Article Text

Abstract
Stroke is a major cause of neurological morbidity and mortality. Atherosclerosis is a major contributor to first and recurrent stroke. A growing evidence base indicates that inflammation is a key process in the pathogenesis of atherosclerosis, leading to thromboembolic events. In this review, we summarise the evidence linking inflammation to stroke risk and discuss clinical trials addressing the ’inflammation hypothesis' in coronary disease and stroke.
Trial registration number CONVINCE trial ClinicalTrials.gov number; NCT 02898610; Pre-results.
- stroke
Statistics from Altmetric.com
Introduction
The WHO estimates that cardiovascular diseases are the leading cause of death globally, causing 17.5 million deaths in 2012. Of these, stroke was the second leading cause of global death.1 Cerebrovascular disease is the most common cause of neurological disability in older adults and contributes substantially to dementia. Stroke incidence rates are increasing rapidly in low-income and middle-income countries and absolute numbers are rising in high-income countries due to increasing life expectancy.2 The American Heart Association estimates that annual total (direct and indirect) costs of stroke were $34 billion in 2011.3
Primary and secondary prevention of early and late recurrent events is a major strategy to reduce the overall burden of stroke. Antithrombotic, lipid-lowering, antihypertensive therapy and lifestyle modification are proven approaches for stroke prevention.4 Recent data indicate that atherosclerotic plaque inflammation may be an important contributor to plaque destabilisation and thromboembolic events. In patients with coronary artery disease, clinical trials of anti-inflammatory therapies to prevent subsequent vascular events are under way. We aimed to review the medical literature relating to plaque inflammation in cerebrovascular disease, with a specific focus on clinical trials targeting atherosclerotic inflammation for secondary stroke prevention.
Importance of atherosclerosis in cerebrovascular disease
Atherosclerosis of the aorta, cervical or intracranial large or small arteries is a major pathophysiological finding causally related to or associated with a large proportion of ischaemic stroke. This view is supported by four main lines of evidence.
First, direct imaging evidence of atherosclerotic narrowing of the aorta or craniocervical arterial system is common in patients with ischaemic stroke or transient ischaemic attack (TIA). Population-based and hospital studies have reported ipsilateral carotid stenosis (≥50% arterial lumen narrowing) in 12–20% of patients with ischaemic stroke,5–10 with intracranial atherosclerosis (ICAS) in a further 8–10% of North American/European and 30–50% of Asian patients.11 12 Symptomatic ICAS is associated with pathological features of plaque instability (rupture, inflammation) and inflammatory markers such as C reactive protein (CRP) and leucocyte count predict recurrent vascular events in patients with ICAS.13–17 Recent data also suggest that arterial stenosis of less than 50% may play an aetiological role in acute ischaemic stroke. A cross-sectional study of 85 Embolic Stroke of Undetermined Source (ESUS) cases imaged by CT angiography showed that plaque 3–5 mm in thickness was present ipsilateral to the stroke in 11–35% of cases versus 1–15% on the contralateral side. There was a poor correlation between plaque volume and degree of stenosis.18
Second, indirect evidence suggests that atherogenic embolism originating from the arterial system is likely to contribute to a substantial proportion of patients with stroke in whom no direct mechanism is identified, which account for 18–35% of all strokes in registries and clinical trials19 In the EMBRACE (Cardiac Event Monitor Belt for Recording Atrial Fibrillation After a Cerebral Ischemic Event) trial, paroxysmal atrial fibrillation (AF) was detected in only 16% at 90 days of patients with cryptogenic stroke or TIA who underwent prolonged cardiac monitoring.20 In the CRYSTAL-AF trial (Study of Continuous Cardiac Monitoring to Assess Atrial Fibrillation After Cryptogenic Stroke), AF was detected in 9% of patients with cryptogenic stroke/TIA at 6 months and 30% by 36 months.21 However, it is unclear whether late detection of AF in CRYSTAL-AF was causally related to the initial event. Taken together, these data suggest that a substantial proportion of cryptogenic stroke/TIA cases were unrelated to cardiac embolism.
In the North Dublin Population Stroke Study, 73% of patients with TOAST-classified (Trial of ORG 10172 in Acute Stroke Treatment) stroke of unidentified aetiology had evidence of aortic or craniocervical atherosclerosis defined by the ASCO (A: atherosclerosis; S: small-vessel disease; C: cardiac pathology; O: other causes) classification.22 Thick (>4 mm) plaque of the aortic arch is also frequent in patients with cryptogenic stroke, with a prevalence of 28% reported in one prospective study.23 In this study, plaque >4 mm was almost 5 times more frequent in patients with cryptogenic stroke compared with those with stroke of identified cause (adjusted OR 4.7, CI 2.2 to 10.1), supporting the hypothesis that aortogenic embolism may have accounted for symptoms. Further indirect evidence supporting a role of aortogenic embolism may emerge from ongoing trials currently evaluating rivaroxaban and dabigatran for secondary prevention in patients with ESUS.
Third, microatheroma is an important contributor to ischaemic disease of cerebral small vessels (arteries and arterioles), which accounts for up to 20% of stroke and is a major contributor to dementia.24 Although the pathophysiology of cerebral ischaemic small vessel disease is varied and not fully understood, existing data suggest two common mechanisms24: (1) microatheroma of larger penetrating arterioles, causing single, frequently symptomatic acute lacunar infarcts and (2) lipohyalinosis (‘arteriolosclerosis’), more frequently associated with diffuse white matter hyperintensity on neuroimaging and neuropathological evidence of cerebral demyelination.
Fourth, randomised clinical trials in patients with non-cardioembolic stroke and TIA have demonstrated benefit of targeting plaque-related lipid accumulation with high-dose atorvastatin and platelet activation to prevent recurrent stroke and coronary events.25–27
High residual vascular risk in stroke survivors
Although suboptimal secondary prevention is common among survivors of stroke and TIA,28 29 the residual risk of recurrent stroke, coronary events and vascular death is substantial even among those treated with high rates of established secondary preventive medications. Data from recent clinical trials and stroke registries indicate a recurrent stroke risk of 2.5–4% per year in patients treated with high rates of statin and antiplatelet therapies after stroke and TIA.30–33 A systematic review reported a cumulative pooled recurrent stroke risk of 11.1% at 1 year and 26.4% at 5 years.34 The risk of myocardial infarction (MI) and vascular death is also substantial in long-term stroke/TIA survivors. In a systematic review (39 studies, 65 996 patients), Touze found a 2.1 %/year rate of non-stroke vascular death and 0.9 %/year risk of non-fatal MI in stroke survivors.35 Early stroke recurrence risk after first stroke and TIA is highest in patients with large-artery atherosclerosis of the cervical carotid arteries, intracranial vessels or posterior circulation, compared with other stroke mechanisms.33 36–39 The mechanisms explaining this residual risk are unclear. However, evidence from multiple sources support the hypothesis that inflammation-related plaque instability may be an important contributing factor.40
Inflammation and pathophysiology of atherosclerotic plaque
Accumulating evidence supports the view that inflammation is of key importance in the pathophysiology of atherosclerotic plaque destabilisation and thromboembolism.41–43 A large body of experimental data indicates that inflammatory cells are involved in all stages of atherosclerosis development. Transendothelial migration of circulating monocytes is a key event in the initiation of atherosclerotic plaque, mediated by surface adhesion molecule expression in response to endothelial stimuli such as arterial tension, non-laminar flow, cigarette smoke constituents and angiotensin 2. Retention of low-density lipoprotein (LDL) lipids in the extracellular matrix of the arterial wall is accompanied by differentiation of monocytes and lipid uptake to lipid-laden ‘foamy’ macrophages. Differentiation of macrophages into proinflammatory subsets (M1 macrophages) results in local expression of proinflammatory cytokines, particularly interleukin 1-beta (IL-1β) and tumour necrosis factor-alpha (TNF-α). Cytokines such as platelet-derived growth factor promote recruitment and proliferation of smooth muscle cells into the endothelial cell layer, which express matrix proteins such as collagen and elastin. As plaque progression continues, a fibrous cap of endothelial cells mainly smooth muscle cells and collagen develops, overlying a plaque matrix comprising monocyte–macrophages, connective tissue proteins, extracellular lipids, smooth muscle cells and neovascularisation. Local ingress of T helper (T-H1) cells produces proinflammatory cytokines, particularly IFN-γ, while T-regulatory cells produce inhibitory cytokines such as IL-10 and TGF-β. Apoptosis of macrophages and smooth muscle cells releases lipid and cellular debris within the extracellular matrix to form a lipid-rich necrotic core containing procoagulant tissue factor. Expression of cytokines and collagenolytic enzymes such as metalloproteinases from macrophages and other cells contributes to erosion and rupture of the fibrous cap, exposure of circulating platelets and coagulation factors to the prothrombotic core and subsequent thromboembolism.
Association of stroke with inflammation from clinical studies
Clinical and epidemiological data supporting the association of plaque inflammation with stroke are derived from six main sources: (1) epidemiological studies of inflammatory biomarkers; (2) epidemiological studies of the association of infection with stroke risk; (3) genetic epidemiological studies of gene polymorphisms in inflammation pathway proteins; (4) clinical–pathological studies; (5) plaque imaging studies and (6) randomised clinical trials of anti-inflammatory agents in vascular disease.
Epidemiological studies of inflammatory biomarkers
The central inflammatory pathway is characterised by the key cytokines IL-1, IL-6 and TNF-α. Epidemiological studies have consistently described dose-dependent associations between circulating blood biomarkers of this pathway and vascular disease, including stroke. Such biomarkers can be considered as ‘downstream’ (eg, CRP) and ‘upstream’ markers (eg, IL-6, TNF-α).43
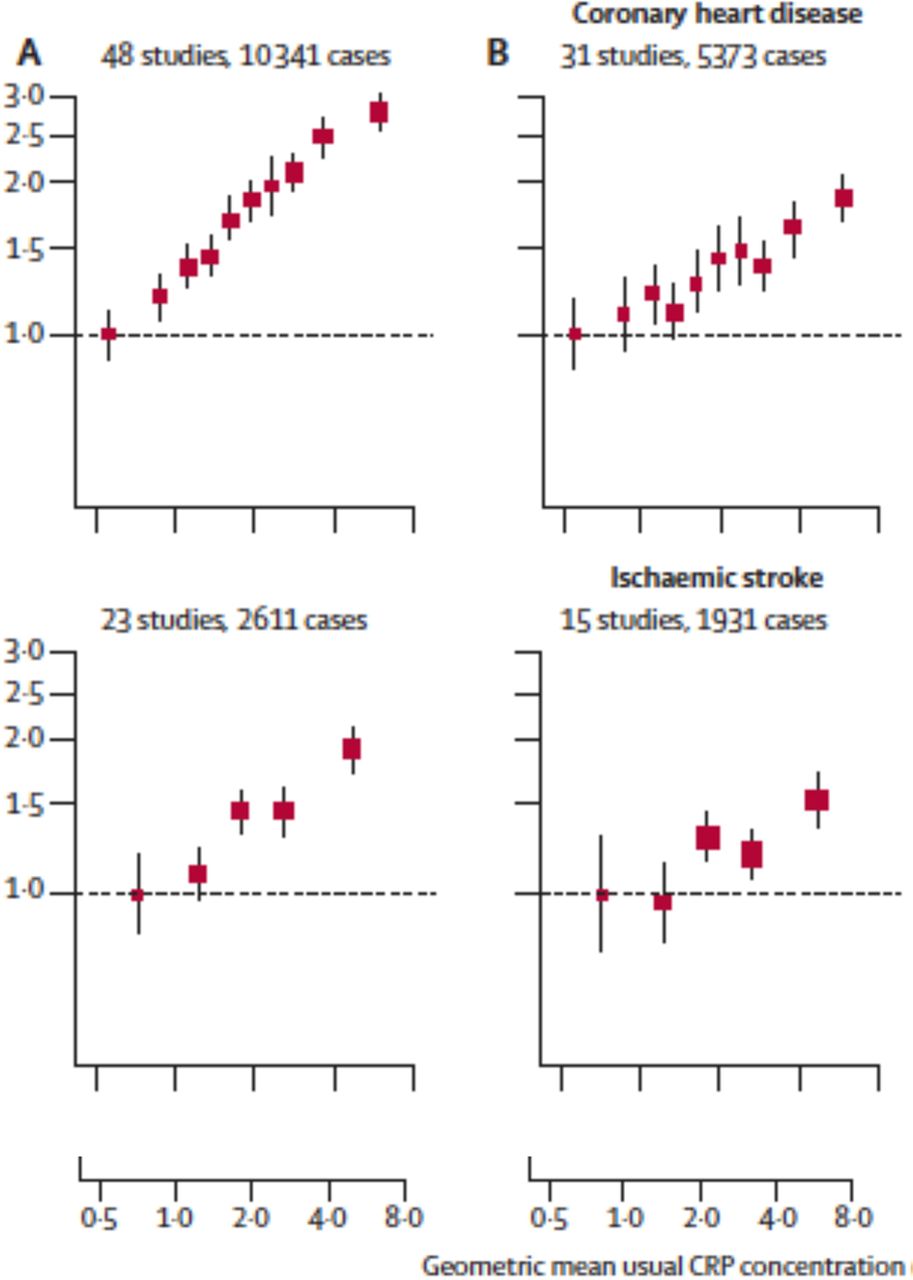
The Emerging Risk Factors Collaboration has described the relationship between circulating CRP and incident stroke in 160 309 individuals without vascular disease in prospective studies.44 After adjusting for age, sex and study, a linear relationship was observed between circulating CRP and risk of ischaemic stroke, which remained (although attenuated) after further adjustment for existing vascular risk factors (figure 1). The adjusted relative risk (RR) per threefold increase in CRP was 1.27 (95% CI 1.15 to 1.40). A similar relationship was observed for coronary disease.

Linear association of C reactive protein (CRP) with new coronary disease (top) and stroke (bottom) in 160 309 individuals without vascular disease, adjusted for age, sex and study (left, graphs A), and additionally for vascular risk factors (right, graphs B). Adjusted relative risk per threefold increase in CRP was 1.37 (CI 1.27 to 1.48) for coronary heart disease and 1.27 (CI 1.15 to 1.4) for ischaemic stroke (reprinted with permission from Kaptoge et al 44).
CRP is increased following acute stroke in response to tissue injury and infection, proportionate to the severity of the acute event.45 In the post-acute phase, CRP remains elevated compared with control subjects, with greatest elevation in patients with large-artery stroke mechanisms. CRP has been reported to independently predict recurrent stroke risk in patients with stroke or TIA due to carotid or ICAS.46 47 Recently, CRP measured at baseline was reported to independently predict the risk of recurrent stroke and vascular events in the SPS3 (Secondary Prevention of Small Subcortical Strokes Trial)and CHANCE (Clopidogrel in High-risk Patients With Acute Non-disabling Cerebrovascular Events) trials. In 1244 patients with lacunar stroke in SPS3, baseline CRP was associated with a 2.32-fold increase in the adjusted hazard of recurrent stroke and vascular events (highest versus lowest quartile).48 In 3044 patients with non-severe non-cardioembolic stroke in the Chinese CHANCE trial, patients in the highest CRP quartile measured at baseline had a 1.46-fold increase in the adjusted risk of early recurrent stroke at 90 days and increased risk of stroke at 1 year.49 In 1232 patients with recent stroke/TIA in the Oxford Vascular Study, CRP measured in the acute phase was an independent predictor of 90-day stroke recurrence (adjusted HR 1.15, CI 1.02 to 1.30).50 Broadly consistent findings have been observed with other inflammatory biomarkers, including fibrinogen and IL-6.50 51
Studies of association between infection and stroke risk
Inflammation of the cerebral arterial wall in response to direct infection by varicella zoster virus has long been recognised as a cause of ischaemic stroke. Other viruses (cytomegalovirus (CMV), hepatitis B, hepatitis C, Epstein-Barr virus), fungal (Aspergillus, Histoplasma) and bacterial (syphilis, Mycobacterium tuberculosis, Haemophilus influenzae) may also trigger cerebral vasculitis and stroke via direct arterial wall invasion, immune complex deposition or secondary cryoglobulinaemia.52–54 These occur typically, although not exclusively, in immune-suppressed patients. HIV has recently been associated with extensive remodelling of the cerebral arterial wall, although the role of inflammation in this process is unclear.55
Epidemiological studies have reported associations between chronic infection and stroke risk. Infective agents have been diverse, including Chlamydia pneumoniae, H influenzae, Helicobacter pylori, Herpes simplex 1 and 2, CMV and Epstein-Barr virus.56 The Northern Manhattan Study reported an association (adjusted HR 1.39) between overall infectious burden, defined as cumulative exposure to several prespecified infective agents, and first-ever stroke risk.57 However, this finding requires further confirmation, as other studies have not demonstrated an association between chronic infectious burden and stroke risk.58 59 Recent data suggest that acute infection may be associated with higher stroke risk. In an analysis from the Cardiovascular Health Study, Elkind and colleagues reported increased risk of first-ever stroke associated with hospital admission for treatment of infection, with greatest risk observed at earliest time points.60 The adjusted HR for stroke within 90 days of admission was 2.4 (CI 1.6 to 3.4). Further studies are required to definitively confirm this finding.
Genetic epidemiology studies
Despite sophisticated analytical methods, the interpretation of epidemiological studies investigating blood biomarkers may be limited by residual confounding and ‘reverse causality’ (where subclinical disease may influence the biomarker levels). Epidemiological studies of gene variants affecting protein function in key pathways overcome these limitations, as, by definition, exposure is determined prior to the onset of disease.
One such functional polymorphism exists in the IL-6 receptor gene, causing an alanine-to-aspartate substitution at position 358 of the expressed protein, resulting in reduced membrane-bound IL-6 receptor, impaired IL-6 signalling and reduced expression of downstream CRP and fibrinogen. Two ‘Mendelian randomisation studies’ have reported associations of this polymorphism with reduced risk of coronary heart disease after adjusting for conventional risk factors in a dose-dependent fashion depending on the number of 358Ala alleles inherited, with consistent effect sizes (per allele, 3.4%, CI 1.8 -5% and 5%, CI 3-7%).61 62 Similar reductions in CRP and fibrinogen were observed, supporting the biological plausibility of the findings. However, stroke was not reported as an outcome in these studies. Genome-wide association studies in patients with ischaemic stroke with sufficiently large sample sizes may elucidate the role of these variants in stroke.
Clinical–pathological studies
Pathological studies also support an association between plaque inflammation and clinical events. For example, an analysis of resected carotid plaque from 526 patients with symptomatic carotid stenosis in the Oxford Plaque Study found that 66% of patients had evidence of marked inflammation in resected plaque from the ipsilateral internal carotid artery, while 64% had other features of plaque instability (thin fibrous cap, large lipid core, cap rupture or superficial thrombus).63 Extensive macrophage infiltration was independently associated with plaque rupture (adjusted OR 3.52, p<0.001), as were cap thickness <200 µm (OR 2.64), intraplaque haemorrhage (OR 2.65) and large lipid core (OR 4.03) (all ORs adjusted, p<0.001 for all).
Similar findings were observed in a smaller study investigating the relationship of plaque inflammation with early recurrent stroke.64 In 44 consecutive patients with ipsilateral carotid stenosis and TIA/ischaemic stroke who had endarterectomy within 10 days (IQR 7–17 days), early stroke recurrence pre-endarterectomy was associated with extensive macrophage and lymphocyte infiltration (Oxford Plaque Score ≥3), low fibrous content, ≥25% cap disruption and plaque neovascularisation. After adjustment for age and degree of stenosis, high macrophage density was the only independent predictor of early stroke recurrence (adjusted HR 9.0, p=0.04).
Matrix metalloproteinases (MMPs) are proteolytic enzymes for which subendothelial matrix collagen and elastin are known substrates. In patients with small artery disease, increased inflammatory cells (macrophages, activated microglia) expressing MMPs are present around affected arterioles and areas of ischaemic demyelination and MMP-9 is increased in cerebrospinal fluid.65 66
Plaque imaging studies
Positron emission tomography using 18-fluorodeoxyglucose (FDG-PET) is a validated technique for imaging plaque metabolic activity, mainly related to inflammatory monocyte–macrophage activity. Tawakol reported high FDG uptake in symptomatic carotid plaque, with high (r=0.89) correlation with plaque macrophage density.67 Cross-sectional studies have established that plaque FDG uptake is correlated with other markers of plaque instability, such as microembolic signals on transcranial Doppler ultrasound, unstable plaque morphology and expression of inflammatory cytokines and proteases.68–70 Longitudinal studies in patients who underwent whole-body PET for cancer screening have reported that aortic FDG uptake independently predicts late vascular events, including stroke. In 60 patients with recent stroke/TIA and ipsilateral carotid stenosis, we found that carotid plaque FDG uptake was an independent predictor of early pre-endarterectomy stroke recurrence, after adjusting for age and degree of stenosis (adjusted HR 6.1, CI 1.3 to 28.8, p=0.02) (figure 2).71 The 90-day stroke recurrence rate for patients in the highest FDG uptake tertile was 59% compared with 19% and 13% in the lowest tertiles (log-rank p=0.03) (figure 3). Other groups have reported similar findings.72 73 An international multicentre study (Biomarkers and Imaging Of Vulnerable Atherosclerosis in Symptomatic Carotid atherosclerosis (BIOVASC)) is under way to test the validity of these findings in an independent cohort.

(A) (Left image): Axial CT angiogram of patient with left hemisphere transient ischaemic attack and internal carotid artery origin stenosis (arrow). (B) (Right image): Fused 18-FDG PET/CT image demonstrating focus of increased FDG uptake reflecting inflammatory hypermetabolism at site of carotid mural plaque (arrow). 18-FDG-PET, 18-fluorodeoxyglucose positron emission tomography.

Early recurrent stroke in patients with non-severe stroke or TIA and ipsilateral carotid stenosis, stratified by tertile of 18-FDG uptake in symptomatic plaque on positron emission tomography/CT. Stroke recurrence rates were 59% in highest FDG uptake tertile versus 19% and 13% in the lowest and middle tertiles (log-rank p=0.03). In a Cox regression model adjusted for age and degree of stenosis, the HR for stroke recurrence was 6.1 per 1 standard uptake value of plaque FDG activity (CI 1.3 to 28.8, p=0.02) (reprinted with permission from Marnane et al 71).
Randomised trials in patients without cerebrovascular disease
In patients without clinical cerebrovascular disease, several randomised clinical trials testing the hypothesis that inhibiting inflammation may prevent cardiovascular events have been completed or are under way (table 1). In addition to their lipid-lowering effects, statins are known to influence other biological pathways (pleotropic effects), including anti-inflammatory effects. Small studies have demonstrated reduction in blood biomarkers and plaque FDG uptake in a dose-dependent manner by statins.74 75 In the JUPITER trial, 17 802 patients without a history of vascular disease, low-normal LDL cholesterol and CRP ≥2 mg/L were randomly allocated to receive either rosuvastatin 20 mg or placebo.76 Rosuvastatin treatment reduced LDL by 50% and CRP by 37%. The trial was halted early due to benefit, with a relative risk reduction (RRR) in major vascular events of 46% in rosuvastatin-treated patients. In a prespecified secondary analysis, the RRR for stroke was 48% (p=0.002). However, the interpretation of these findings was unclear due to the non-specific effects of rosuvastatin on both inflammation and LDL metabolism.
Large prevention trials targeting atherosclerotic inflammation in cardiovascular disease
Other trials which targeted secretory lipoprotein-associated phospholipase A2 (Lp-PLA2), which has been hypothesised to be implicated in atherosclerosis development using specific antagonists (darapladib, varespladib) did not show benefit in patients with recent or stable coronary disease.77–79 However, as Lp-PLA2 is not centrally involved in the classical IL1–IL6–TNF-α inflammatory pathway, these results should be interpreted with caution.
Clinical trials using specific and direct anti-inflammatory interventions are under way in non-stroke populations (table 1).40 43 In CANTOS, canukinumab (an IL-1β antagonist) is under evaluation in 10 000 patients with stable coronary disease selected on the basis of CRP ≥2 mg/L. The National Institutes of Health-funded Cardiovascular Inflammation Reduction Trial (CIRT) is comparing low-dose weekly methotrexate (15 or 20 mg per week) with placebo plus recommended care in 7000 patients with stable coronary disease and diabetes or metabolic syndrome. In Australia, the LoDoCo2 trial is examining the efficacy of low-dose colchicine compared with placebo in addition to usual care in patients with stable coronary disease (see below). An ongoing trial (ENTRACTE) is comparing the IL-6 antagonist tocilizumab with entanercept for prevention of major cardiovascular events in patients with rheumatoid arthritis and cardiovascular risk factors.
Randomised trials of anti-inflammatory treatments for secondary stroke prevention
To assess the literature of trials of anti-inflammatory agents for stroke prevention, we conducted a systematic review of published data. We searched MEDLINE for completed published trials and the Clinicaltrials.gov registry for ongoing trials. Prespecified inclusion criteria were: (1) randomised controlled trials testing the addition of anti-inflammatory agents to standard care in patients with clinical cerebrovascular disease (study size 100 patients or more with at least 80% of included patients with stroke/TIA); (2) inclusion of stroke as a primary or secondary outcome measure; (3) inclusion of adults only (age ≥18 years); (4) English language publication and (5) publication year 1966–July 2016. The initial search strategy (Web-appendix) revealed 453 studies. However, after review of abstracts, only a single ongoing trial (CONVINCE) testing low-dose colchicine for secondary prevention in patients with clinical cerebrovascular disease was identified.
Crystal-induced inflammation and atherosclerosis
Crystallised extracellular cholesterol has long been recognised as a common feature of atherosclerotic plaque, but was often considered as a bystander phenomenon in plaque development. Recent experimental and clinical–pathological studies have shown that microscopic cholesterol crystals form very early in atherosclerotic plaque development and may be a potent inflammatory stimulus for neutrophils and macrophages. Studies in apolipoprotein E-deficient mice have demonstrated that cholesterol crystals activate monocytes–macrophages via the intracellular nucleotide-binding leucine-rich repeat-containing pyrin receptor (NLRP) inflammasome protein complex. This causes increased IL-1β expression, which is known as a key event in the initiation of local and systemic inflammatory cascades, evidenced by elevated IL-6 and CRP.80–82 These important observations provide direct evidence linking plaque lipid metabolism and inflammation. Indirect support for these findings in humans is provided by a PET study in patients with symptomatic carotid stenosis, where 18-FDG uptake in symptomatic plaque was associated with total and LDL cholesterol and inversely associated with HDL cholesterol, after adjustment for confounding variables.83
Uric acid is a product of purine metabolism which undergoes hepatic and renal elimination in vivo. Uric acid is a potent antioxidant with neuroprotective effects in animal models and established safety in humans.84 However, hyperuricaemia is strongly associated with atherosclerosis risk factors, such as hypertension, renal impairment, obesity, metabolic syndrome and ethanol excess.85 In epidemiological studies, serum urate has been associated with inflammatory blood biomarkers, suggesting that hyperuricaemia may predispose to a proinflammatory state.86 87 Some studies have described associations between hyperuricaemia and subclinical markers of atherosclerosis, such as carotid intima-media thickness and coronary artery calcification burden.88 However, these associations have not persisted after adjustment for vascular risk factors, raising the possibility that uric acid may be a risk marker rather than a causal factor. Data are conflicting regarding the association between uric acid and cardiovascular events, including stroke. Several studies have also reported positive associations. For example, in the Rotterdam Study, the HR of ischaemic stroke was 1.77 (CI 1.1 to 2.83) in the fifth compared with the first quintile of uric acid, with only minimal attenuation after adjustment for vascular risk factors.89 However, other studies, including the Framingham and Atherosclerosis Risk in Communities studies, have not replicated these findings.90 91
In gout, monosodium urate crystals are deposited in joints and bursae, causing activation of the NLRP inflammasome, IL-1β generation and both local and systemic inflammation. Crystal-induced inflammation, via either cholesterol and/or monosodium urate crystals, may be a common mechanism underlying the associations between inflammation, lipid metabolism and hyperuricaemia.
Potential of colchicine for prevention of atherosclerotic events
Colchicine has been a mainstay of treatment for gout for centuries.92 93 Although traditionally high-dose colchicine was associated with gastrointestinal (GI) problems when used for acute gout flares, recent guidelines have recommended that similar efficacy may be achieved with major improvements in tolerability when lower doses are used.92 Long-term low-dose colchicine is safe and effective for gout prevention and has been a cornerstone of treatment of Bechet’s Disease and Familial Mediterranean Fever for decades.93
Via binding to α-tubulin and β-tubulin proteins, colchicine has multiple anti-inflammatory properties, including inhibition of microtubule polymerisation, with inhibition of leucocyte rolling and endothelial adhesion, impaired leucocyte motility, phagocytosis and cytokine secretion. It inhibits crystal-induced activation of the NLRP inflammasome, thus inhibiting caspase-1 proteolysis and IL-1β secretion in monocyte–macrophages.
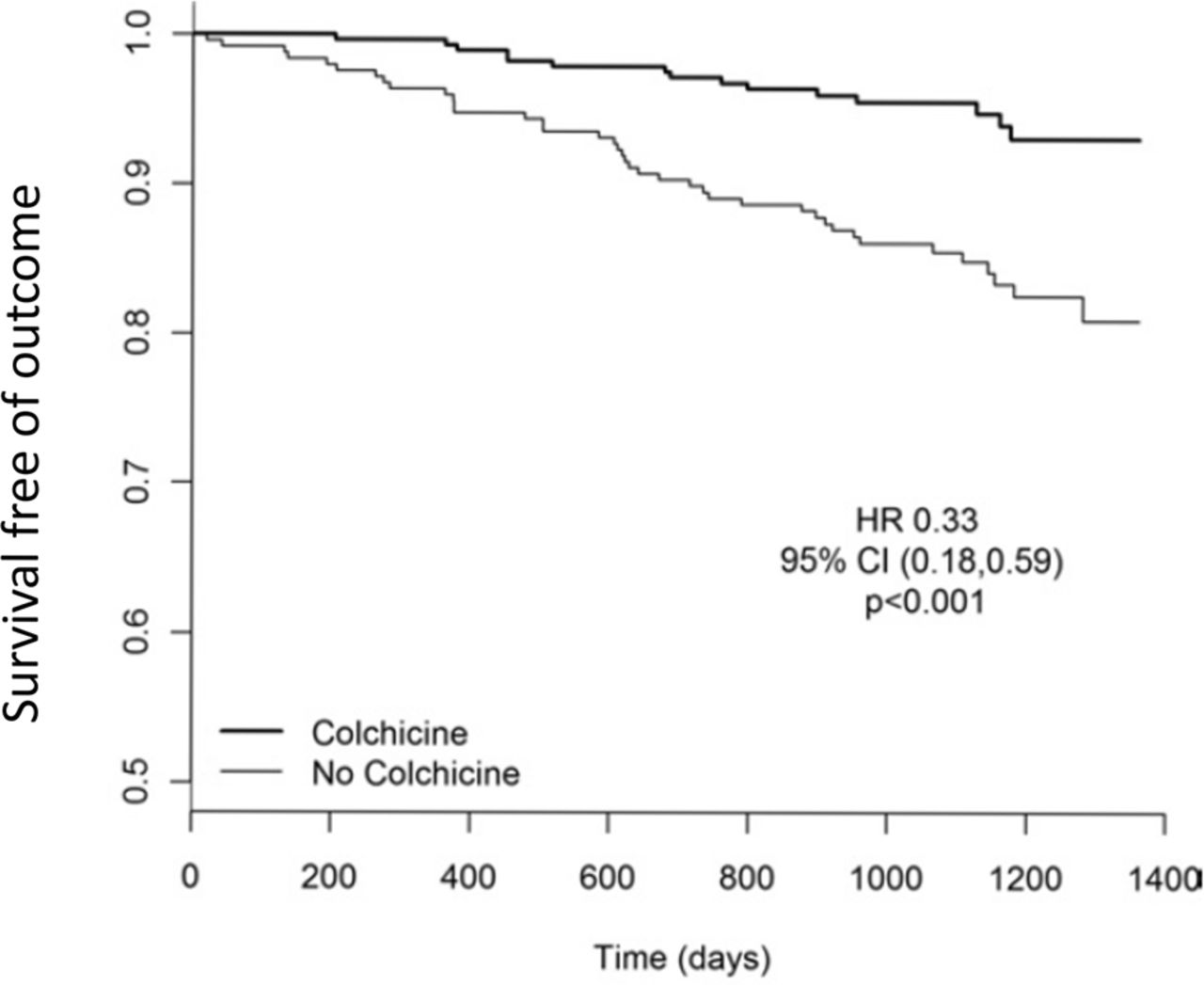
Observational data report lower rates of coronary disease in gout and familial mediterranean fever associated with colchicine therapy.94 In patients with stable coronary atherosclerosis treated with low-dose colchicine, statins and antiplatelet agents, CRP was reduced by 60%, but was unchanged in controls (p=0.002).95 In the LoDoCo randomised trial, 532 patients with chronic stable coronary disease were randomised to the lowest available dose of colchicine (0.5 mg/day) or usual care.96 Almost all were taking antiplatelet agents and high-dose statins at baseline and antihypertensive therapy as indicated. Over a median follow-up of 36 months, the risk of major cardiovascular events was reduced by 67% in patients treated with low-dose colchicine (HR 0.33, CI 0.18 to 0.59, p<0.001) (figure 4). Only five stroke events occurred (as expected in this patient sample), but the direction of benefit for stroke was similar to that for coronary events (four strokes in controls versus one in colchicine group, p=0.18). Colchicine had an excellent safety profile. The the most common adverse effect was intestinal upset (2.5%) with myalgia in two patients (0.9%) and myositis, rash, itch, alopecia or peripheral neuropathy reported in one patient each (<0.5%) and no excess of deaths observed. Recent trials have also demonstrated benefit of low-dose colchicine (0.5–1 mg/day) for prevention of recurrent pericarditis and reduced infarct size when used acutely in patients with ST-elevation MI.97 98

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative risk of major cardiovascular events in LoDoCo trial in patients with stable coronary disease treated with low-dose colchicine plus usual care compared with usual care alone (reprinted with permission from Nidorf et al 96).
A 2016 Cochrane Systematic Review has investigated the safety and benefits of long-term colchicine use with particular emphasis on cardiovascular disease.99 It included 39 trials overall of 4992 patients and 4 trials of 1230 patients with heart disease. The risk of MI was reduced by 80% (RR 0.2, CI 0.07 to 0.57, two trials, 652 patients, moderate quality evidence). No increased risk of serious adverse events was observed. Colchicine was associated with increased GI intolerance, generally mild and short-lived.
CONVINCE: can anti-inflammatory therapy with colchicine prevent recurrent stroke?
The underlying pathophysiology of recurrent vascular events in patients with non-cardioembolic stroke is likely to resemble that in patients with coronary artery disease. Informed by the growing body of experimental and clinical data supporting a rationale for treatment with colchicine in vascular disease, the CONVINCE trial will test the hypothesis that daily low-dose colchicine (0.5 mg/day) combined with usual care (lifestyle advice plus antiplatelet, antihypertensive and lipid-lowering therapy) will have benefit for prevention of recurrent stroke and major vascular events compared with usual care alone.100 Similar to other stroke secondary prevention trials of antiplatelet and lipid-lowering therapy, CONVINCE will include patients with non-severe (Modified Rankin Score 3 or less) stroke or TIA, randomised between 72 hours and 28 days of symptom onset and followed for a median of 36 months. Patients with cardioembolic stroke/TIA, those with other identified non-atherosclerotic stroke mechanisms (eg, arterial dissection) or contraindication to colchicine therapy will be excluded. The tolerability and safety of colchicine will be closely monitored, with a prespecified review after completion of randomisation of the initial 10% of the trial sample (internal pilot ‘Vanguard’ stage).
Conclusion
Atherosclerosis of different vessels has been associated with a large proportion of ischaemic stroke. Growing evidence has emerged based on experimental, epidemiological and clinical data in recent years to support the hypothesis that inflammatory pathways are key mediators in the development of atherosclerosis, leading to stroke and other vascular events. This ‘inflammation hypothesis’ has been the basis of several clinical trials using different agents in patients with coronary disease and colchicine has shown promising therapeutic potential until now. These findings require further study in ischaemic stroke and will be tested in the CONVINCE trial. Further trials are needed to improve our understanding of the role of atherosclerotic inflammation in stroke pathogenesis.
References
Footnotes
Contributors All authors fulfil ICMJE guidelines for authorship as follows: Professor Kelly contributed to the conception of the article, the design of the systematic search of trials of anti-inflammatory medication for stroke prevention and interpretation of search data. He wrote the first draft and critically revised the manuscript for important intellectual content. He gave final approval of the version published. He agrees to be accountable for all aspects of the work in accordance with ICMJE guidelines. Professor Murphy, Professor Price, ProfessorTsivgoulis, Professor Lemmens and Professor Purroy contributed to the conception of the article, contributed to revised drafts of the manuscript and critically revised the manuscript for important intellectual content. They gave final approval of the version published. They agree to be accountable for all aspects of the work in accordance with ICMJE guidelines. Dr Coveney contributed to the conception of the article, contributed to revised drafts of the manuscript and critically revised the manuscript for important intellectual content. She conducted the search of anti-inflammatory therapies for secondary stroke prevention, summarised and interpreted the findings. She gave final approval of the version published. She agrees to be accountable for all aspects of the work in accordance with ICMJE guidelines.
Competing interests PJK is chief investigator of the CONVINCE (COlchicine for preventioN of Vascular Inflammation in Non-Cardio-Embolic stroke) trial funded by the Health Research Board of Ireland. SM, FP, RL, GT and CP are national lead investigators for CONVINCE in their respective countries and serve on the trial steering committee.
Provenance and peer review Not commissioned; externally peer reviewed.