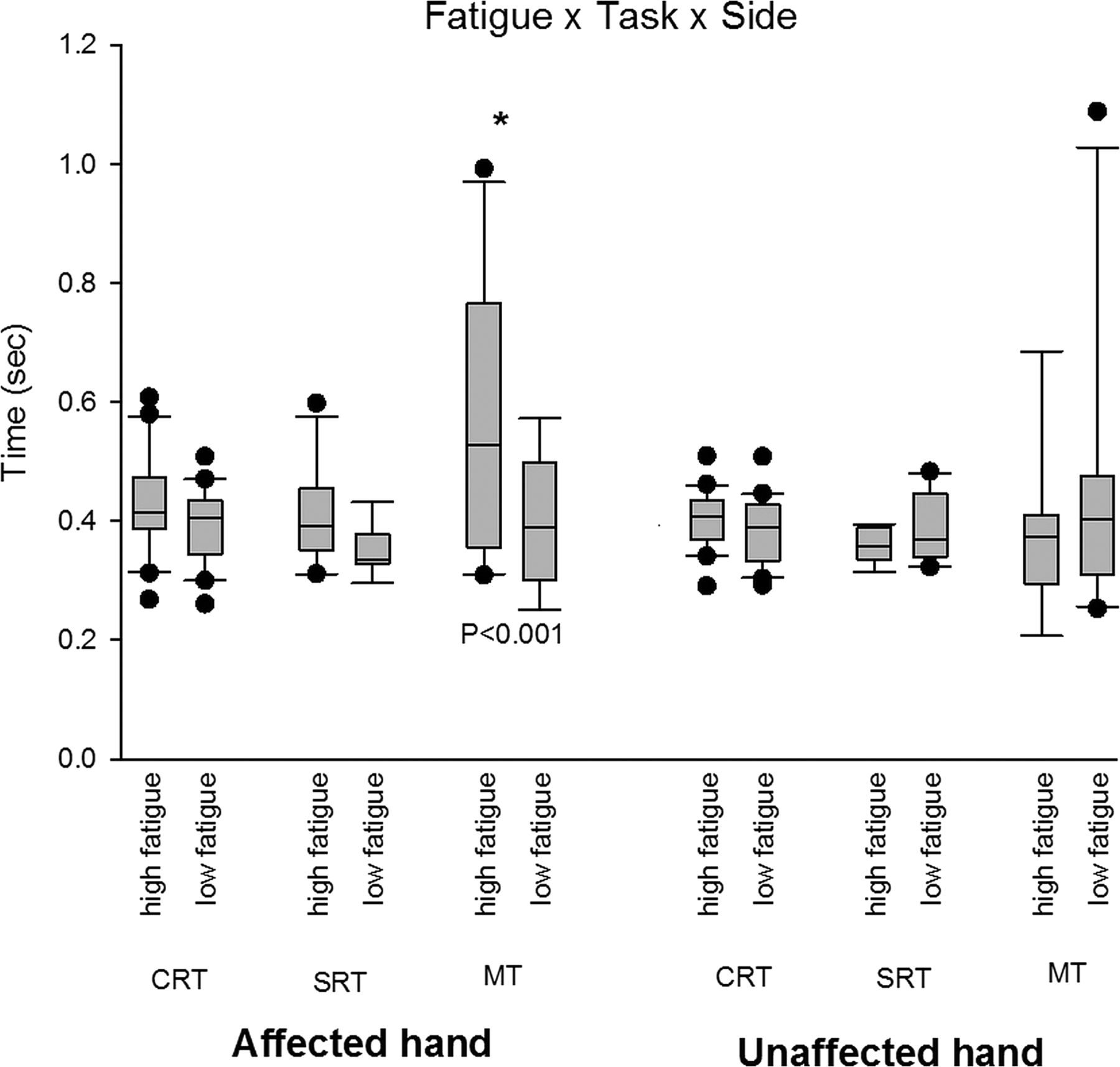
Three-way ANOVA results (figure 1): A 2 (fatigue levels)×3 (task types)×2 (affected arm) analysis of variance (ANOVA) was performed on task times.

{kind=link}
The time (y axis) taken to perform the various tasks (simple reaction and movement time task (SRT), choice reaction time task (CRT) and movement times (MT)) with either the affected or unaffected hand in the high-fatigue and low-fatigue groups are depicted as box and whisker plots in this figure. A significant difference was seen between the MT of the affected hand, between the low-fatigue and high-fatigue groups (p<0.001). Differences between high-fatigue and low-fatigue groups in the SRT, CRT and unaffected hand MT were not significant.
There was a significant main effect of task, F(2,146)=5.008, p=0.008. There was no significant main effect of fatigue (p=0.078) or arm (p=0.085). A possible significant main effect for both parameters was masked by presence of significant interaction between the factors.
There was a statistically significant three-way interaction between fatigue, task and arm, F(2,146)=3.602, p=0.03. Therefore, any significant interaction between fatigue and task depends on whether it is the affected or unaffected hand. Analysis of interaction effects showed a significant interaction between fatigue levels and task performed (p<0.001) by the affected but not unaffected hand (p=0.2). This indicates the difference between high and low fatigue is not the same across all three tasks, MT, SRT and CRT in the affected hand. In the unaffected hand, difference between high-fatigue and low-fatigue groups is not significantly different between the three tasks.
A post hoc pairwise multiple comparisons procedure using the Holm-Sidak method revealed a significant difference between high and low fatigue movement times in the affected hand (p<0.001), but not in SRT and CRT.
Discussion
Understanding the neurobiological basis of post-stroke fatigue is crucial if novel therapeutic strategies to combat this disabling symptom are to be developed. Here, we describe three new findings that contribute to this understanding. First, movement times during rapid ballistic movement are slower in those with high fatigue; second, this effect is seen only in the affected side; third, reaction times with either hand were no different in those with or without fatigue.
We recently showed diminished motor cortical excitability in the affected side of high-fatigue stroke survivors,2 and here we propose that slowing of movement speed on the affected side is a consequence of low motor cortical excitability.4 A rapid ballistic movement requires a burst of maximal muscle force in the shortest possible time. Such muscle activity depends heavily on the ability of the motor cortex to quickly activate the necessary output pathways, which in turn depends on the ‘readiness to act’ or motor cortex excitability. Indeed, it has been shown that ballistic movements are particularly susceptible to reductions in motor cortex excitability.4 Slowing of movement in an affected but not unaffected hand is an important finding, as it lends support to the idea that post-stroke fatigue may arise directly from altered corticomotor control of the lesioned hemisphere.
It is unclear how a reduction in movement velocity might relate to the generalised sensation of fatigue. One possible explanation relates to altered sensory processing. Processing of self-generated sensory afferent activity by volitional movement is normally attenuated.8 This attenuated sensory processing results in underestimation of effort invested into an action. Disturbing the attenuation process by reducing motor cortex excitability results in tasks feeling more effortful to perform.9 If one considers for a moment a classic force matching task, altered sensory attenuation results in an increased sense of effort. However, in our task, there was no ‘matching’, as participants were simply asked to move quickly and so any increase in sense of effort required to complete the task (in our high-fatigue group) might more likely lead to slowing of voluntary movement speed. However, we did not test whether participants were capable of higher speeds in the affected hand.
The simple and choice reaction times in this study were similar, in contrast to previous reports where simple reaction times were significantly shorter than choice reaction times.10 This difference may be the result of the different tasks being used for the simple and choice reaction times. The SRT task involved an antigravity movement of releasing a button, while the CRT task involved a gravity-assisted movement of pressing a button. Additionally, the reaction times on average were longer than previously reported times,10 which could be attributed to the long inter-cue interval of 10 s with a variability of 20%. The lack of difference between the high-fatigue and low-fatigue group reaction times, during both choice and simple tasks, suggests that fatigue may not depend on movement-related cognitive processes such as decision-making. Fatigue in neurological conditions, for example, Parkinson's disease11 and multiple sclerosis,12 is often seen as predominantly cognitive. Our results suggest that post-stroke fatigue is a fundamentally different clinical entity and that treatment strategies will not generalise across diseases. Post-stroke fatigue is a result of corticomotor deficits and not a cognitive disorder.
In conclusion, we show that post-stroke fatigue is associated with altered corticomotor control but not motor-related decision-making and planning. We build on our recent finding of lowered corticomotor excitability seen in high-fatigue stroke survivors2 by identifying a behavioural correlate that could be a direct result of lowered excitability. These results are a step towards understanding the neurobiological basis of fatigue after stroke.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online tables
Footnotes
Contributors AK was responsible for identifying the need for research into motor behavioural correlates of post-stroke fatigue, designed the study, collected data for the study, performed all the statistical analysis for the study and prepared the manuscript. EVC contributed substantially towards identifying suitable fatigue patients for the study and recruited them into the study. KSS assisted the first author with the data collection sessions. JCR contributed towards the study design and made an intellectual contribution towards manuscript preparation. NSW substantially contributed towards manuscript preparation and towards patient recruitment.
Funding This study was funded by the Stroke Association; AK holds a Stroke Association Senior Research Training Fellowship, TSA/SRTF 2012/01.
Competing interests AK, EVC, KSS and NSW have no disclosures to report. JCR received the following grants—Medical Research Council: MR/K01384X/1, Stroke Association: TSA 2010/06 and TSA 2014/ 04.
Ethics approval Riverside REC 12/LO/1474.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary