Article Text

Abstract
Objectives We investigated long-term (to 25 years) seizure prognosis and survival in people with newly diagnosed epilepsy in the community. We explored whether prognosis is different in those with epilepsy (>2 unprovoked seizures) and those with a single seizure at presentation.
Methods This is a prospective observational cohort study of people with newly diagnosed seizures. We investigated seizure outcome and survival in people presenting with a single seizure and in those presenting with >2 seizures (epilepsy).
Results 695 people (median follow-up 23.6 years) had unprovoked epileptic seizures. For seizure analysis we excluded 38 people with missing data leaving 657 (309 male, and 249 aged <18 years). Seizures recurred in 67%. The 354 people with epilepsy were only slightly more likely to have further seizure recurrence than the 302 people with a single seizure at presentation (HR 1.32, 95% CI 1.09 to 1.59). In 327 people with complete follow-up, 268 (82%, 95% CI 77% to 86%) were in terminal remission; (80%, (95% CI 73% to 85%) in those with epilepsy at presentation). Premature mortality was increased in people with epilepsy (standardised mortality ratio 1.67; 95% CI 1.40 to 1.99) and those with a single seizure at presentation (standardised mortality ratio 2.65; 95% CI 2.23 to 3.15). It is also high in those with early remission.
Conclusions People with epilepsy and with single seizures at presentation in the community generally have good prognosis for seizure control with prolonged follow-up. The risk of premature mortality is significantly increased in both groups.
- EPILEPSY
Statistics from Altmetric.com
Introduction
Epilepsy remains the most common serious neurological disorder, yet there is little information on long-term prognosis.1 Few studies have examined prognosis in unselected or community-based cohorts with more than 10 years follow-up, and report terminal remission in 44–70%.2–5 The UK National General Practice Study of Epilepsy (NGPSE) is a prospective cohort study of people with newly diagnosed seizures set up in 1984 to determine the prognosis of people with new onset seizures.6 The last reports on prognosis were at 9 years follow-up.7 ,8 Long-term mortality to April 2009 has been reported.9 We now provide a comprehensive review of the outcome of those with epileptic seizures up to 25 years after onset, including probability of seizure recurrence, remission, patterns of seizure recurrence and mortality to see whether both seizure prognosis and survival are as usually suggested.
Methods
The methodology of the NGPSE has been previously described.6 Between 1984 and 1987 UK general practitioners (GPs) registered people with newly suspected seizures. Six months after registration a diagnostic panel reviewed all 1195 registered using contemporaneous data.6 Those with a prior diagnosis of epilepsy (104 (9%)) or an alternative diagnosis (79 (7%)) were excluded. For the current analysis we excluded those with febrile seizures (220 (18%)).10 The remaining 792 (66%) were classified as having definite (564 (47%)) or probable epileptic seizures (228 (19%)). Subsequently those with epileptic seizures were classified into four groups: idiopathic/cryptogenic seizures (1980s definition—no identified predisposing cause); remote symptomatic seizures (central nervous system lesions acquired postnatally); acute symptomatic seizures (occurring <3 months after an acute insult); associated with congenital neurological deficits.10 This classification was made using only information available 6 months after the seizure prompting registration (the index seizure) and no changes were made based on future outcomes. Follow-up of those with epileptic seizures used postal questionnaires sent to all individuals’ GPs approximately yearly until 1997, with further follow-up in 2001 and in 2009. For the current analysis, to enable comparison with other cohorts, we excluded people with acute symptomatic seizures (97 (12%)), and analysed those with epilepsy (recurrent unprovoked seizures at presentation) and those with a single unprovoked seizure at presentation separately, as well as the whole group. We also separately analysed those with idiopathic/cryptogenic seizures and the group of people with remote symptomatic seizures (in which we included those with congenital neurological deficits). As sensitivity analyses, the main analyses were repeated in the whole group of people with epileptic seizures, including those with acute symptomatic seizures, and in the subgroup with definite unprovoked epileptic seizures.
A complete description of the methodology of the NGPSE is available in the online supplementary material methods.
Patient involvement
This observational study was started in the 1980s and, although no patients were involved in the design, recruitment or conduct, epilepsy support groups were aware of it.
Statistics
The number of seizures prior to the index seizure was estimated and grouped. The date of the first seizure after the index seizure was noted, as were the date of the first seizure occurring at least 5 years, and at least 10 years, after the index seizure. The date of the last follow-up at which seizure status was recorded was taken as the end of follow-up for analyses of seizure outcome; those with no seizure data were excluded from analysis of seizure outcome. Kaplan-Meier analysis was used to investigate probability of seizure recurrence after the index seizure and after 5 and 10 years after the index seizure. Factors affecting seizure recurrence were determined using Cox regression, unless proportionality assumptions were not met, when the log rank test was used. Competing risks regression with probability of seizure recurrence as the outcome of interest and death as a competing interest was also performed. For analysis of survival, the end of follow-up was death or 5 October 2009, whichever occurred earlier.
For each 12-month period since the index seizure, a dichotomous variable was calculated denoting the presence or absence of seizures during that 12-month period, with no distinction between seizure types. Using these data, time to the completion of the first 3-year and 5-year remissions from the index seizure was noted, as well as presence or absence of the terminal 5-year remission. Patterns of seizure remission and relapse were described, with follow-up duration, using these dichotomous variables; the χ2 test was used to compare those with a single seizure and those with epilepsy. The dichotomous variables were used to construct a graph illustrating the probability of being seizure-free each year stratified on seizure status in the preceding year.
The standardised mortality ratio (SMR) for the whole cohort with unprovoked seizures was estimated as described previously.9 Expected numbers of deaths were estimated using age, sex and calendar year-specific death rates in England and Wales.11 SMRs were also estimated for people with early remission (those who became seizure-free by the second year and subsequently remained seizure-free throughout follow-up), for people with a single notified seizure ever and for those with more than one notified seizure ever. Median duration from index seizure to death was estimated.
Data were analysed using Stata V.13.1 (Texas, USA). CIs for binomial proportions (Wilson method) and differences between proportions (Newcombe method) were calculated using CIA software.12
Results
Demographics
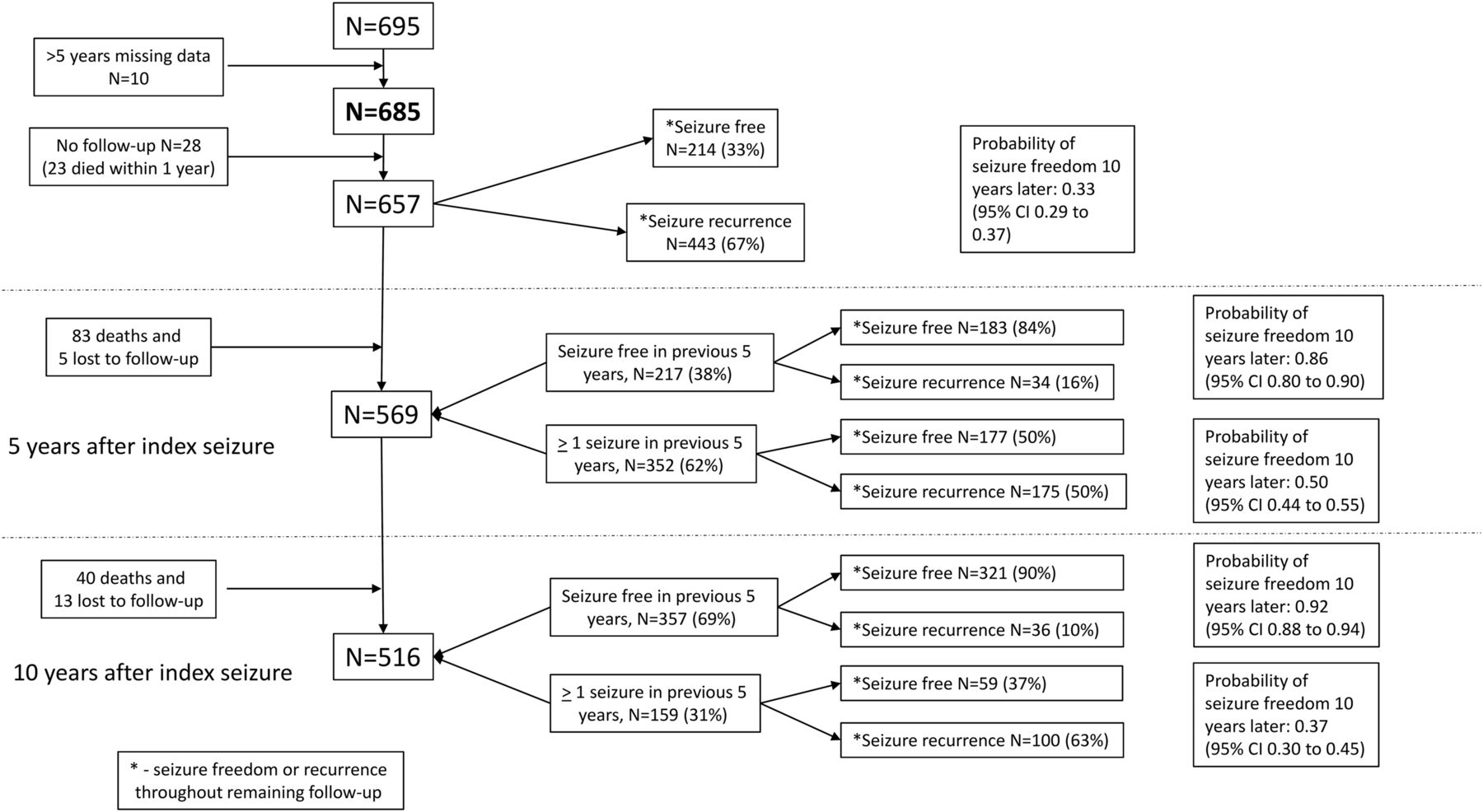
The study profile for the NGPSE is shown in the online supplementary figure. For the whole cohort of 695 people with unprovoked epileptic seizures, the median duration of follow-up (to death or last follow-up) from the index seizure was 16.6 years (IQR 10.2, 24.0); 255 people (37%) died by 5 October 2009. For those alive (n=440) on this date, median duration of follow-up was 23.6 years (IQR 22.2, 24.7).
At the time of GP registration with the study, 370/695 (53%) people had had more than one seizure (‘epilepsy’ group) and 324 (47%) people had had a single seizure (‘single seizure’ group) (table 1); one person was excluded from analyses as we could not determine whether the index seizure was the first.
Study characteristics
Ten individuals had >5 years with missing seizure data but with further follow-up, while 28 people had no seizure follow-up at all; each of these 28 died during the follow-up period, 22 (79%) within 6 months of the index seizure. These 38 people were excluded from the analyses of seizure outcome which are based on the remaining 657 individuals. Three quarters (513 people, 78%) were classified as having idiopathic/cryptogenic seizures and 144 (22%) had remote symptomatic seizures (including those due to congenital neurological deficits).
Probability of seizure recurrence after the index seizure
Seizures recurred in 258/354 (73%, 95% CI 68% to 77%) in those with epilepsy at presentation and in 184/302 (61%, 95% CI 55% to 66%) in those with a single seizure. Those with epilepsy were only slightly more likely to have further seizure recurrence than those with a single seizure (HR 1.32, 95% CI 1.09 to 1.59). Those with greater numbers of seizures before the index seizure were increasingly likely to have further seizure recurrence (compared with those with a single seizure at presentation, HR 1.21, 95% CI 0.99 to 1.48 for those with 1–5 seizures before the index seizure, HR 1.41, 95% CI 0.99 to 2.01 for 6–10 seizures before the index seizure and HR 2.72, 95% CI 1.84 to 4.03 for >10 seizures before the index seizure). Neither sex (HR 0.99, 95% CI 0.82 to 1.19) nor age at index seizure (HR 1.00, 95% CI 0.996 to 1.00) affected probability of seizure recurrence. Those with onset at 18 years or older were less likely to have seizure recurrence; the difference was not significant using standard analyses (HR 0.83, 95% CI 0.69 to 1.01), but it was significant when competing risks analysis was used (Subhazard ratio 0.79, 95% CI 0.66 to 0.96). Table 2 shows the probability of continued seizure-freedom at various time points in the whole cohort, in those with epilepsy and those with a single seizure at presentation, and in those with a single seizure by 5 and 10 years after presentation.
Probability of remaining seizure-free after various periods from the index seizure, in the whole group, and in groups stratified by seizure occurrence
Remission
Details of remission are shown in table 3.
Probability of having experienced a 3-year remission and 5-year remission by 5, 10 and 15 years after the index seizure, and 5-year terminal remission
In 327 people with follow-up to 2009, 268 (82%, 95% CI 77% to 86%) were in terminal remission (ie, no seizures for the last 5 years of follow-up); 204 (76%, 95% CI 71% to 81%) of those were off antiepileptic drugs (AEDs), while six people (all with epilepsy at presentation) were not in remission but not taking AEDs. There was no difference in the percentage in 5-year terminal remission between adults and children.
Outcome after 5 years
The 568 people with >5 years of follow-up were divided into four seizure pattern groups depending on seizures prior to the index seizure and during the first 5 years of follow-up; three people had missing data. Of the others, 113 (20%) had no seizures before the index seizure or during the first 5 years of follow-up, 136 (24%) had no seizures before the index seizure, but had seizures during the first 5 years, 102 (18%) had seizures before the index seizure but not since, and 214 (38%) had seizures before and after the index seizure. The log rank test indicated a significant difference in probability of later seizure recurrence among the groups (p<0.0001) (figure 1).
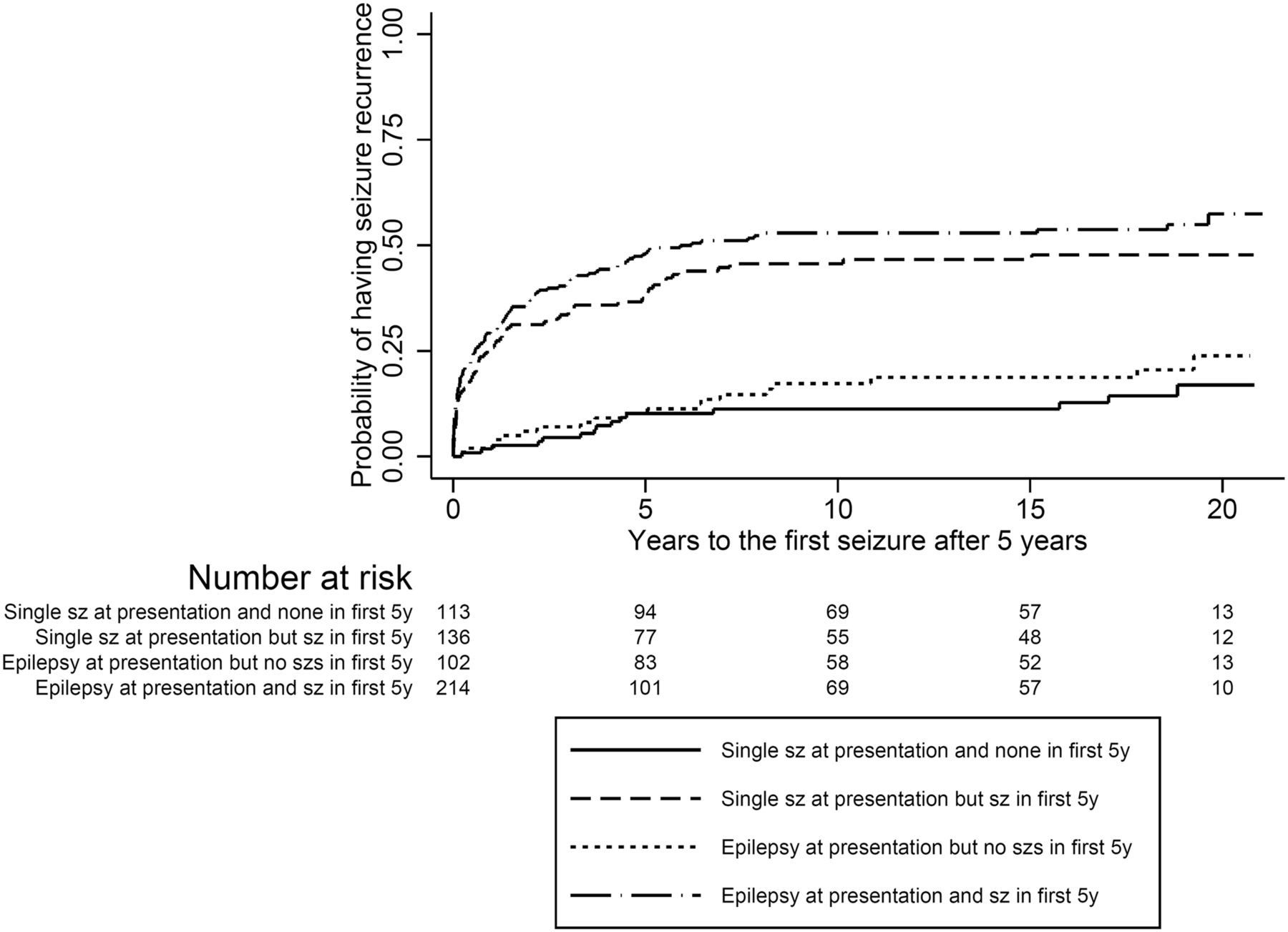
Probability of seizure recurrence after the first 5 years of follow-up. The log rank test indicated a significant difference in probability of later seizure recurrence among the groups (p<0.0001). There was a higher probability of recurrence in the two groups with seizures in the first 5 years than in the two groups with no seizures then (p<0.0001). There were no differences between the two groups without seizures in the first 5 years (p=0.30), or between the two groups with seizures (p=0.17). By 20 years after the index seizure, the probability of remaining seizure-free was: 0.89 (95% CI 0.81 to 0.93) in those with a single seizure at 5 years 0.81 (95% CI 0.71 to 0.88) in those with seizures only before the index seizure 0.53 (95% CI 0.44 to 0.62) for those with seizures only in the first 5 years 0.47 (95% CI 0.40 to 0.54) in those with seizures during both time periods. sz, seizure 5 y, 5 years
Seizure patterns
Patterns of seizure remission and relapse are illustrated in table 4. There was no significant difference in the distribution of pattern groups between those with epilepsy and those with a single seizure at presentation (p=0.084).
Patterns of seizure remission and relapse after the index seizure, based on dichotomous seizure variables
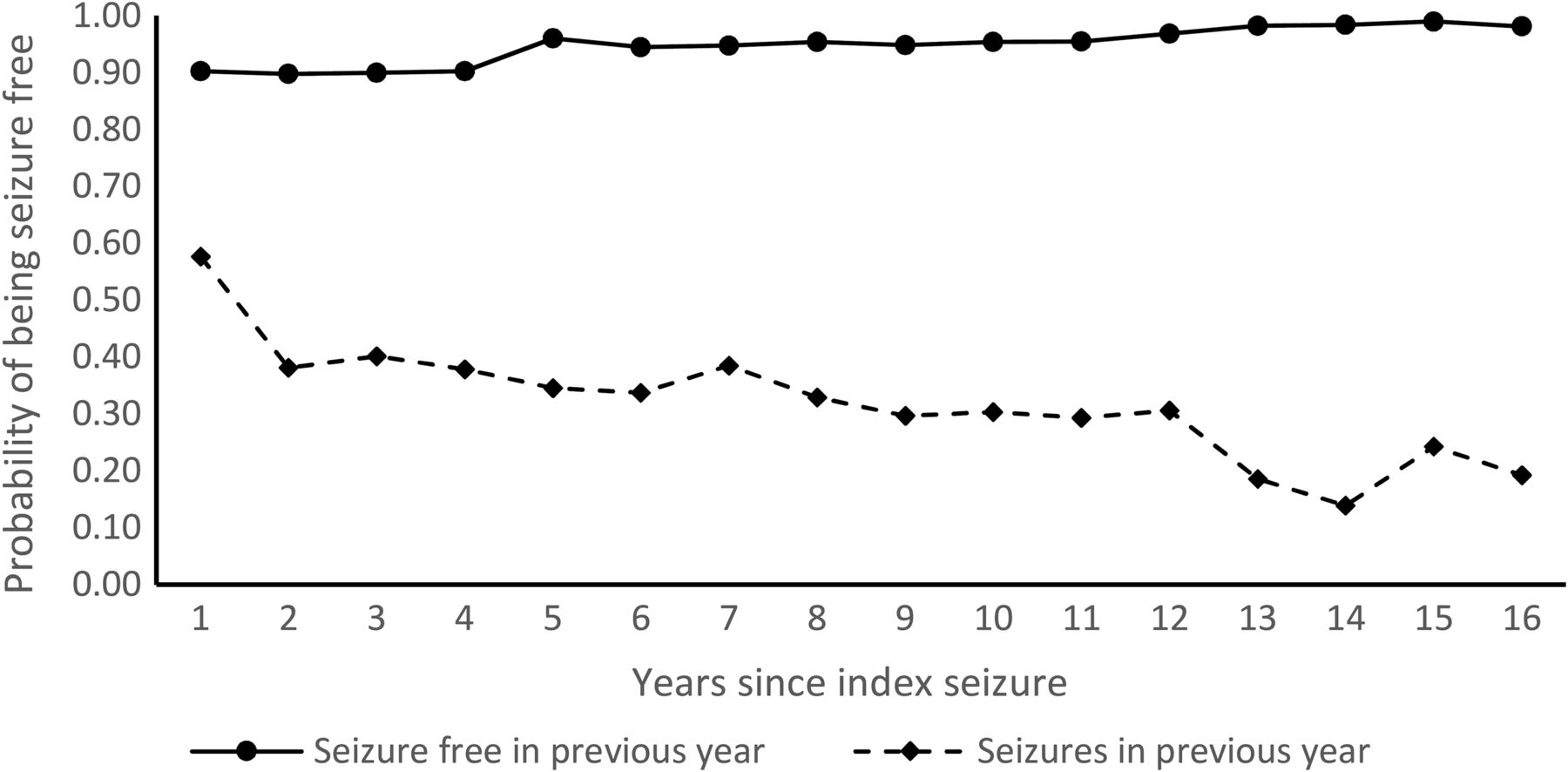
In those with no missing data, 49% (298/606) were seizure-free during the first year of follow-up. This increased to 74% by the second year, and was consistently over 80% by the sixth year of follow-up, although it was not always the same people who remained seizure-free. The proportion who were seizure-free 1 year and relapsed the following year was small (always <11%) but was never zero. Figure 2 shows the probability of being seizure-free in any year stratified on seizure status in the previous year.

Probability of seizure-freedom each year based on presence or absence of seizures in the previous year (N=568 with follow-up of at least 2 years).
Seizure outcome, stratified on seizure status in the previous 5 years at 5 and at 10 years is illustrated in figure 3.
{kind=link}
{kind=link}
{kind=link}
Seizure recurrence after 5 and 10 years stratified by seizure status in the previous 5 years.
Mortality
In the whole cohort (695 people) 255 died by October 2009 (SMR 2.07, 95% CI 1.83 to 2.34). The SMR was 2.65 (95% CI 2.23 to 3.15) in those with a single seizure at presentation and 1.67 (95% CI 1.40 to 1.99) in those with epilepsy at presentation. The SMR was higher in those with the index seizure in childhood (<18 years; SMR 5.34, 95% CI 3.32 to 8.59) than in those with onset later (SMR 1.98, 95% CI 1.75 to 2.25), although only 17 with childhood onset died (3.2 expected). Most (13/17) died as adults.
In those with a single seizure at presentation and with at least 2 years of follow-up, 146 people had early remission (no reported seizures beyond the first year of follow-up; SMR 1.86; 95% CI 1.40 to 2.46). In those with epilepsy at presentation, 145 people had early remission (SMR 1.44; 95% CI 1.06 to 1.95). The SMR in 112 people with a single notified seizure ever and with >1 year follow-up was 1.57 (95% CI 1.15 to 2.13) (1.62 in males and 1.53 in females). Most (91/112; 81%, 95% CI 73% to 87%) had at >10 years of follow-up. The SMR in 558 people with more than one notified seizure (before or after the index seizure) was 1.99 (95% CI 1.73 to 2.30).
Presumed aetiology
The main analyses were repeated for those with idiopathic/cryptogenic seizures (N=513) and those with remote symptomatic seizures (N=144) (table 5). Overall the group with symptomatic epilepsy fared worse, with bigger differences for 5-year terminal remission and mortality.
Seizure recurrence, remission, and mortality in people with cryptogenic/idiopathic seizures and those with symptomatic seizures
Sensitivity analyses
The online supplementary table shows the results of two sensitivity analyses. We found no evidence of difference between the current cohort and the original cohort (including people with acute symptomatic seizures), with overlapping CIs throughout. Comparison of the current cohort with only those with definite unprovoked epileptic seizures showed largely similar results but those with definite epilepsy were slightly more likely to have recurrent seizures and slightly less likely to have early 5-year remission.
Discussion
The NGPSE is a pragmatic, observational study set up in the 1980s, following an unselected cohort of people of all ages with newly diagnosed seizures of any type, to establish the long-term prognosis. For this analysis we excluded people with acute symptomatic seizures, and have separately investigated those with a single seizure and those with epilepsy at presentation. Two-thirds of people had >1 seizure recurrence after the index seizure; this was slightly more likely in people with epilepsy at presentation. We found high rates of seizure remission with slightly higher rates in those with a single seizure at presentation. Overall almost one-third remained seizure-free after the index seizure while another one fifth entered terminal remission after initial seizures (table 4). The probability of becoming seizure-free becomes more remote the longer seizures persist. The proportion of people who become seizure-free and then subsequently relapse is small (probability of relapse in the subsequent 10 years was 0.14 in those seizure-free in the first 5 years and 0.08 in those seizure-free in the second 5 years). In 327 people with follow-up to 2009, 268 (82%, 95% CI 77% to 86%) were in terminal remission, and 204 (62% of those with follow-up) were also off AEDs. Premature mortality is, however, higher than in the general population in all subgroups including those with a single reported seizure.
This study's strengths include long-term prospective follow-up of an unselected population-based cohort. Its weaknesses are inherent to its design. During a long-term, observational study it is inevitable that some people are lost to follow-up, either briefly or until the study end. Survival analysis assumes that any right censoring (loss to follow-up) is independent of survival, but those who were not followed-up may be in some way different. Our information came via GPs, and during this long study some GPs changed; the new GPs may not be as interested in epilepsy or the study. Some individuals may not have notified their GP of all seizures, or they may not have been recorded in the medical records; this applies to all seizure studies without direct observation. Doubtless with newer imaging techniques, many in the idiopathic/cryptogenic groups would be reclassified as having lesions; nevertheless, it is not possible to have 25-year follow-up in 2015 on people investigated using modern techniques. It is possible that use of the ‘operational’ clinical definition of epilepsy would reclassify some currently classified as having single seizures as having epilepsy.13 As we demonstrated little prognostic difference between those with epilepsy and those with a single seizure at presentation, it is unclear how this would have affected our results. GPs continued with their usual practice; the study team had no influence over medical care or any investigations performed.
The number of seizures prior to the index seizure was predictive of the probability of seizure recurrence after the index seizure, but the presence of seizures in the first 5 years after the index seizure seems more important in seizure prognosis. In the same cohort, it was previously shown that the number of seizures during the first 6 months after presentation was the most important predictor of remission.8
Apart from the NGPSE, there are only two other population-based studies with a longitudinal cohort larger than 250 participants, only one of which one has follow-up for >10 years.2 ,14 ,15 The percentages of people in terminal remission in previously reported studies range between about 44 and 70.2–5 ,16 Earlier analysis of the NGPSE, also excluding people with acute symptomatic seizures and excluding those with a single seizure at presentation found that 60% (95% CI 52% to 68%) had had a 5-year remission (not necessarily terminal remission) by 9 years.17 We found higher figures (80% in 5-year terminal remission in people with epilepsy at presentation followed to 2009). This may be influenced by the long follow-up in this study, with the proportion seizure-free each year consistently greater than 80% after 6 years. This finding of higher proportions in terminal remission associated with longer follow-up was previously suggested in two smaller cohort studies.2 ,18 The high proportion with terminal remission seen in the NGPSE is not entirely explained by the inclusion of people with single seizures at presentation (table 3); 73% of those with more than one seizure at presentation were in terminal remission by the end of follow-up (80% in those with complete follow-up). This higher rate of seizure remission may also be related to the community-based nature of the cohort, and may approximate to the ‘true’ population rate.
It is well recognised, through prospective cohort studies, that people with epilepsy are at increased risk of premature mortality, with this risk present at seizure onset and subsequently decreasing (but persisting) over time; this risk varies with underlying aetiology.19 In the NGPSE cohort we have previously demonstrated that the risk of premature mortality is increased throughout prolonged follow-up.9 We have now shown that the SMR is also significantly raised in people with early remission and in people with only a single notified unprovoked seizure. The SMR was increased in each group, including in those with idiopathic/cryptogenic seizures. Thus, prognosis for survival is not good, even among those whose seizures have ceased; the reasons for this are unknown. An early study from the US found the SMR to be 2.3 in 159 people with a single seizure.14 In other studies reporting survival after an isolated seizure, it is unclear how many remained seizure-free.20 ,21
The reasons for higher mortality in those presenting with a single seizure than in those with epilepsy are unknown, and indeed the finding seems counterintuitive. More people in the single seizure group had symptomatic aetiology (24%) than the epilepsy group (20%), and people in the single seizure group died earlier (table 1). While the overall disparity in mortality rates between the two groups may be partially explained by the higher proportion with symptomatic aetiology in the single seizure group, it does not explain why those with symptomatic aetiology in those with single seizures at presentation have a higher SMR (4.1) than those with symptomatic aetiology in those with epilepsy at presentation (SMR 2.6) (table 5). People with an idiopathic/cryptogenic aetiology in those with single seizures at presentation had a similarly higher SMR (1.9) than those with epilepsy at presentation (SMR 1.2) although the disparity is less marked. It is possible that some people originally classified as having a single unprovoked seizure had, in fact, had a provoked seizure which was not recognised. The cause of the provoked seizure may have been lifestyle habits (such as alcohol abuse, or alcohol or drug withdrawal)22 which could contribute to premature mortality. Alternatively, presenting after a single seizure might be a surrogate for seizure severity. The higher mortality rate in those with single seizures could, conversely, influence the probability of seizure recurrence as those who have died are not at risk of a further seizure. Using competing risks analysis for the main analyses (data not shown), however, found the differences between those with a single seizure and those with epilepsy at presentation marginally increased, but CIs overlapped throughout.
People with epilepsy have a higher rate of a variety of comorbidities than the general population.23 Some of these comorbidities may be a determinant of premature mortality.24 Our results suggest that these comorbidities may indeed constitute a major factor in premature mortality, particularly in people in long-term remission. This needs thorough investigation to allow for preventative strategies.
One of the key features of the current analysis was the dichotomisation of the original cohort into people with a single unprovoked seizure and people with epilepsy at the time of presentation to the study. This allowed for accurate depiction of the long-term seizure and mortality prognosis of people presenting with a single unprovoked seizure, which few studies have addressed.25 We can now say that the probability of remaining seizure free after 5 years is 37–49% in those presenting with a single unprovoked seizure; this is similar to the 48–58% found in the MESS study26 and to the 40–47% of people who entered 5-year remission with in 3 months of a first seizure in the FIRST study.27 More encouragingly the prognosis is far better in those who still have only had a single seizure at 5 and 10 years with only 17% and 8% probability of having a further seizure by the end of follow-up. This is of great prognostic value for clinicians counselling anxious people presenting with a single unprovoked seizure.
We have also shown that seizure prognosis (risk of seizure recurrence) in those with a single seizure at presentation is significantly, but only marginally, better than for those with >1 seizure at presentation. This fact has previously been commented on by several authors (eg, Berg28) but as described above, this picture is less clear when analysing mortality outcomes. By 25 years of follow-up the probability of having had no further seizures was only 0.36 in those with a single seizure, compared with 0.29 in those with epilepsy at presentation.
We excluded people with acute symptomatic seizures in the main analyses to make the results more comparable with other studies. Nevertheless, the results are similar when people with acute symptomatic seizures are included.
The NGPSE is probably one of the last large cohort studies of people with epilepsy where inclusion is determined by the presenting symptom. The perception of epilepsy as a homogeneous entity is being replaced by the concept of it being a collection of genetic and acquired conditions with a propensity to have unprovoked seizures. Consequently future cohort studies in people with epilepsy are likely to be smaller, determined by aetiology (eg, a genetic variant), which will allow for greater prognostic accuracy (in terms of both seizure control and survival) of people with the individual epileptic syndromes.
Acknowledgments
The NGPSE was adopted onto the NIHR CRN portfolio and financial support and logistical assistance was provided by the NIHR CRN and PCRN for this stage of the project which we gratefully acknowledge. JLP acknowledges support from the NIHR Biomedical Research Centre at Guys’ and St Thomas’ NHS Foundation Trust and King's College London, UK. We wish to acknowledge the contributions of previous members of the study team: Malcolm Taylor; Ewan Ross; Yvonne Hart; Charles Cockerell; Mark Manford; Samden Lhatoo and Bridget MacDonald. We would also like to thank all those individuals who participated and all the GPs who helped with the NGPSE throughout the years. We also wish to thank all the regional PCRN coordinators who helped raise awareness and promote the final follow-up stage of the NGPSE.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figure
- Data supplement 3 - Online table
Footnotes
Contributors The original study was conceived by SDS and DMGG. The most recent follow-up was led by JWS, AN and GSB. Data were collected by AN, aided by GSB, DMGG, CG, and JN. Analysis was performed by GSB with advice from ALJ and JLP. Intellectual input to the analysis was provided by MRK. AN and GSB drafted the paper and MRK and JWS provided further input to the draft. All authors approved the final version. JWS is the guarantor.
Funding This work was funded by the Brain Research Trust, the National Society for Epilepsy (now Epilepsy Society), British Epilepsy Association (now Epilepsy Action); National Fund for Research into Crippling Disease (now Action Medical Research). This work was carried out at University College London Hospitals/University College London Comprehensive Biomedical Research Centre, which receives partial funding from the UK Department of Health's NIHR Biomedical Research Centres funding scheme. JWS is supported by the Marvin Weil Epilepsy Research Fund.
Competing interests All authors have completed the Unified Competing Interests form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that: JWS has been consulted by and his department has received fees for lectures and research grants from Eisai, GlaxoSmithKline, and UCB and has received speaker's honorarium from Lundbeck and Teva. SDS has received speaker’s honorarium or is an advisory board member for UCB, GSK, Viropharma, Sage, Sanofi, Eisai. GSB's family has shares in GSK and her husband worked for GSK. MRK has received honoraria from UCB for educational lectures given to trainees. AN has received a speaker honorarium and travel bursary from Eisai. JN has received speaker honoraria and travel bursary from Pfizer and UCB. CG, DMGG, ALJ and JLP have no conflicts of interest.
Ethics approval The National Research Ethics Committee approved the on-going follow-up of the cohort in November 2007 (REC Reference 07/H0720/160), as did the National Information Governance Board Ethics and Confidentiality Committee (PIAG 1-05(g)/2008 NGPSE) granting Section 251 support.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No consent for data sharing with other parties was obtained, but the corresponding author may be contacted to request a limited amount of anonymised data