Article Text

Abstract
Migraine is a highly prevalent and disabling neurological disorder associated with a wide range of psychiatric comorbidities. In this manuscript, we provide an overview of the link between migraine and several comorbid psychiatric disorders, including depression, anxiety and post-traumatic stress disorder. We present data on psychiatric risk factors for migraine chronification. We discuss the evidence, theories and methods, such as brain functional imaging, to explain the pathophysiological links between migraine and psychiatric disorders. Finally, we provide an overview of the treatment considerations for treating migraine with psychiatric comorbidities. In conclusion, a review of the literature demonstrates the wide variety of psychiatric comorbidities with migraine. However, more research is needed to elucidate the neurocircuitry underlying the association between migraine and the comorbid psychiatric conditions and to determine the most effective treatment for migraine with psychiatric comorbidity.
- MIGRAINE
- NEUROEPIDEMIOLOGY
- NEUROPSYCHIATRY
- NEURORADIOLOGY
- PSYCHOPHARMACOLOGY
Statistics from Altmetric.com
Introduction
Migraine affects 12% of adults in the USA, making this condition a common concern for many patients and their doctors.1 Often overlooked is the high prevalence of psychiatric comorbidities associated with migraine, such as depression, anxiety and post-traumatic stress disorder.2–4 Migraineurs with psychiatric comorbidity have higher healthcare utilisation tendencies than migraineurs without psychiatric comorbidity.5 If left untreated, these comorbid psychiatric conditions can increase the risk of migraine chronification, the evolution of episodic migraine (EM) into chronic migraine (CM) (ie, at least 15 headache days a month, including at least 8 days/month with full-blown migraines). In addition, if left untreated, the comorbid psychiatric conditions can increase migraine-related disability, reduce quality of life and negatively impact treatment outcomes.
Here, we describe the epidemiology of psychiatric comorbidities associated with migraine, and describe some screening tools for diagnosing these comorbidities. Following this, we describe recent functional neuroimaging findings and theories that might help to elucidate the connection. We then provide an overview of migraine treatment options, including pharmacological and behavioural therapies with a special emphasis on treating patients with psychiatric comorbidities.
Psychiatric comorbidities associated with migraine
Depression
Psychiatric comorbidities are common in migraine patients (table 1).
Prevalence of common psychiatric comorbidities in patients with migraine
Depression is one of the most common psychiatric comorbidities in patients with migraine. Three different studies found that migraineurs are over 2.5 times more likely to suffer from depression compared with non-migraineurs.6–8 A meta-analysis of data from 12 studies on migraine and depression found that the incidence of depression in migraineurs is highly variable, ranging from 8.6% to 47.9%.9
The association between migraine and major depressive disorder is even stronger for patients with CM and for patients who have migraine with aura.10 The relationship between migraine and depression appears to be bidirectional.7
There is no current evidence that improved control of depression helps to control migraines. However, it is important to identify and treat depression in patients with migraine because it is a significant predictor of migraine chronification.10 Furthermore, migraineurs who suffer from depression are more likely to be refractory to migraine treatments and to suffer from medication overuse and disability.11
The efficacy of tricyclic antidepressants in prevention of migraine suggests a shared causative mechanism for depression and migraine.12 The current hypotheses to explain this shared causative mechanism include serotonergic dysfunction, hormonal influences and sensitisation of the sensory and emotional neural networks.13
Bipolar spectrum disorder
There seems to be a bidirectional relationship between migraine and bipolar disorder. Patients suffering from migraine with aura are three times more likely to suffer from bipolar disorder than the general population.14–16 Conversely, about one-third of patients with bipolar disorder have migraine. The prevalence of migraine was higher among people with bipolar disorder type II (54.17%, 95% CI 31.52 to 75.95) compared with bipolar disorder type I (32.7%, 95% CI 18.16 to 49.19).17
Bipolar disorder comorbidity with migraine seems to be a subtype of bipolar disorder with an unstable rapid cycling course, an increased prevalence of comorbid panic attacks, an earlier age of onset and increased prevalence in women.18 ,19
Bipolar disorder and migraine share similar features. They are both episodic, worsened by stress, associated with a family history of affective disorders and migraine, and responsive to anticonvulsants such as valproate.20 Although there is still much to learn about the neurobiology of both disorders, they are thought to share a common pathophysiology involving dysfunction of calcium channels.18
Anxiety disorders
More than half of the patients with migraine will meet the criteria for at least one anxiety disorder in their lifetime. Anxiety disorders are two to five times more prevalent in patients with migraine than in the general population, up to two times more common in patients with migraine than in patients with depression, and much more common in patients with CM than in patients with EM.21 Depression is often comorbid, with anxiety disorders in patients with migraine.22 Among the anxiety disorders, generalised anxiety disorder (GAD), obsessive compulsive disorder (OCD) and panic disorder (PD), are the most strongly linked with migraine.22
Patients with GAD are at increased risk for migraine (OR 3.86, 95% CI 2.48 to 6), and patients with migraine are at increased risk for GAD (OR 3.13, 95% CI 1.56 to 6.3).23
Patients with OCD are at increased risk and higher frequency of migraine (OR 4.57, 95% CI 2.82 to 7.83 for migraine 2–6 times/week).24 The OR of PD in migraine is 3.76, and is even greater in patients with migraine with aura.25 PD is associated with increased migraine frequency, increased disability, higher risk of chronification and higher risk of medication overuse.25 Migraine and PD share features such as functional impairment, gastrointestinal (nausea), autonomic (dizziness), affective (fear) symptoms during attacks, and worry about further attacks between attacks.25
Patients with migraine with a comorbid anxiety disorder spend US$4634 more per year in healthcare than those without comorbid anxiety.26 One study found that a family history of anxiety was associated with self-reported usage of non-pharmacological treatments for headache. However, most of the participants in non-pharmacological treatments who reported such use, were not those with grade A evidence.27 Controlling anxiety of patients with migraine is associated with improved quality of life, adherence to a migraine treatment plan, and effectiveness of migraine treatment.22
The relationship between anxiety disorders and migraine seems to be bidirectional.25 Both anxiety and migraine have been associated with a higher frequency of the s allele in a study of the 5HTTLPR polymorphism of the serotonin transporter gene, implying a common genetic predisposition.28 Current hypotheses on the neurobiological mechanism underlying the association between anxiety and migraine include serotonergic dysfunction, dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, hormonal influences and psychological factors, such as interoceptive conditioning, pain-related cognition, avoidance learning and anticipatory anxiety.25 ,29
Stress
Stress is a prevalent migraine trigger. Patients with migraine tend to suffer from high levels of stress, especially those with CM.30 The Frequent Headache Epidemiology Study suggested that patients with CM had more major life events in the year preceding the chronification of their migraines than did patients with EM.31 The Longitudinal Brazilian study (ELSA-Brasil) showed an association between negative life events and increased frequency of migraine.32 Stress management with relaxation therapies, biofeedback and cognitive behavioural therapies were proven to be effective migraine prophylaxis measures.33–37
Chronic repeated stress (including repeated migraines) leads to allostatic dysfunction, manifested as both structural and functional damage.38 ,39 These negative changes impact pain processing, induce central sensitivity, and might affect the pain experience in patients with migraine.33 ,39 In response to a painful heat stimulus, patients with migraine have more activation on their functional MRI (fMRI) studies in the perigenual cortex than patients without migraine, which was found to be the brain area associated with allostatic dysfunction in rats.40 The overuse of analgesic and headache symptomatic medications might affect allostasis too. Patients with CM with medication overuse were found to have impaired secretion of the growth hormone, ACTH and cortisol.41 The degree of endocrine dysfunction seemed to be correlated to the duration of the CM.41
In addition, stress reduction is associated with increased risk of migraine the following day, which could support the biological associations between stress and headaches discussed above.42 Indeed, stressors activate the autonomic nervous and neuroendocrine systems, which leads to increased glucocorticoids, and hence, anti-inflammatory and antinociceptive effects. These processes are reversed when the stress ends, which could precipitate a migraine.42
Stress also affects psychiatric disorders. Stressful events, especially early in life, increase the incidence and susceptibility of major depressive disorder and other psychiatric disorders. Chronic stress early in life and in adulthood can decrease the expression of glucocorticoid receptors (GR) upregulate the expression of the cochaperone gene, FKBP5, which restrains GR activity by limiting the translocation of the receptor complex to the nucleus, and alter transcriptional activity. As a result, chronic stress can impact gene function, response to future stressors and susceptibility to further stressors, migraine, and psychiatric disorders.43
Abuse and post-traumatic stress disorder
Migraine is more prevalent in patients with a history of emotional abuse, physical abuse, physical neglect and/or sexual abuse compared with the general population (OR 1.6–1.8).44 This association is maintained independently of comorbid depression and/or anxiety in the case of emotional abuse.45 Childhood emotional abuse is a risk factor for migraine chronification, more disabling migraines, allodynia and earlier onset of migraines.46 There appears to be an association between the number of adverse childhood events (ACE score) and migraine frequency.44 Patients with headache with a history of emotional abuse, emotional neglect and/or sexual abuse are more likely to suffer from migraines than tension headaches.45 One hypothesis for the association between abuse and migraine involves cortisol dysfunction and stress reactivity. Perhaps past abuse modifies the HPA axis leading to greater stress reactivity and migraine.47 ,48
However, recent studies suggest that abuse is not independently associated with migraine, and that post-traumatic stress disorder (PTSD) mediates the association. A cross-sectional study that compared patients with and without migraine showed that PTSD (OR 2.3, 95% CI 1.56 to 3.39), but not trauma alone (OR 1.17, 95% CI 0.85 to 1.61), is a predictor of migraine.25 In veterans, PTSD is associated with increased consumption of prescription medications for headaches (used as a marker of headache), more in men (OR 5.2 with 95% CI 2.4 to 11.1) than in women (OR 2.0 with 95% CI 1.1 to 3.7). No associations were found between either lifetime or combat traumatic events and use of prescription medication for headaches.49
Persons with headache and a history of abuse or neglect are more likely to have migraine than tension-type headache warranting an increased index of diagnostic suspicion for migraine. Knowledge of abuse and neglect makes it more likely that headaches are attributable to migraine. In addition, the psychological consequences of abuse and its sequelae, including PTSD and depression, are important treatable comorbidities of migraine. This is especially important because migraineurs with PTSD were found to have greater disability and more lost work days due to physical or mental health or substance abuse (8 days for migraineurs with PTSD compared with 2.6 days for migraineurs without PTSD, adjusted rate ratio 2.77 (95% CI 2.45 to 3.14)), and more difficulties with developing and maintaining a social life than migraineurs without PTSD (adjusted OR 2.32 (95% CI 1.15 to 4.09)).50 ,51 Cognitive–behavioural therapy (CBT) for PTSD was found to improve the disability of patients with migraine with comorbid PTSD.52
PTSD is much more prevalent in patients with migraine than in the general population (14–25% vs 1–12%), and is even more prevalent in patients with CM compared with patients with EM (43% vs 9%), despite a similar frequency and prevalence of trauma exposure between the groups.53–55 Patients with migraine have increased lifetime and 1 year ORs of PTSD compared with the general population.56 On the one hand, PTSD increases the risk of migraine development.56 On the other hand, patients with migraine might suffer from increased allostatic loads and subsequent maladaptive stress responses, which might predispose them to PTSD.56 Current hypotheses on neurobiological mechanism underlying the association between PTSD and migraines include serotonergic, autonomic nervous system, and HPA axis dysfunction. This would also explain why both PTSD and migraine have mood and anxiety disorder comorbidities.57
Adult attention deficit hyperactivity disorder
There is extremely limited data on migraine and attention deficit hyperactivity disorder (ADHD). A cross-sectional study reported an increased prevalence of migraine in patients with persistent ADHD compared with the general population (OR 1.67, 95% CI 1.28 to 2.17).58 Of note, comorbid depression and anxiety were more prevalent in patients with persistent ADHD suffering from migraines than in those without migraines.58
Sleep
Sleep disorders are more prevalent in patients with migraine than in the general population.59 The Third Nord-Trondelag Health Study showed an increased risk of severe sleep disturbances as measured by the Karolinska Sleep Questionnaire and the Epworth Sleepiness Scale with migraine (OR 5.4, 95% CI 2 to 14.5).60 More than half the patients with migraine report sleep difficulties at least occasionally, and more than a third of them suffer from frequent sleep difficulties and chronic short sleep (≤6 h per night).61 Chronic short sleep was found to be associated with more severe headaches.61 In terms of sleep diagnoses, migraine is associated with a wide variety of sleep disorders, such as restless leg syndrome, parasomnias, sleep apnoea and insomnia.62 A small randomised placebo-controlled trial showed significant improvement in headache frequency and severity, and sometimes even a reversal from CM to EM in patients who underwent behavioural sleep modification compared with a placebo intervention.63 Controlling a patient's sleep apnoea was found to have a positive effect on their chronic migraines.59
The relationship between migraines and sleep is bidirectional: on the one hand, sleep disturbances (such as, excess of, lack of, or irregular sleep) are known triggers and risk factors for migraines, and on the other hand, migraines interfere with patients’ quality of sleep.64 The neurobiological mechanism underlying this relationship is likely due to some overlapping pathophysiology and shared anatomical structures within the brain.65 In addition, depression and anxiety are comorbid with both sleep disorders and migraine.
Substance abuse
Prior studies have suggested an association between migraine and increased risk of substance abuse and addiction.66 ,67 A study showed that 19% of opioid-dependent patients started opioids because of headache.68 However, this association was not found in later studies.69 The association between migraine and substance abuse was no longer statistically significant in the analysis of the National Comorbidity Survey Replication data when adjusting for the depression, and PTSD confounders.56
There is no known association between alcohol use disorder and migraine. In a large population-based study, the 12-month prevalence of alcohol dependence measured by the World Mental Health Composite International Diagnostic Interview was similar among migraineurs and controls.3 In a cross-sectional study, migraineurs consumed less alcohol than controls (2.34 vs 2.92 drinks per week, p=0.038); these findings may be explained by the fact that alcohol is a headache trigger in 37.8% of migraineurs and a consistent trigger in 10% of migraineurs.70 ,71 In addition, migraineurs have a lower alcoholic beverage threshold for alcohol-delayed headache. The relationship between alcohol and headaches is thought to be mediated by the 5-hydroxytryptamine system.71
Personality disorders
The diagnoses of personality disorders remain a matter of debate in the psychiatric community. The Diagnostic and Statistical Manual of Mental Disorders (DSM)-V does not have an axis II anymore; however, the 10 diagnoses of personality disorders were retained, although the decision to keep them is not widely accepted. Furthermore, the pathophysiology of personality disorders is still unknown. Thus, personality disorders are beyond the scope of this review.72
Screening tools for psychiatric comorbiditiy
Screening for comorbid psychiatric disorders in persons with migraine has been recommended.73 A number of instruments are also available to screen for general psychiatric symptoms and specific conditions, such as depression, anxiety and bipolar disorder (see table 2 for a detailed list of screening tools). Screening is especially important if patients or families report symptoms of depression and anxiety, or if the clinician observes dysphoric or anxious moods.73 ,74 While some have advocated verbal screening with informal questions (eg, ‘Do you feel depressed?’, ‘Do you worry frequently?’),75 we prefer the use of the four depression and anxiety questions from the Patient Health Questionnaire (table 2).76 ,77 Patients who present to headache specialty clinics, and/or patients who are unsuccessful with standard treatment, often warrant more detailed assessment for psychiatric comorbidities.78
Screening tools
Psychiatric comorbidity and the relationship with migraine chronification
Longitudinal studies have demonstrated that in persons with EM, CM develops at the rate of about 2% to 3% per year.79 The development of CM and its rate of onset in patients with EM are associated with a number of risk factors, including depression and anxiety, stressful life events, snoring, obesity, comorbid pain disorders and overuse of medication.10 ,30 ,31 ,45 Depression was a significant predictor of onset of CM (OR=1.65, 95% CI 1.12 to 2.45), after adjusting for sociodemographic variables and characteristics of headache.10 Additionally, risk of CM onset increased with depression severity. Relative to study respondents with none or mild depression, those with moderate (OR=1.77, 95% CI 1.25 to 2.52), moderately severe (OR=2.35, 95% CI 1.53 to 3.62) and severe depression (OR=2.53, 95% CI 1.52 to 4.21) were at increased risk for the onset of CM at increasingly higher rates.10 ,79 On the contrary, psychiatric comorbidities are more prevalent in CM than in EM.80 ,81
Current hypotheses on the neurobiological mechanism underlying the contribution of depression and anxiety to progression of migraine include shared dysfunction of the serotonergic system, overuse of medication derived from a lack of appropriate coping behaviours, and inherent ideology that magnifies pain and unpleasant associated features.82
Theories and evidence underlying the relationship between migraine and psychiatric comorbidities
There are four general categories for explanation of comorbidity.83 First, there may be a unidirectional causal relationship among disorders. For example, if recurrent unpredictable attacks of headache lead to depression as the sole explanation of comorbidity, we would predict that persons with migraine would be at increased risk for depression, but that depression would not be a risk factor for migraine. Available data demonstrates a bidirectional relationship between migraine and depression; persons with either disorder are predisposed to the other, undermining the unidirectional causal explanation. Second, migraine may be comorbid due to a common environmental risk factor. For example, if head injury predisposed both to migraine and anxiety, the link between them could be accounted for by this exposure. Third, migraine may be linked to psychiatric comorbidities through a shared genetic risk factor.15 Finally, other biological, environmental or genetic risk factors may converge to produce a brain state which predisposes to both disorders.9 For example, serotonergic dysfunction, HPA hyperactivity and inflammation could predispose both to migraine and psychiatric comorbidities such as depression. Several systems seem to be involved in the intrinsic relationships between migraines and psychiatric comorbidities, such as stress, insomnia, serotonergic dysfunction, HPA axis hyperactivity, inflammation, hormonal influences, central sensitivity/sensitisation of the sensory and emotional neural networks, and shared genetic risk factors. On the one hand, frequent migraines add to the allostatic load which eventually leads to allostatic dysfunction and central sensitivity. On the other hand, chronic stress, subsequent allostatic dysfunction and central sensitivity predispose to both migraines and psychiatric disorders, such as depression, anxiety and PTSD. Insomnia is comorbid to migraines, depression, anxiety and PTSD. Migraine and psychiatric disorders negatively impact sleep quality. Also, on the other hand, poor sleep quality predisposes to migraines. Serotonergic dysfunction, HPA axis hyperactivity, hormonal influences, inflammation and sensitisation of the sensory and emotional neural networks are common ingredients to both migraine and psychiatric disorders, such as depression, anxiety and PTSD. Inflammatory markers were found to be elevated in both depression (tumour necrosis factor (TNF) α, C reactive protein (CRP) and interleukin (IL) 6) and migraine (CRP).84–86
Higher frequency and severity of headache seem to correlate with a heavier burden of psychiatric comorbidities.9 This dose-dependent association is not specific to migraine, but also seems to be present between other chronic pain disorders and psychiatric comorbidities, which raises the question of whether these associations might all, at least partially, be explained by central sensitivity or by neurotransmitter interactions in the trigeminothalamic pathway of migraines. Depression, anxiety, stress, irritability and sleep affect the homeostasis of the transmission of the headache-related nociceptive signals from the thalamus to the cortex (and even prior to the thalamus in the case of serotonin). These signals are affected by different neurotransmitters, including serotonin, noradrenalin and dopamine. In the thalamocortical signal transmission from the thalamus to the cortex, burst discharges are associated with acute pain, whereas tonic discharges are associated with chronic pain. However, additional excitatory inputs can change the firing mode from burst to tonic, and inhibitory input can change the firing mode from tonic to burst. This could explain the impact of psychiatric comorbidities on migraine chronification.87
Knowledge learned from imaging studies: how functional imaging studies might lend insights into shared pathophysiology between migraine and psychiatric comorbidities
Research neuroimaging studies provide insights into the emotional component of migraine symptoms and might provide insights into the comorbidity between migraine and psychiatric disorders. Migraine studies demonstrate abnormal function, structure and connectivity of brain regions that play important roles in determining emotional responses to pain and to other sensory stimuli, and in determining general affect and mood. Greater pain-induced functional activation, and stronger functional connectivity of these regions, likely contribute to determining the emotional aspect of migraine symptoms, and could partially account for the coexistence of psychiatric disorders with migraine.
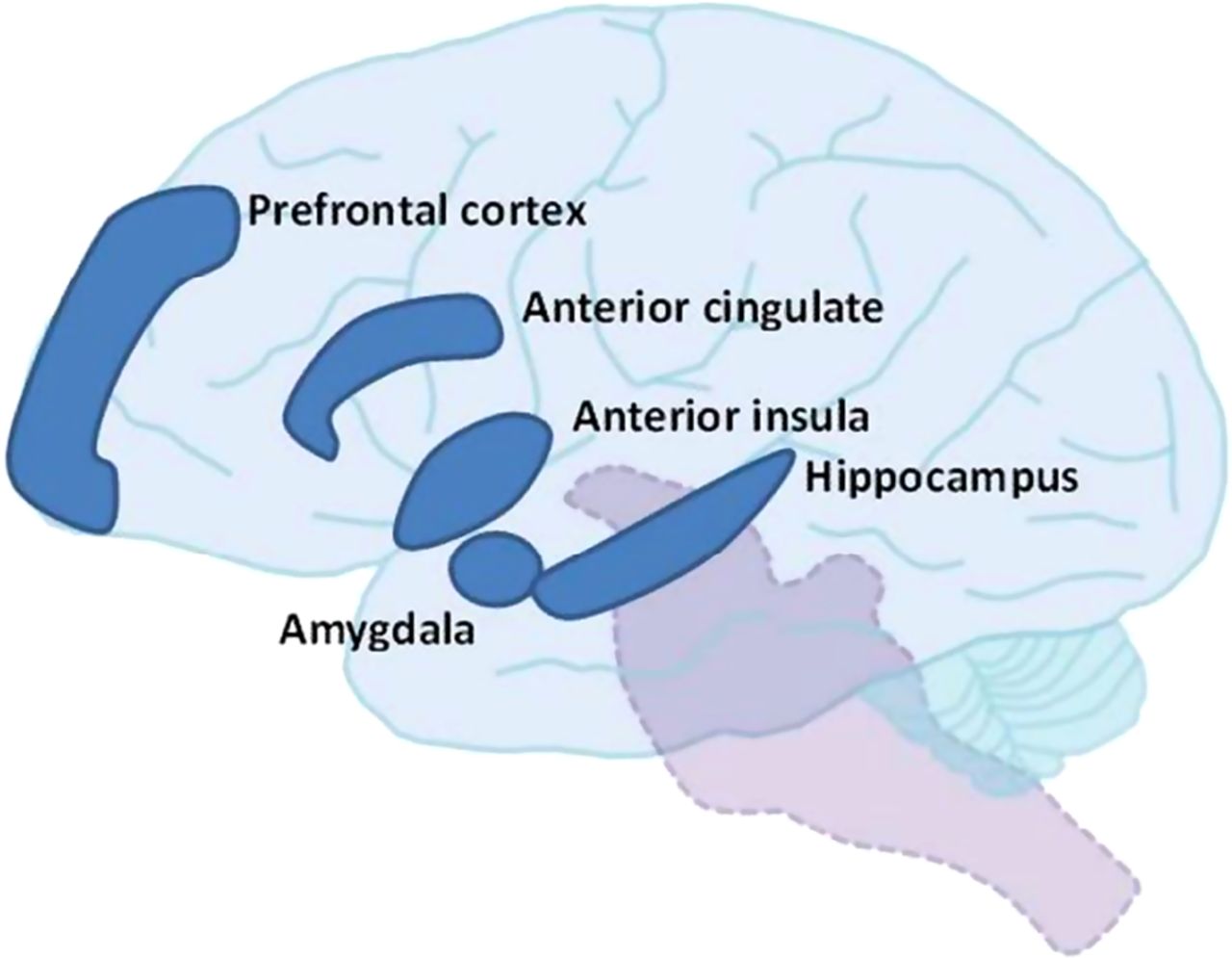
Affective-motivational brain regions that have been commonly identified as having abnormal function or structure in migraine studies include: anterior cingulate cortex, anterior insula, prefrontal cortex, hippocampus and amygdala.88–100 Figure 1 illustrates these brain regions.
{kind=link}
Affective-motivational brain regions commonly identified as having abnormal function or structure in migraine studies.
Within the realm of a migraine study, atypical structure and function of these regions are usually interpreted as being associated with atypical affective-motivational processing of noxious stimuli, including the emotional reactions to migraine headache, lights, sounds and odours. This theory is supported by studies that demonstrate people with migraine tend to have greater activation of affective-motivational brain regions in response to painful stimuli and stronger functional connectivity between affective-motivational brain regions and those regions responsible for sensory-discriminative processing compared with healthy controls. For example, fMRI studies comparing pain-induced brain activation patterns in people with migraine with healthy controls, have demonstrated people with migraine tend to have greater activation in the hippocampus, prefrontal cortex and anterior cingulate cortex, regions that are involved in the emotional responses to pain.88 ,90 Resting-state functional connectivity studies have shown that compared with healthy controls, people with migraine have stronger connectivity between affective-motivational brain regions and those responsible for sensory-discriminative processing. For example, studies demonstrate that people with migraine have stronger connectivity between anterior insula with primary visual cortex, primary auditory cortex and thalamus, and between amygdala with visceroceptive insular cortex, auditory cortex, thalamus and somatosensory cortex.89 ,91 ,93 Stronger functional connectivity could predispose the person with migraine to greater emotional responses to noxious sensory stimuli during the migraine attack. However, since not all migraine studies have matched subject cohorts on measures of anxiety and depression, or excluded participants with psychiatric disorders, it is possible that anxiety and depression are over-represented within these migraine cohorts. This makes it difficult to determine if imaging findings are due to migraine, to psychiatric comorbidity, or to a combination of both. Brain imaging studies of people with psychiatric disorders demonstrate atypical structure and function of similar regions as those identified as being atypical and important for affective-motivational processing of sensory stimuli in migraine studies.101–106 Similar to people with depression and other psychiatric disorders, people with migraine have atypical function and structure of brain regions that are important for determining affective-motivational responses to sensory stimuli and for determining mood.100 These regions are key components of brain networks implicated in emotion, such as the limbic system, the salience network, and the default mode network. The emotional components of migraine symptoms and the relationships between migraine and comorbid psychiatric disorders might be partially explained by stronger functional activation and connectivity of these brain regions. However, further investigations are required to determine if the atypical imaging findings are a baseline brain trait that predisposes a person to greater emotional responses to painful sensory stimuli as well as to the development of comorbid psychiatric disorders, if they are a result of recurrent migraine attacks that then leads to the development of greater stimulus-induced emotional responses and comorbid psychiatric disease, or if the presence of psychiatric disease leads to changes in these regions that then alter a person's emotional responses to noxious sensory stimuli.
Overview of treatment considerations and options
Migraine attacks are commonly managed by abortive medications such as triptans and non-steroidal anti-inflammatory drugs. When necessary, preventive medications, such as antidepressants, antihypertensives and antiepileptic drugs, are added to the treatment.107 ,108 Beyond medications, behavioural treatments are often used to treat migraine, and have been found to be effective in reducing headache frequency.109 Biofeedback, deep breathing, progressive muscle relaxation and guided imagery-coping skills are often used to help patients successfully manage headaches. Additional cognitive strategies often used include cognitive modification, problem-solving techniques, and cognitive-behavioural stress-management therapy.109 The combination of medication and behavioural therapy has been found to be more effective than either medication or behavioural therapy alone in treating migraine.34 ,37 ,110
Comorbid psychiatric conditions need to be considered when devising a treatment plan for the patient with migraine.21 ,111–113 However, many of the treatments listed above are evaluated in samples of patients without comorbid psychiatric illness, limiting our understanding of how these comorbidities impact outcomes of migraine treatment. The literature that does exist on the impact of psychiatric comorbidities on the effectiveness of headache treatment is mixed. Some studies have cited psychiatric comorbidities as a reason for failure of migraine treatment.114–117 Other studies have indicated that patients with comorbid psychiatric diagnoses show similar rates of improvement after treatment when compared with patients with no comorbid psychiatric diagnoses.118 To date, there is no treatment algorithm for the management of migraine in patients with psychiatric comorbidities. However, a few considerations need to be mentioned.
First, the choice of the migraine-preventive medication in patients with psychiatric comorbidities should be based on psychiatric comorbidity severity, patients’ preference, patients’ risks for adverse events and prior treatment history.11
Second, when the psychiatric comorbidity is mild, monotherapy for migraine prevention and a psychiatric comorbidity can be considered. For example, the migraine preventive propranolol may help with some forms of anxiety. However, when the treatments of the psychiatric comorbidity and migraine do not overlap or the conditions are severe, it is necessary to use separate treatments.119 Examples are discussed in table 3.
Pharmacological treatments used for migraine prevention and psychiatric comorbidities
Using different treatments for migraine and psychiatric comorbidities instead of monotherapy seems to improve outcomes and to minimise side effects.120 Medications used for both migraine and psychiatric comorbidities are usually used at different doses with a different titration plan according to the condition they are intended to treat. Treatments should be reviewed independently for their effectiveness on the condition for which they were prescribed (migraine or psychiatric comorbidity), and potential side effects, and drug-drug interactions should be assessed. The treatment plan should be coordinated between all the physicians involved.120
Third, the treatment of migraine and the psychiatric comorbidities should be carried out in a sequential stepwise manner with close monitoring of potential side effects and treatment interactions.11 Attempts should be made to avoid migraine preventives that can potentially worsen patients’ psychiatric comorbidities. For example, the migraine preventive topiramate can affect mood.120 The data about a potential association between β-blockers and depression are controversial and limited.120 In the event that someone has a psychiatrist, it is advisable to consider discussing potential risks with the patient's psychiatrist before prescribing migraine-preventive medications.
Behavioural treatments (eg, progressive muscle relaxation, biofeedback, CBT) are effective migraine management options with enduring benefits, and are essentially free of side effects.121 ,122 They may be less costly than pharmacological interventions.123 As stated previously, studies have shown that combination pharmacological–behavioural therapy is most effective for migraine treatment.34 ,37 ,124 ,125 Because studies have shown that these American Academy of Neurology/US Headache Consortium level A evidence-based treatments125 have a synergistic effect when combined with medications, consider using them in combination with pharmacological treatments for migraine and/or psychiatric comorbidity. A pilot randomised control trial on CBT for comorbid migraine and major depressive disorder suggests at least a 4-month long improvement in headaches, depression, anxiety and quality of life.126
Fourth, the development of mood disorder symptoms in episodic patients with migraine who do not require preventive therapy may indicate suboptimal migraine management, in which case the physician should decide whether to start the patient on a preventive therapy or on a mood disorder therapy based on the severity of the emerging psychiatric disorder.120
A few studies have been conducted examining how treatment of migraine may impact comorbid psychiatric disorders. A recent pilot study on the effect of onabotulinumtoxin A used for migraine prevention in patients with CM with comorbid depression and anxiety suggested an improvement in depression and anxiety symptoms measured by the Beck Depression Inventory II, Patient Health Questionnaire 9 and (GAD-7.127 However, further studies are needed.
Conclusion
Psychiatric comorbidities have a much higher prevalence in patients with migraine than in the general population, and even more so in patients with CM than in patients with EM. There are hypotheses that could potentially explain the intricate relationships between psychiatric comorbidities but, the biological mechanisms to explain these intricate relationships are still not well understood. Of concern, psychiatric comorbidities seem to increase the risk of development of migraine chronicity, decrease the quality of life of patients with migraine, and complicate migraine management. Since psychiatric comorbidities so intricately affect migraines, their chronicity and their management, it is essential to screen patients with migraine for psychiatric comorbidities. More studies need to be conducted to explicitly address this intersection from a therapeutic point of view given the clinical, functional and cost implications.
References
Footnotes
Competing interests RL reports grants and personal fees from Alder, personal fees from Allergan, personal fees from CoLucid, grants and personal fees from Electrocore, personal fees and other from eNeura, personal fees from Ethicon, personal fees from Merck, grants and personal fees from Novartis, personal fees from Labrys, personal fees from Autonomic Technologies, personal fees from Boston Scientific, personal fees from Bristol Myers Squibb, personal fees from Dr Reddys, personal fees from Eli Lilly, personal fees from Endo Pharmaceuticals, personal fees from Informa, grants from Migraine Research Fund, grants from National Headache Foundation, grants from NIH, personal fees from Teva, personal fees from Vedanta, outside the submitted work. TJS reports personal fees from Allergan, personal fees from Zogenix, personal fees from Supernus, all outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.