Article Text

Abstract
Parkinson's disease, dementia with Lewy bodies and multiple system atrophy are characterised by abnormal neuroglial α-synuclein accumulation. These α-synucleinopathies have in common parkinsonism and non-motor features including orthostatic hypotension (OH) and cognitive impairment. However, the nature of the relationship between OH and cognitive impairment is unclear. We therefore systematically reviewed the literature for evidence of an association between OH and cognitive impairment in α-synucleinopathies and discuss possible mechanisms and implications of this relationship. Abstracts from 313 original research articles were surveyed, and a total of 132 articles were considered for this review. Articles were stratified as: ‘direct-evidence studies’ based on the direct assessment for a relationship between OH and cognitive impairment in α-synucleinopathies, and ‘indirect-evidence studies’ based on an association being referred to as a secondary outcome. Ten ‘direct-evidence papers’ were identified, seven of which reported a positive association between OH and cognitive impairment, while seven of 12 ‘indirect-evidence papers’ similarly did as well. The papers that reported no association between OH and cognitive impairment used less sensitive measures of cognition. A relationship between OH and cognitive impairment in patients with α-synucleinopathies exists, but the underlying mechanisms remain unclear. Three hypotheses are proposed: (1) OH and cognitive impairment occur concurrently due to diffuse brain and peripheral deposition of α-synuclein, (2) OH-mediated cerebral hypoperfusion impairs cognition and (3) the two act synergistically to accelerate cognitive decline. Longitudinal neuroimaging studies and clinical trials may help clarify the nature of this relationship.
- PARKINSON'S DISEASE
- COGNITION
- AUTONOMIC
- LEWY BODY
- MULTISYSTEM ATROPHY
Statistics from Altmetric.com
Introduction
Parkinson's disease (PD), dementia with Lewy bodies (DLB) and multiple system atrophy (MSA) are neurodegenerative disorders characterised by the pathological accumulation of intracellular α-synuclein. In PD and DLB, α-synuclein aggregates in the neuronal cytoplasm and axonal processes into Lewy bodies and Lewy neurites, respectively.1 In MSA, α-synuclein aggregates in glial cells, especially within the cytoplasm of oligodendroglia.2 The parkinsonian motor syndrome of akinetic-rigidity, gait dysfunction and postural instability is most common not only in idiopathic PD, but it also occurs in DLB and the parkinsonian subtype of MSA.
With improvements in the management of motor symptoms in recent decades, non-motor features of these α-synucleinopathies are now a major cause of morbidity, including cognitive, neuropsychiatric, autonomic and sleep disorders.3–5 Two of the most prevalent and disabling non-motor features are orthostatic hypotension (OH) and cognitive impairment, which are often prominent early in MSA and DLB, respectively,6 whereas they typically predominate later in PD. Such non-motor symptoms contribute substantially to morbidity and mortality,7 increase healthcare utilisation and prolong hospitalisations.8–10 They have a negative impact on quality of life11 and account for considerable suffering by patients and caregivers. Non-motor features are often poorly recognised and evaluated by healthcare providers,12 and currently are among the most pressing unmet therapeutic needs in PD.13
Autonomic dysfunction includes genitourinary, gastrointestinal, respiratory, sweating and cardiovascular abnormalities. Although dysautonomia is more severe in MSA than PD or DLB,14 it is present in all three α-synucleinopathies,6 ,15 with OH being a common manifestation. OH is also a key symptom in pure autonomic failure (PAF), a syndrome characterised pathologically by α-synuclein-mediated neuronal degeneration of the peripheral autonomic nervous system with preservation of the central nervous system, and thus no additional neurological symptoms or signs such as parkinsonism or dementia are present.16
Symptoms of OH have been reported in 81% of MSA patients, 28–31% of DLB patients and 18–30% of PD patients.17–19 It is important to note, however, that classical symptoms of OH (ie, postural light-headedness) may be absent in PD patients who have objective postural drops in blood pressure (BP), and thus OH is under-recognised and under-reported.20 This may relate to either cognitive impairment confounding the ability of patients to report symptoms or to the reduced threshold in mean arterial pressure above which patients may not experience symptoms of OH in α-synucleinopathies.21
Cognitive impairment in α-synucleinopathies is most prevalent and earliest by definition in DLB since it is an essential criterion for the clinical diagnosis.22 In contrast, in PD, about 25% of the patients have mild cognitive impairment (MCI) early23 ,24 with dementia reaching ∼80% in the second decade of the illness.25 ,26 Although cognitive impairment was for many years considered to be uncommon in MSA, growing evidence suggests that this is not the case.27 Neuropsychological testing reveals a similar pattern of attention, visuospatial and frontosubcortical-mediated executive dysfunction occurring in PD dementia (PDD), DLB and MSA.27–29
While OH and cognitive impairment are often considered discrete clinical entities that commonly occur along the spectrum of α-synucleinopathies, there is increasing evidence of a link between them in neurodegenerative and other, non-neurodegenerative, cohorts. OH may cause mood and cognitive changes across the lifespan.30 For example, OH is correlated with cognitive impairment irrespective of age and education level in geriatric patients,31 while even in younger patients, execution time on cognitive testing is slower in hypotensive compared to normotensive counterparts.32 Impaired systolic BP regulation in response to standing in children was associated with poor effort in school—possibly related to altered release of activating neurotransmitters or cerebral hypoperfusion.33 In patients with non-insulin-dependent diabetes mellitus, impairment of serial list learning and reaction time was correlated with the fall in systolic BP on standing.34 Patients with any type of dementia were more likely to have OH than healthy adults.35 Dysautonomia commonly occurs in patients with dementia and is more common in DLB and PD than in patients with Alzheimer's disease or frontotemporal dementia.36 In PD, Allcock et al37 first showed that patients with OH had more impairment in sustained attention and visual episodic memory than patients without OH. Despite this evidence, the relationship between OH and cognitive impairment in different diseases, including α-synucleinopathies, has remained controversial,38 and the mechanisms of the association are unclear.39 Previous evaluations of the relationship between OH and cognitive impairment in patients with movement disorders did not account for the degree to which cognition was tested in each source study. Therefore, a more focused and detailed review of the literature relating to this relationship in α-synucleinopathies is warranted taking into consideration domain-specific cognitive impairment.
In this systematic review of the evidence for and against an association between OH and cognitive impairment in α-synucleinopathies, we have also sought to discuss the mechanisms that may underlie this relationship. OH may contribute to cognitive impairment by causing repeated episodes of cerebral hypoperfusion with a resultant acceleration in the clinical course. Alternatively, OH and cognitive impairment may be caused independently by the diffuse neuropathology underlying severe phenotypes of α-synucleinopathies. A third possibility is that OH and cognitive impairment arise from an interaction between diffuse brain/peripheral α-synuclein and cerebral hypoperfusion.
Orthostatic hypotension and cognitive impairment in α-synucleinopathies: a systematic review
Search strategy and results
Using the search strategy detailed in figure 1, 313 article abstracts were reviewed for relevance by the first author (SJU). Articles were included as ‘direct-evidence studies’ if they were designed to assess the relationship of OH and cognitive impairment in one of the α-synucleinopathies. Articles were included as ‘indirect-evidence studies’ if they added information about the clinical, mechanistic or indirect association between OH and cognitive impairment in α-synucleinopathies, but were designed with a different objective.

A flow chart depicting the search strategy and process of inclusion and exclusion of papers in the systematic review.
Ten out of 132 articles considered were deemed ‘direct-evidence studies’ (table 1), and 12 out of the 132 articles were considered ‘indirect-evidence studies’ (table 2). There was marked heterogeneity between studies including use of diverse patient populations, how OH was quantified, how cognition was evaluated and in the outcome measures used (see online supplementary tables S1 and S2). Characterisation of OH varied in terms of the type of orthostatic test (ie, tilt table or orthostatic BP), the timing of BP measurements and the definition of OH. Cognition was assessed subjectively by questionnaire and/or objectively by screening tests such as the mini-mental state examination (MMSE) and/or domain-specific neuropsychological testing.
Direct-evidence studies on the association between OH and cognitive impairment
Indirect-evidence studies on the association between orthostatic hypotension and cognitive impairment
supplementary table
A Summary of the Direct Evidence Papers Reporting on the Association between Orthostatic Hypotension and Cognitive Impairment in Alpha-Synucleinopathies
supplementary table
A Summary of the Indirect Evidence Studies Reporting on the Association between Orthostatic Hypotension and Cognitive Impairment in Alpha-Synucleinopathies
All 10 of the direct-evidence studies involved only PD patients. Nine were cross-sectional studies, and one was a longitudinal, prospective study. Half of them were small studies, with <30 patients per group. A positive association between OH and cognitive impairment was reported in 7 of the 10 papers (including the longitudinal study), where PD patients with OH were more likely to have cognitive impairment. Cognitive domains that were particularly sensitive to this relationship included attentional/executive and visuospatial functions that are characteristic of PD-related cognitive decline.
Of the 12 indirect-evidence studies, 5 included PD patients, 3 included DLB patients, 1 included PD and DLB patients, and 3 included MSA patients. Eight were cross-sectional studies, three were prospective studies and one was a retrospective chart review. A positive association between OH and cognitive impairment in these patient populations was described in 7 out of the 12 papers (including 2 of the 3 prospective studies). None of the 22 studies showed the reverse of this association, where patients without OH had worse cognitive deficits.
Robust direct-evidence of the association between OH and cognitive impairment was shown in a prospective study of 80 cognitively intact PD patients. The risk of developing dementia over a mean follow-up of 4.4 years was increased by 84% per 10 mm Hg drop in systolic BP.45 In the MSA population, cardiovascular dysautonomia was independently associated with cognitive impairment in 372 MSA patients.59 In another MSA study, patients with OH scored lower on an executive function task than patients without OH and had delayed novelty P3 somatosensory responses, suggesting that OH is associated with frontal lobe dysfunction.49
Orthostatic hypotension is associated with subtle, domain-specific cognitive deficits
OH was associated with domain-specific cognitive impairment in four of the direct-evidence studies. Although MMSE scores were similar between PD patients with and without OH, those with OH performed worse on tests of sustained attention and visuospatial function37 ,44 as well as verbal episodic memory.43 ,44 A correlation between the extent of orthostatic BP drop and lower attention scores was found in PDD, but not in PD without dementia.40 The cognitive profile observed in these four studies was typical of that seen in PD.28
Indeed, several of the studies that did not confirm a relationship between OH and cognitive impairment in α-synucleinopathies used relatively insensitive measurements of cognition, specifically with respect to executive dysfunction, the most common domain affected in PD. In particular, three of these studies only evaluated MMSE,47 ,48 ,52 which is relatively insensitive to cognitive impairment in PD.S61
Arahata et al50 evaluated brain metabolism using 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) and identified that PD patients with OH had regional hypometabolism involving the occipital, inferior parietal and superior parietal cortices compared to those without OH; however, both groups had similarly normal performance on the Hasegawa Dementia Scale (HDS) or HDS-Revised (HDS-R). The HDS-R is sensitive to Alzheimer's disease, but it does not sufficiently assess executive functions.S62 It is plausible that this typical FDG-PET signature of PDD, DLB and PD patients with OH may be validated as an imaging biomarker of future dementia. Together, these results suggest that comprehensive neuropsychological assessment is necessary to detect the changes in cognition that are associated with OH.
Cognitive impairment in α-synucleinopathies is heterogeneous and likely caused by multiple pathophysiological mechanisms including cortical and subcortical neurodegeneration due to Lewy body formation that results in dysfunction of dopaminergic, noradrenergic and cholinergic neurotransmitter systems.28 However, based on the results of our systematic review, we have identified a robust association between OH and cognitive impairment in α-synucleinopathies that may also be playing a contributory role. We propose two alternative explanations of this association (figure 2). First, the coexistence of OH and cognitive impairment may be a marker of diffuse neuropathological involvement reflecting parallel neurodegeneration of regions responsible for cardiovascular autonomic control and cognition.36 S63 Alternatively, OH on its own or together with supine hypertension (SH) may have a negative prognostic impact on cognition in α-synucleinopathies, where the combination of cerebral hypoperfusion, with or without small vessel disease, contributes in part to cognitive dysfunction.S64
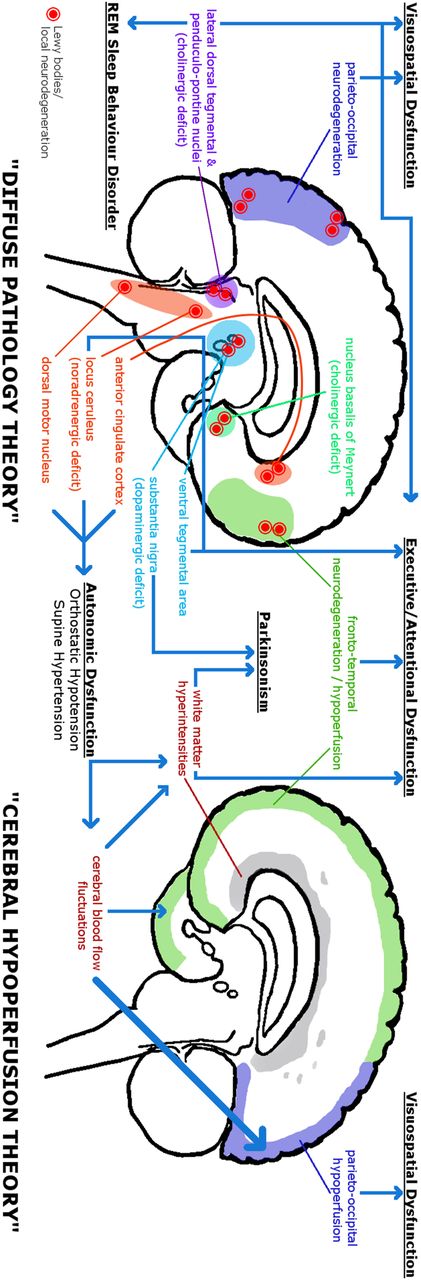
A graphical representation of two possible theories that explain the relationship between OH and cognitive impairment in α-synucleinopathies. In the ‘Diffuse Neuropathology Theory’, diffuse Lewy body deposition and neurodegeneration in multiple brain areas lead to autonomic dysfunction and cognitive impairment. Lewy body deposition and neuropathology in the substantia nigra lead to the striatal dopamine deficit that causes parkinsonism. The combination of frontal neurodegeneration and a frontostriatal dopaminergic deficit from pathology in the ventral tegmental area contributes to executive and attentional dysfunction. Parieto-occipital neurodegeneration and cholinergic deficit due to pathology in the lateral dorsal tegmental and pedunculopontine nuclei as well as in the basal forebrain contribute to visuospatial dysfunction and visual hallucinations, and the cholinergic deficit contributes to executive and attentional dysfunction as well. Neuropathology affecting the anterior cingulate cortex, locus ceruleus and dorsal motor nucleus contributes to OH and SH. Noradrenergic deficit due to locus ceruleus pathology contributes to executive-attentional dysfunction. In the ‘Cerebral Hypoperfusion Theory’, the combination of OH and SH likely contributes to the development of WMH, due to neuropathological protein accumulation and/or vasculopathy, which contribute to parkinsonism and to the development of cognitive impairment, specifically that related to frontal lobe dysfunction. Furthermore, OH causes CBF fluctuations which may worsen cognitive impairment transiently, with deficits potentially accruing over time. The posterior circulation, and thus the parieto-occipital areas, is more susceptible to OH-mediated hypoperfusion. It is likely that both of these processes—diffuse neuropathology and cerebral hypoperfusion—are not exclusionary, and each contributes to the worsening of cognitive impairment in patients with α-synucleinopathies and OH. CBF, cerebral blood flow; OH, orthostatic hypotension; SH, supine hypertension; WMH, white matter hyperintensities.
Cerebral hypoperfusion theory
OH occurs following a redistribution of blood volume into the lower limb and splanchnic organs on standing. This redistribution lowers venous return and cardiac filling pressure, and leads to reduced stroke volume and cardiac output.S65 Cerebral hypoperfusion, associated with reduced cardiac output, is believed to contribute to symptomatic OH, including light-headedness, fatigue, blurred vision, presyncope and even syncope. This transient cerebral hypoperfusion and/or repeated bouts of it may mediate the association between OH and cognitive impairment in patients with α-synucleinopathies.
Some insight into the relationship between OH and cognitive impairment can be gained from reviewing the different pathophysiological mechanisms of OH. In PAF, for example, OH arises from neurodegeneration of the peripheral nervous system,16 S66 and autonomic innervation of the skin is reduced in PAF compared to MSA, in which central neurodegeneration accounts for autonomic failure.S67 These observations intimate that OH in PAF is due to peripheral pathology, while OH in MSA is due to central pathology.S68 Although cognitive impairment is not traditionally seen in PAF, neuropsychological testing revealed deficits of attention and executive function in PAF patients similar to patients with ‘central’ α-synucleinopathies.S69 Furthermore, patients with PAF had displayed impairment of executive function during orthostatic testing.S70 These cognitive deficits are likely due to cerebral hypoperfusion since these patients have no central neurodegeneration.
Fluctuations in cerebral perfusion
One characteristic of cognitive impairment in patients with PDD and DLB is the profound fluctuations in alertness and attention.28 ,29 Transient episodes of cerebral hypoperfusion may contribute to these fluctuations. One direct-evidence study showed that in PDD, performance on attention-related tasks was worse during an episode of OH precipitated by head-up tilt.40 Autonomic and neuropsychiatric fluctuations, including hallucinations, were common in another PD cohort with motor fluctuations.S71 While OH was not measured in this cohort, this study suggests a possible relationship between autonomic dysfunction and transient changes in neuropsychiatric state. Furthermore, visual hallucinations in PD were associated with autonomic symptoms (including gastrointestinal, urinary, thermoregulatory and cardiovascular dysfunction) and also reduced cardiac metaiodobenzylguanidine uptake.57 S72 Finally, among geriatric patients with dementia and OH, 65.6% reported mental fluctuations, and these symptoms improved with the treatment of OH.S73
Cerebral autoregulation is a cerebrovascular mechanism that in good health can compensate for hypotension by maintaining cerebral blood flow (CBF) over a wide range of perfusion pressures. However, there is evidence that this process may break down in α-synucleinopathies. Near-infrared spectroscopy (NIRS) and transcranial Doppler ultrasound (TCD) are methods of tracking transient changes in cerebral oxygenation and blood flow velocity, respectively. In patients with PAF or MSA, BP reduction during head-up tilt was associated with reduced cerebral oxygenation measured by NIRS.S74 In PD, a mean standing arterial BP under 75 mm Hg was highly sensitive and specific for detecting patients with symptomatic OH, whereas only 50% of the patients who had a drop of either 20 mm Hg in systolic BP or 10 mm Hg in diastolic BP were symptomatic.20 This may indicate that a mean arterial pressure of under 75 mm Hg is likely below the lower threshold for cerebral autoregulation of blood flow in patients with α-synucleinopathies. On the other hand, TCD studies have shown that cerebral autoregulation adequately compensates for mild OH in MSAS75 and PD.S76 Therefore, the lower limit for cerebrovascular autoregulation might be reduced to compensate for chronic OH in α-synucleinopathies.21 In patients with more extreme orthostatic BP drops, however, CBF velocity decreases and patients became presyncopal, suggesting that BP had fallen below the limit of autoregulation.S76
Chronic OH may also accelerate neurodegenerative processes. In rats, chronic cerebral hypoperfusion induced by carotid ligation has been shown to induce proteasome dysfunction and the aggregation of ubiquinated proteins.S77 In the autopsied brains of PD patients with OH, there was a preponderance of ß-amyloid deposition in cortical regions susceptible to hypoxic-ischemic injury such as at the boundary zones between the anterior and middle cerebral arteries or middle and posterior cerebral arteries.S78
Little evidence is available comparing differences in resting CBF in patients with and without OH. Matsui et alS79 reported hypoperfusion in the bilateral anterior cingulate gyri in patients with OH using single photon emission CT. They argued that dysfunction of the anterior cingulate, which has higher order influences on autonomic regulation, contributed to OH. The cross-sectional nature of their study, however, precluded any causative inference. A proof-of-concept study was recently published after the time of our review process. This study provides direct evidence that cerebral hypoperfusion is related to OH in α-synucleinopathies.S80 CBF was measured by arterial spin labelling (ASL) MRI in 15 patients with α-synucleinopathies (7 DLB, 5 PDD and 3 PD-MCI) and 15 patients with small vessel disease matched for age, sex and education. In the α-synucleinopathy group, OH was associated with lower occipitoparietal CBF, which in turn was associated with impairment on visuospatial and attentional tasks even after controlling for severity of general cognitive function. This study provided the first and most compelling evidence that regional hypoperfusion is proportional to the severity of OH, and that CBF in these regions is associated with domain-specific cognitive impairment.
Cerebral small vessel disease: assessment of white matter hyperintensities using MRI
Chronic OH and SH may also contribute to cerebrovascular pathology in α-synucleinopathies by increasing the risk of cerebral small vessel disease, which has been well documented in contributing to non-α-synuclein-related dementia.S81 S82 White matter hyperintensities (WMH) are lesions visible as T2 hyperintense regions seen on MRI scans that may have a heterogeneous pathology. Most commonly, these are due to leukoaraiosis but may be seen due to venous collagenosis or cerebral amyloid angiopathy (coexistent with α-synuclein or tau pathology). Increased burden of WMH was associated with more severe parkinsonism in PD patients,S83 although the entity vascular parkinsonism is controversial,S84 and WMH burden may also contribute to cognitive deficits.S85 There is evidence that OH is associated with WMH in α-synucleinopathies, which may partially explain the relationship between OH and cognitive impairment. Kim et al46 showed that cognitive impairment is not only associated with OH in early-stage PD, but it is also associated with the combination of OH, SH and increased WMH. In DLB patients, the severity of the drop in systolic BP in response to carotid sinus massage was correlated with the severity of WMH.S86 S87 In PD patients, a higher drop in BP during postural testing was correlated with increasing WMH scores.S88 In patients with MSA, the presence of OH was independently correlated with WMH burden.S89 Furthermore, in patients with early, untreated PD, OH was associated with increased intimal–medial thickness and wall:lumen ratio on neurocirculatory and carotid sonographic measurements.S90 This combination of arteriosclerosis and OH may contribute to microvascular injury and cognitive impairment in PD patients.
Supine hypertension
OH is often accompanied by SH in chronic autonomic failure including PD, MSA and PAF.S91 S92 The mechanisms underlying this relationship are poorly understood but may be due to denervation supersensitivity of adrenergic receptors, alterations in baroreceptor reflex gain, increased blood volume and/or arterial stiffness.S93 Furthermore, treatment of OH with BP-enhancing agents can aggravate SH.S93 One direct-evidence study found that cognitive impairment was associated with OH, SH and WMH in 87 PD patients, and all 13 patients with OH and SH had MCI or dementia.46 The strong association of SH with OH in this cohort made it impossible to determine the separate contributions of OH and SH to cognitive impairment. However, there is evidence to suggest that SH contributes to cognitive impairment over and above OH. SH was found to contribute to cognitive impairment in adults without α-synucleinopathies, and together, OH and SH were associated with lower global and executive cognitive performance than in those with OH alone.S94 A recent study published after our literature search showed that SH was associated with the akinetic-rigid motor subtype of PD and also with lower MMSE scores, whereas OH was not associated with lower MMSE scores,S95 but this finding has not been shown in other studies. On the other hand, SH did not contribute to the cognitive impairment associated with OH in PD in one direct-evidence study. Of 23 patients with OH, 9 had SH, and there were no differences in neuropsychological test scores in OH patients with or without SH.44 There was also no difference of SH frequency in non-demented PD compared to PDD with similar disease stage, gender and age.S96 Chronic SH is a risk factor for stroke in the elderly, is associated with cardiovascular comorbidity in PD patientsS96 S97 and is also associated with WMH. It is possible that lowered cerebral autoregulatory thresholds to compensate for chronic OH lead to increased susceptibility of the brain to vascular lesions caused by SH.21 The consequence of SH in patients with α-synucleinopathies remains unclear as most of the evidence suggesting that SH is harmful is derived from non-α-synucleinopathy populations with chronic essential hypertension. Managing OH in the context of coexisting SH requires a careful balance and should be investigated in future prospective clinical trials.S92
Interestingly, in patients with PD-MCI, PDD and DLB, SH was associated with hyperperfusion of the frontal lobes,S80 which may predispose to frontal WMH. This same study found that OH was associated with hypoperfusion of the occipitoparietal regions, and in a separate longitudinal cohort of PD patients, posterior cortical dysfunction evidenced on neuropsychological tasks was associated with the risk of developing dementia.S98 This suggests that OH may lead to cognitive impairment by contributing to occipitoparietal hypoperfusion and early posterior cortical cognitive dysfunction, while SH may cause increased frontal WMH through hypertensive damage to small cerebral vessels—a dual-hit hypothesis.
Diffuse neuropathology theory
The diffuse neuropathology theory posits that the presence of OH and cognitive impairment may simply reflect α-synuclein-mediated neurodegeneration in diffuse areas of the brain and in the peripheral autonomic nervous system (figure 2). Whereas early autonomic dysfunction in α-synucleinopathies may arise from pathology in the peripheral autonomic nervous system,S99 there is also central control of cardiovascular autonomic function from brainstem, hypothalamic and cortical structures including the anterior cingulate and/or insular gyri.36 S63 S79 S100 Neurodegeneration of diencephalic and cortical structures is also directly implicated in dementia.
Among the studies reviewed, several supported the diffuse neuropathology theory. Compared to non-OH PD patients, those with OH had lower MMSE scores and more severe motor impairment, although this study did not compare age or disease duration between groups.42 In PD, symptoms of autonomic dysfunction were correlated not only with cognitive impairment but also with motor dysfunction, psychiatric complications, poor sleep and excessive daytime sleepiness.60 Another study showed prospectively that PDD and DLB patients who presented with persistent OH had a shorter survival time than those without OH independent of age, disease duration or vascular risk factors.52 These studies support the notion that neurodegeneration in multiple areas may underlie the association between OH and cognitive impairment.
OH and cognitive impairment are associated with the global motor severity of PD as rated by the Hoehn and Yahr stage.S101 Furthermore, patients with an older age of disease onset are more likely to have more severe motor symptoms, cognitive impairment and dysautonomia as well as other non-motor features such as impaired taste or anosmia, insomnia, hallucinations, intense vivid dreaming and acting out during dreams (likely due to rapid eye movement sleep behaviour disorder (RBD)).S102 Motor severity, autonomic dysfunction and cognitive impairment were also associated with older age of onset in a cohort of 624 PD patients.S103 Bulbar dysfunction and the presence of non-specific systemic, gastroenterological and urological disorders (suggesting autonomic dysfunction) predicted the development of dementia in a large PD cohort after 5 years of follow-up.S104 Bulbar dysfunction and dysautonomia, as predictors of dementia, suggest the pathological involvement of more extensive brain areas, including brainstem and cortical regions. In PD patients, autonomic symptoms were associated with psychosis,S105 depression, excessive daytime sleepiness, night-time sleep disturbance and more severe parkinsonism.60 In a cohort of nearly 400 PD patients, exploratory factor analysis identified that cognitive impairment, dysautonomia, depression, psychotic symptoms, daytime sleepiness and axial symptoms clustered together and reflected more advanced disease.S106 In 274 PD patients, a more severe disease phenotype was associated with higher risk of non-motor symptom burden.S107 These studies suggest that OH may cluster together with cognitive impairment and other non-motor features in patients with more severe PD without implying a causal relationship between them.
To assess a causal relationship between OH and cognitive impairment, one can examine specific at-risk states for α-synucleinopathy. For example, in a genetic study of families with parkinsonism and α-synuclein gene (SNCA) copy number variants, a higher number of SNCA multiplications (ie, higher SNCA dosage) was correlated with more severe and frequent parkinsonism, autonomic dysfunction and dementia.S108 SNCA multiplication causes overexpression of α-synuclein, which is proposed to lead to a more diffuse neuropathology.
Late-onset RBD is a ‘premotor’ manifestation of α-synucleinopathies,S109 S110 which is commonly reported years before the other typical symptoms of PD.S111 RBD is associated with cognitive impairment in PD patients.S112 S113 Compared to those without RBD, non-demented PD patients with RBD performed poorly on tests of verbal episodic memory, executive function and visuospatial and visuoperceptual processing.S114 RBD in PD is also associated with OHS115 and other measures of cardiac autonomic dysfunction such as beat-to-beat heart rate variability on electrocardiogram tracings.S116
The coexistence of RBD and OH in PD predicts the development of dementia55 and along with MCI portend a more severe ‘diffuse/malignant’ phenotype.58 Together, the association between RBD, OH and cognitive impairment might be interpreted as evidence of more extensive neuropathological involvement of diffuse brain structures. However, prodromal cardiovascular autonomic dysfunction may arise from peripheral rather than central pathology,S99 suggesting that OH does not arise from exclusively central nervous system pathology. Indeed, peripheral noradrenergic denervation is a major factor that predicts the development of OH in PD.S117 Furthermore, as suggested by Postuma et al, the pathophysiology of RBD and cardiac dysautonomia are not necessarily associated simply due to co-localised neuropathology.S118 If this is the case, OH may contribute to, rather than simply share in, the pathophysiology of dementia, in patients with α-synucleinopathies.
Clinical implications
There is sufficient evidence to acknowledge a strong relationship between OH and cognitive impairment in the three major α-synucleinopathies. While it is possible that these two clinical features are markers of a more severe α-synuclein phenotype, we propose that the effects of OH (and possibly SH) on CBF contribute in part to the development of cognitive impairment. The two hypotheses linking OH and cognitive impairment in α-synucleinopathies are not mutually exclusive (figure 3). As with all complex neurodegenerative diseases, mechanisms to cognitive impairment in α-synucleinopathies are multifactorial in nature, so the cerebral hypoperfusion and diffuse neuropathology theories may be operating in synergy with, and magnify, each other.

{kind=link}
{kind=link}
{kind=link}
A graphical representation of the synergistic effect caused by contributions from the ‘diffuse neuropathology theory’ and ‘cerebral hypoperfusion theory’. It is likely that the pathophysiologic mechanisms underlying each theory interact with each other, where diffuse neuropathology causes OH and cognitive impairment, OH contributes to cognitive impairment and OH contributes to worsening of neuropathology. Together, these mechanisms increase the rate and severity of disease progression. OH, orthostatic hypotension.
These neurodegenerative diseases share a motor syndrome, parkinsonism, with non-motor features including RBD, OH and cognitive impairment. The cognitive profile in these patients involves attention-executive and visuospatial deficits as the most prominent features, which are not well represented in the common cognitive screening test, MMSE. Several studies have shown that these domains themselves are more affected in patients with OH than those without. OH (perhaps with SH contributing in some cases), with impairments in cerebral vascular autoregulation, leads to cerebral hypoperfusion that may accelerate neurodegeneration, increase the burden of WMH and promote fluctuations in attention and alertness.
There are important clinical implications of the relationship between OH and cognitive impairment in α-synucleinopathies. First, it is important to assess OH clinically at an early stage. OH is not always symptomatic (eg, postural light-headedness), especially in demented patients, where up to 60% of the patients with objectively measured OH are asymptomatic.54 It is important as a bare minimum to measure lying and standing BPs during clinical visits. Additionally, we recommend that patients or their caregivers measure and record their own BP at home, after lying supine for 5 min and then again 3 min after standing, as single point of care measurements in the clinic may not reveal OH. Clear and explicit instructions are paramount to obtain reliable data. Other more involved measurements such as 24-hour BP monitoring or formal autonomic testing may be useful to detect OH for clinical and research endeavours, although, for 24-hour BP monitoring, sit to stand postural changes would need to be documented in some way.
The second implication surrounds treatment of OH. Aside from its effects on cognition, OH is detrimental to the quality of life of patients.S119 Treatment of OH has been shown to reduce mental fluctuations, excessive sleeping in chairs, falls, lethargy, fatigue and dizziness experienced by geriatric patients with dementia.S73 Current treatments of OH have a risk of exacerbation of (paroxysmal) SH and with this, the risk of accelerating small vessel cerebrovascular disease. The clinical and cognitive impact of this iatrogenic SH needs to be assessed in systematic studies, together with investigations into potential treatments for OH that are less likely to induce it.
Future directions
Future studies evaluating the relationship between OH and cognitive impairment in α-synucleinopathies are warranted, and we suggest that these studies control for confounding factors such as levodopa equivalent daily dose and cardiovascular risk factors, which are associated with autonomic and cognitive dysfunction. Given the results of our review and case report (see online supplementary material), early and sustained treatment of OH may have a role in slowing the progression and impact of cognitive impairment in patients with α-synucleinopathies. A randomised controlled clinical trial of anti-OH treatment would be helpful in testing this hypothesis, with the caveat of risks associated with SH from aggressive treatment of OH.
supplementary material
In the interim, we recommend systematic clinician inquiry and record keeping regarding cognitive impairment in all three diseases. In many clinics, cognitive symptoms and signs may be under-reported. For a rare disease like MSA, national and international collaborative registries can assist hypothesis generation and testing (eg, The UK MSA Research Network and Pan-American Consortium of Multiple System Atrophy (PANMSA)). These multicentre cohorts would provide large-scale and longitudinal natural history studies to a greater degree than the studies outlined in tables 1 and 2, if the cognitive screening tests used are appropriately sensitive to the domains affected by PD, MSA and DLB (eg, MoCA).S61 S120 This would also provide a platform for design and recruitment to clinical trials of symptomatic and disease-modifying treatments, including efforts to break a causal link between OH and cognitive impairment.
It is likely that the neuropathology of α-synucleinopathies is established in the brain many years before symptoms begin. Projects like the 500 000 strong UK BioBank of middle-aged ‘healthy adults’ with cognitive, imaging, genetic and cardiovascular markers therefore provide an opportunity to study the antecedents and co-evolution of OH and cognitive impairment in α-synucleinopathies as patients become symptomatic in the next 10 years.
We also recommend targeted neuroimaging investigations of cerebral vascular autoregulation, perfusion and WMH, to investigate the mechanisms through which OH and SH might modulate cognition in symptomatic α-synucleinopathies. In addition to providing for evidence of cerebral small vessel disease from structural neuroimaging techniques,S121 S122 functional neuroimaging may also be useful in elucidating the putative pathophysiological link between OH and cognitive impairment. Functional MRI (fMRI) using blood oxygen level-dependent (BOLD) contrast and ASL can non-invasively be used to estimate neuronal activity and vascular reactivity by measuring on transient changes in blood flow, volume and oxyhaemoglobin/deoxyhemoglobin ratios.S123 ASL MRI may be particularly useful to non-invasively measure tissue perfusion (ie, CBF).S124 Longitudinal changes in resting-state fMRI and ASL MRI measures in de novo cohorts of patients with α-synucleinopathies (eg, Parkinson's Progression Markers Initiative) who develop OH and cognitive impairment during their disease course will be critical, to control for confounding factors and estimate temporal precedence of OH and cognitive impairment on an individual patient level. It is anticipated that such studies may elucidate the neurophysiological basis of observed associations between these non-motor symptoms.
PET would also be helpful if ligands that bind selectively to α-synuclein are developed for human use, analogous to amyloid and tau ligands that have become available in the past decade.S125 S126 The in vivo estimation of regional α-synuclein pathology would enable one to separately estimate the anatomical pathologic correlates of cognitive impairment and OH, and estimate the causal relationships between them including mediating influences of WMH. However, no such α-synuclein ligands are currently licenced for human imaging.
Novel applications of functional neuroimaging techniques hold great promise in understanding the mechanistic basis of the association between OH and cognitive impairment in α-synucleinopathies. For example, a recent fMRI study showed that activation of the parasympathetic nervous system can negatively affect cognition and alter functional connectivity of related networks.S127 Another promising technique that uses resting-state fMRI to examine downstream effects of cardiac-related beat-by-beat pulsatility in cerebral white matter (termed physiological fluctuations in white matter) has shown dysfunction of normal appearing white matter in three patient cohorts: individuals with small vessel disease, MCI and Alzheimer's disease.S128 S129 These physiological fluctuations are hypothesised to precede the development of WMH on structural MRI and might be a more sensitive measure to investigate in determining the effects of OH and SH on vascular brain health in α-synucleinopathies. Such longitudinal assessments and correlation with brain autopsy studies would add significant insight into the relationship of OH and cognitive impairment in α-synucleinopathies.
Conclusion
OH and cognitive impairment are common, disabling non-motor features in patients with PD, DLB and MSA. OH may contribute to cognitive impairment in this population, although the underlying pathophysiological underpinnings await further clarification using longitudinal, multimodal neuroimaging and neuropathologic studies. Early diagnosis and treatment of OH may improve the prognosis of these patients with progressive and intractable neurodegenerative diseases; however, clinical trials with existing and novel therapeutic agents investigating this hypothesis are currently lacking and represent a major unmet clinical need. Despite the current absence of effective disease-modifying therapies for α-synucleinopathies, clinicians can capitalise on addressing readily treatable targets that otherwise magnify the disability and poor quality of life resulting from α-synucleinopathies.
supplementary References
Acknowledgments
SJU would like to thank Parkinson's Society Canada for supporting his clinical fellowship in Movement Disorders and the helpful librarians at the Gerstein Science Information Library at the University of Toronto. MM receives salary support from the Department of Medicine at Sunnybrook Health Sciences Centre and University of Toronto, and from the Sunnybrook Foundation.
References
Footnotes
Contributors SJU and MM involved in preparation of project conception. SJU involved in review execution. Graphic design was made by SJU and ADR. SJU prepared manuscript draft. Manuscript review and critique were performed by ADR, BJM, AJE, JBR, AEL and MM.
Funding This project was supported by a Clinical Fellowship award from Parkinson's Society Canada.
Competing interests SJU and ADR have nothing to disclose. BJM has received peer-reviewed research support from the Canadian Institutes of Health Research. AJE is supported by the NIH (1K23MH092735); has received grant support from Great Lakes Neurotechnologies and the Michael J Fox Foundation; personal compensation as a consultant/scientific advisory board member for Abbvie, TEVA, Impax, Merz, Acadia, Cynapsus, Lundbeck and USWorldMeds; royalties from Lippincott Williams & Wilkins and Cambridge University Press; and honoraria from Abbvie, USWorldMeds, Lundbeck, Acadia, the American Academy of Neurology and the Movement Disorders Society. JBR receives salary support from the Wellcome Trust (103838) and has received peer-reviewed research support from Wellcome Trust, Medical Research Council, National Institute for Health Research, PSP-Association, Parkinson's UK, Alzheimer's Research UK, The Evelyn Trust James F McDonnell Foundation and an academic research grant from AZ-Medimmune. AEL has served as an advisor for Abbvie, Allon Therapeutics, Avanir Pharmaceuticals, Biogen Idec, Boerhinger-Ingelheim, Bristol Myers Squibb, Ceregene, Cipla, Intekrin, Lilly, Medtronic, Merck, Novartis, NeuroPhage Pharmaceuticals, Teva and UCB; received honoraria from Medtronic, Teva, UCB and AbbVie; received grants from Brain Canada, Canadian Institutes of Health Research, Edmond J Safra Philanthropic Foundation, Michael J. Fox Foundation, Ontario Brain Institute, National Parkinson Foundation, Parkinson Society Canada, Physicians Services Incorporated (PSI), Tourette Syndrome Association and W. Garfield Weston Foundation; received publishing royalties from Saunders, Wiley-Blackwell, Johns Hopkins Press and Cambridge University Press; and has served as an expert witness in cases related to the welding industry. MM has served as an advisor to Bioscape Medical Imaging CRO, Novartis and UCB; received honoraria from Novartis; received royalties from Henry Stewart Talks; received an investigator-initiated research grant from Teva; received contract research support from Roche and Novartis; received peer-reviewed research support from Canadian Institutes of Health Research, Ministry of Economic Development and Innovation (Ontario), Weston Brain Institute, Sunnybrook AFP Innovation Fund, Washington University, Parkinson Society Canada, Alzheimer's Drug Discovery Foundation, Brain Canada and Ontario Brain Institute; and received salary support from the Department of Medicine at Sunnybrook Health Sciences Centre and University of Toronto and from the Sunnybrook Foundation.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.