Article Text

Abstract
Background No consensus exists which quality of life (QoL) measure should be used in patients with inflammatory neuropathies. Moreover, most QoL measures are ordinal-based scales with their known deficiencies.
Objectives To establish a new disease-specific interval-based QoL questionnaire in inflammatory neuropathies (IN-QoL) using the Rasch model and evaluate its scientific properties (validity, reliability and responsiveness).
Methods 264 patients with inflammatory neuropathies completed six commonly used QoL questionnaires. The obtained data were stacked and subjected to Rasch analysis. Responsiveness was determined by using the concept of minimum clinically important differences related to varying individually obtained SEs (responsiveness definition: MCID-SE≥1.96 after 1-year follow-up compared with baseline).
Results The IN-QoL fulfilled all Rasch’s model requirements with high internal reliability values (patient separation index of 0.94), except being multidimensional. Additional factor analysis resulted in two (functional and mental) subsets that were unidimensional on their own. The IN-QoL showed good correlation with the EuroQol-health quality visual analogue scale (EQ-VAS) (Spearman’s rho 0.72). It demonstrated acceptable responsiveness in patients with Guillain-Barré syndrome (GBS) and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), as did the EQ-VAS. In patients with monoclonal gammopathy-related neuropathy and multifocal motor neuropathy, hardly any changes were seen over time.
Conclusion The IN-QoL questionnaire fulfils modern clinimetric requirements and correlates strongly with a patient’s self-assessment of their own quality of health, while also showing responsiveness in patients with GBS and CIDP. We propose using the IN-QoL and the EQ-VAS for assessing the QoL of patients with inflammatory neuropathies in future studies.
- Guillain-Barré syndrome (GBS)
- Chronic inflammatory demyelinating polyneuropathy (CIDP)
- IgM-monoclonal gammopathy of undetermined significance-related polyneuropathy (MGUSP)
- peripheral neuropathy
- multifocal motor neuropathy (MMN)
- Quality of Life (QoL)
Statistics from Altmetric.com
- Guillain-Barré syndrome (GBS)
- Chronic inflammatory demyelinating polyneuropathy (CIDP)
- IgM-monoclonal gammopathy of undetermined significance-related polyneuropathy (MGUSP)
- peripheral neuropathy
- multifocal motor neuropathy (MMN)
- Quality of Life (QoL)
Introduction
Quality of life (QoL) is a highly valued outcome measurement in any chronic illness in modern medicine. Over time, a multitude of questionnaires have been developed aiming to capture patient’s QoL.1–8 These questionnaires are created for example through patient focused groups, experts’ opinion or by combining different pre-existing questionnaires. Several of these questionnaires have fulfilled the basic clinimetric requirements like being valid, reliable and responsive.4–8 However, most, if not all, QoL instruments have limitations such as summing up ordinal data with their known deficiencies.9–12 Furthermore, they are often used outside the field for which they were initially developed, assuming that QoL could be captured in the same way across all fields of medicine, thus not respecting potential disease-specific aspects. Only few scales are designed specifically for peripheral neuropathies, but both are based on ordinal sum scores.7 13 To date, no consensus exists regarding which QoL measure should be used in patients with inflammatory neuropathies. Based on these observations, we aimed to create an interval-based QoL questionnaire specifically for inflammatory neuropathies (IN-QoL) from a comprehensive set of items, originating from six commonly used QoL questionnaires, aiming for the metric to be unidimensional, free from item bias, without disordered thresholds or local dependency, and fulfilling all Rasch model requirements. In addition, we examined the scientific soundness (validity, reliability and responsiveness) of the IN-QoL. In particular, we correlated the IN-QoL findings with patients’ own ability to address their health quality using the EuroQol-health quality visual analogue scale (EQ-VAS).3 We postulated that there would be a strong correlation between the outcome of the new questionnaire and patient’s self-assessed quality of health.
Methods
Patients
This study is part of the Peripheral Neuropathy Outcome Measures Standardisation (PeriNomS) Study (duration: 7 years; database closed 31 December 2012), an international collaborative effort of 26 neuromuscular centres with special interest in inflammatory neuropathies, located in nine countries (USA, Canada, Spain, Brazil, Italy, France, Belgium, the Netherlands and UK). A total of 264 patients with Guillain-Barre syndrome (GBS), chronic inflammatory demyelinating polyradiculopathy (CIDP), IgM monoclonal gammopathy-related polyneuropathy (MGUSP) and multifocal motor neuropathy (MMN) were included in the study. These patients completed the WHO quality of life scale (WHOQoL BREF),1Sickness Impact Profile,2 EuroQoL scale,3Nottingham Health Profile,4 short form 36-item health survey (SF-36)5 6 8 and Vickrey Peripheral Neuropathy Quality-of-Life Instrument-97.7 The questionnaires were made available using the validated native language versions (English, Spanish, Portuguese, Italian, French, German and Dutch). The obtained data from these questionnaires were stacked creating a large pre-IN-QoL pooled data set.
Eligibility, standard protocol approvals, registrations and patient consents
Eligibility included normal cognitive function, age 18 years or older, fulfilling international criteria for the diagnosis of GBS, CIDP, IgM (preferably anti-MAG+) MGUSP or MMN14–17 having clinical deterioration as judged by the patient and physician, and not receiving immunotherapy for their polyneuropathy at least 2 months before inclusion. Patients were excluded if other causes of polyneuropathy (eg, renal insufficiency, diabetes mellitus) or any other conditions (eg, alcohol abuse>5 IU/day) that might interfere with nervous system and physical functioning (eg, arthritis) were present. All patients gave written informed consent before participation in the study. The local medical ethics committee in each participating centre approved the protocol.
Procedures and statistics
Rasch analysis 1: pre-IN-QoL
The records originating from the six QoL questionnaires were stacked resulting in a total of 324 items in one dataset. First, the data were subjected to a quality control, in which items with >15% missing values and patients with >15% unanswered items were omitted. Second, we randomly created three subgroups within our dataset to improve the item-to-patient ratio. Third, the data in our randomly created three subgroups were checked for misfitting items and disordered thresholds18 using RUMM2030 (Rasch Unidimensional Measurement Models 2030),19 and, if found, these items were stepwise removed. Fourth, the remaining items from all three subgroups were merged resulting in the so-called pre-IN-QoL. For an algorithm regarding this procedure, see figure 1. For additional details regarding the statistical and mathematical background regarding these steps, we refer the reader to the online supplemental document.
Supplementary file 1

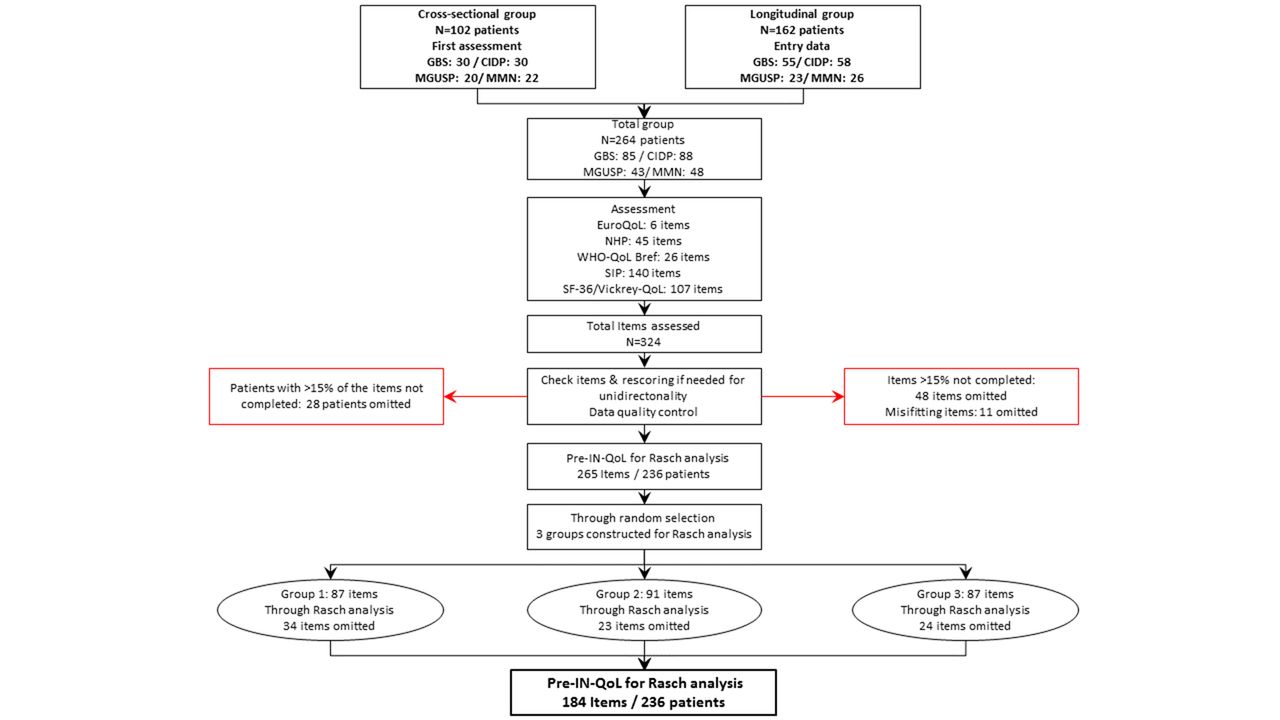
Algorithm for the development of the pre-IN-QoL. First, the data were subjected to a quality control, in which items with >15% missing values and patients with >15% unanswered items were omitted. After the random selection of three groups, an additional 81 items were omitted based on misfitting items/disordered thresholds to establish the pre-IN-QoL questionnaire. CIDP,chronic inflammatory demyelinating polyradiculopathy; GBS, Guillain-Barré syndrome; IN-QoL, QoL questionnaire in inflammatory neuropathies; MGUSP, monoclonal gammopathy-related polyneuropathy; MMN, multifocal motor neuropathy; NHP, Nottingham Health Profile; SF-36, short form 36-item health survey; SIP, Sickness Impact Profile.
Rasch analysis 2: creating the final IN-QoL
The pre-IN-QoL was subsequently analysed through Rasch modelling. This included examining item correlations, item bias based on group factors (age categories (18–50 years vs 51–63 vs 64+ years), gender and diagnosis type (GBS vs CIDP vs MGUSP vs MMN)) and unidimensionality. For an algorithm regarding this procedure, see figure 2. For additional details regarding the statistical and mathematical background regarding these steps, we refer to the online supplemental document. As a final step, knowing that subjects generally are unable to differentiate between more than four response options,20 21 and to establish more uniformity within the final scale, items with five Likert-type response options were rescored resulting in two or three response options for all items taking the distribution of the scores per response item into account.
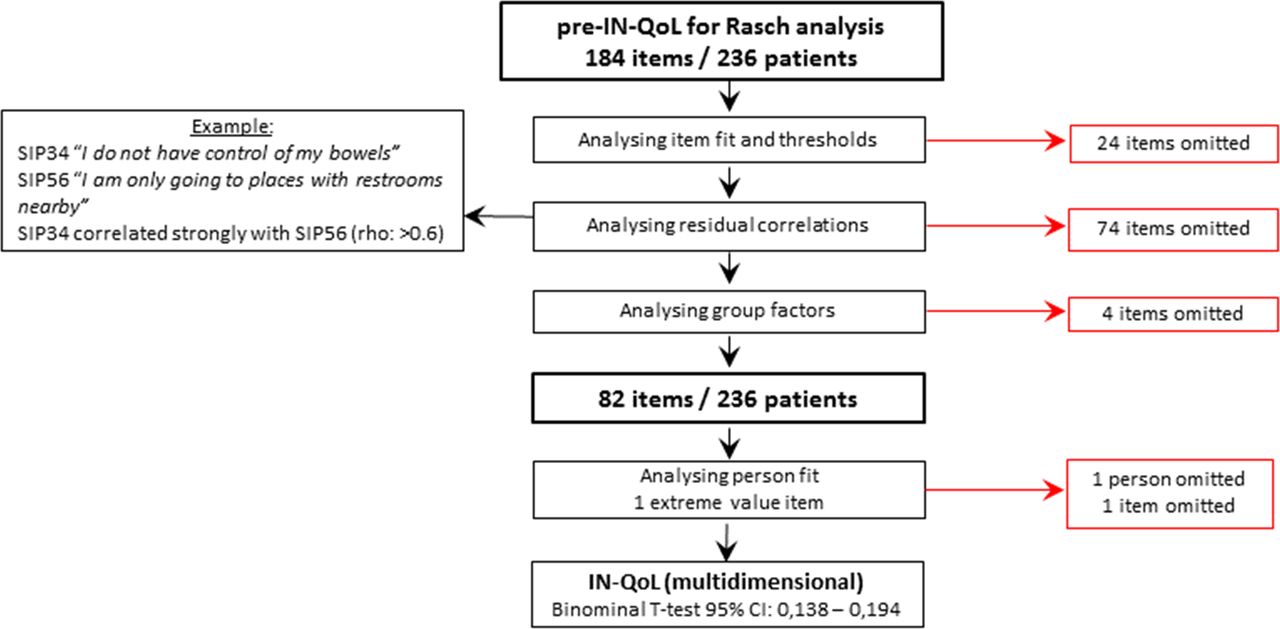
Algorithm for the development of the IN-QoL. The data were subjected to Rasch analysis in a stepwise approach. For additional information and an example on uniform differential item functioning, see online supplementary figure 1. IN-QoL, QoL questionnaire in inflammatory neuropathies; SIP, Sickness Impact Profile.
Supplementary file 5
Validity, reliability and responsiveness
The correlation between the IN-QoL and the EQ-VAS was determined after transforming the IN-QoL to a centile metric scale ranging from 0 to 100 (Spearman’s rho correlation test; validity study). The EQ-VAS ranges from 0 ‘worst imaginable health state’ to 100 ‘best imaginable health state’. To establish the internal reliability, the Person Separation Index (PSI) was determined. In general, a PSI above 0.7 is considered as acceptable, indicating the ability to identify at least two groups of patients.22
Patients completed all six QoL questionnaires at entry and 1 year later, and the final IN-QoL was extracted from these data to determine its responsiveness. For a detailed description of this process, we refer to the online supplemental document and online supplementary figure S3. In short, a personal change is only deemed a clinically important improvement or deterioration if it exceeds±1.96 times the SE, as previously applied.23 24 Similarly, the same calculation was made for the EQ-VAS to determine its responsiveness.
Supplementary file 2
Software
Rasch analyses were performed with the partial credit model as default, using RUMM2030 software.19 Further analyses were undertaken using Stata V.13.0 for Windows XP.
Results
Patients
The basic characteristics of the patients in our initial dataset before any steps were taken are presented in table 1A.
The characteristics of the patients used in our final IN-QoL questionnaire are presented in table 1B.
The characteristics of the patients which were used to determine responsiveness from our longitudinal dataset are presented in table 1C.
Basic characteristics of patients
Procedures and statistics
Rasch analysis 1: creating the pre-IN-QoL
A total of n=264 patients and n=324 were initially collected. After data quality control, 28 patients and 59 items were omitted from the initial dataset, leaving 236 patients and 265 items (figure 1). Additionally, 81 items were omitted from the three randomly selected subgroups based on misfit statistics and/or exceeding fit residual, hence improving the patients-to-items ratio. The remaining items from these three subgroups were joined, resulting in the pre-IN-QoL consisting out of 184 items (see figure 1).
Rasch analysis 2: creating the IN-QoL
The pre-IN-QoL (n=236 patients/n=184 items; see figure 2) mean items’ fit residual showed a decent model fit (mean −0.287, SD 1.169) and persons’ fit residual (mean −0.284, SD 1.180). However, the mean person location was 2.061 (SD 1.218), deviating substantially from the model’s aimed mean value around 0. The item–trait interaction (an indication of the consistency of the item difficulties across the scale) showed a χ2 probability of <0.05, indicating misfit to the Rasch model and potentially measuring non-unidimensional traits.
A total of 24 items with misfit statistics were stepwise omitted (n=160 items remaining). Also, n=74 items’ residual correlations showing local dependency were stepwise removed (n=86 items remaining). An example of a residual correlation is shown in figure 2. Next, potential bias by group factors (age categories, gender and diagnosis type) was analysed, revealing four items with bias (two having uniform differential item function (U-DIF) and one showing non-uniform DIF (NU-DIF) on age-categories, and one item having NU-DIF on diagnosis. An example can also be found in online supplementary figure S1.
Finally, person fit and item fit were analysed, resulting in the omission of one item (extreme value, ceiling effect) and one person (extreme value>2.5 fit residual). The final questionnaire IN-QoL consisted of 81 items in 235 subjects.
A binominal paired t-test showed a proportion of 0.17 of the paired t-test performed falling outside the ±1.96 range with a 95% CI of 0.138–0.194 (indicating multidimensionality).
Additionally, exploratory factor analysis (EFA) was undertaken. With a sample of more than 200 patients (as seen in this study), a scree plot provides a fairly reliable criterion for factor selection.25 This EFA showed two underlying factors, in which the loading was deemed significant if it exceeded 0.3.25 These factors were named ‘mental’ and ‘functional’. Items not loading significantly were classified on their face and content validity between mental and functional after getting consensus between three experts (TD/CGF/ISJM). Two items that had both domains incorporated within their questions were omitted.
This resulted in two subset questionnaires: a mental subset consisting of 59 items and a functional subset consisting of 20 items. These two subsets of items were again subjected to the above-mentioned rigorous Rasch analysis steps, which led to the omission of four items in the ‘mental’ subset and two items in the ‘functional' subset, based on misfitting items and significant residual correlations. Both final two remaining subsets showed a proportion of 0.08 of the paired t-test performed falling outside the ±1.96 range, but with CIs for mental being 0.049–0104 and functional being 0.048–0105, indicating acceptable unidimensionality. The algorithm regarding this procedure is depicted in figure 3.

Algorithm for the factor analysis and subsequent steps for the development of the final IN-QoL. IN-QoL, QoL questionnaire in inflammatory neuropathies.
The final IN-QoL consists of 73 items, with n=55 items as part of the ‘mental’ subset and n=18 items forming the ‘functional’ subset (online supplementary appendix A). For the item–person distribution of the IN-QoL, see online supplementary figure S2.
Supplementary file 3
Supplementary file 4
Validity, reliability and responsiveness
Both the IN-QoL and the mental subset showed good correlation with EQ-VAS (Spearman’s rho 0.72 and 0.71, respectively, with corresponding p-values<0.0001, figure 4). The functional subset showed a low, but significant correlation with EQ-VAS, having a Spearman’s rho of 0.28 and corresponding p-value<0.0001.
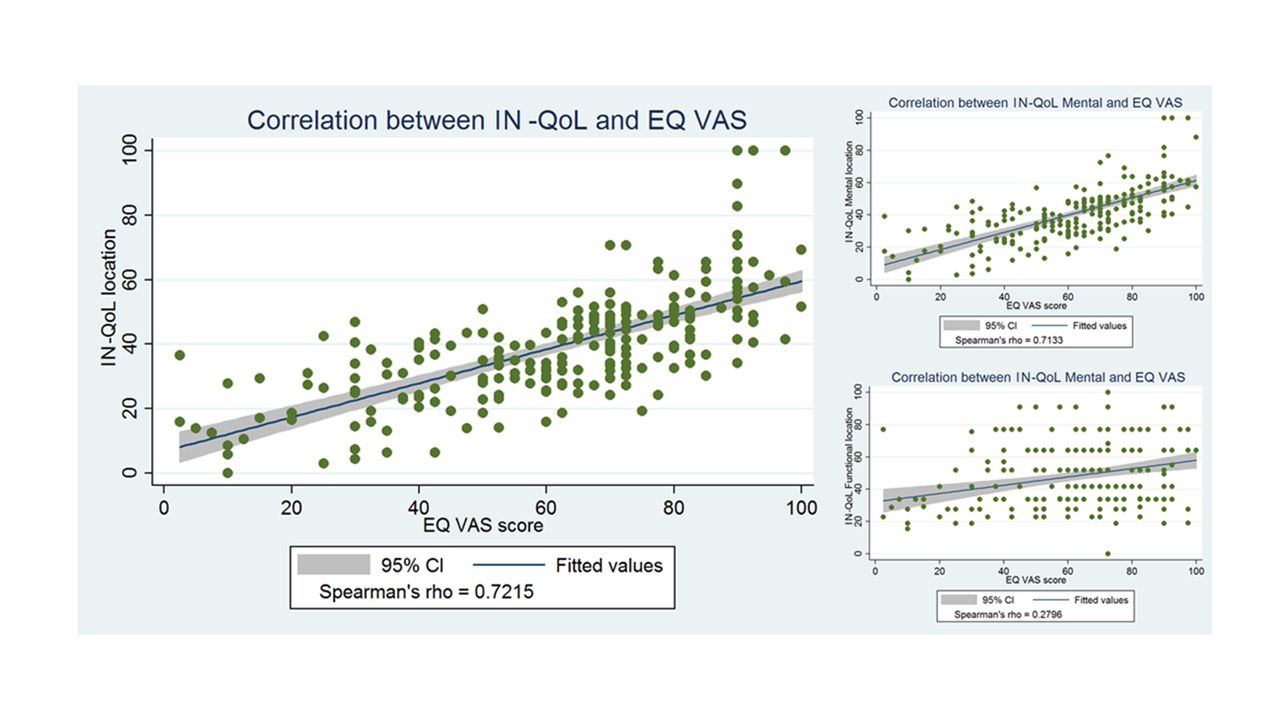
Correlation between IN-QoL (and subsets) and the EQ-VAS. The text block also shows the corresponding Spearman’s rho. EQ-VAS, EuroQol-health quality visual analogue scale; IN-QoL, QoL questionnaire in inflammatory neuropathies.
The questionnaire showed very good internal reliability (PSI 0.94). The subsets, the IN-QoL mental and functional, had a PSI of 0.93 and 0.73, respectively.
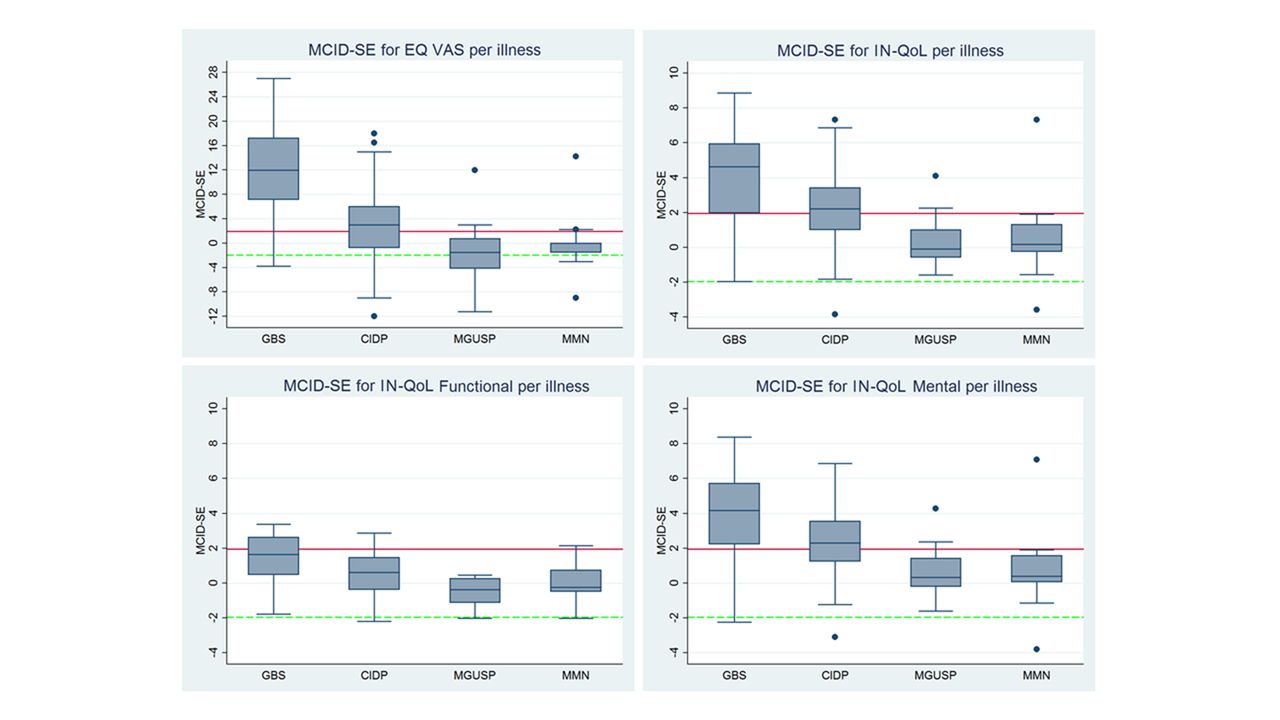
Responsiveness was determined by calculating the minimum clinically important differences related to varying individually obtained SE (MCID-SE, see figure 5) for the IN-QoL, its subsets and the EQ-VAS. Next, we grouped the MCID-SE per illness, as due to the nature of the illnesses, differences in clinical change between them were expected. As can be seen in figure 5, the EQ-VAS and the IN-QoL showed higher responsiveness in GBS and to some extent in CIDP, while MGUSP and MMN did not show clinically important improvement. The IN-QoL mental subset showed near similar responsiveness as the whole IN-QoL scale, while the IN-QoL functional showed minimal clinically important change.

{kind=link}
{kind=link}
![[SP5.jpg]](https://jnnp.bmj.com/content/jnnp/89/3/256/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[SP2.jpg]](https://jnnp.bmj.com/content/jnnp/89/3/256/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
![[SP4.jpg]](https://jnnp.bmj.com/content/jnnp/89/3/256/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
{kind=link}
{kind=link}
The MCID-SE for each instrument grouped by illness. A reference line (solid, red) was added at 1.96 MCID-SE, which is used as a cut-off for clinically important improvement. Also, a reference line (dash, green) was added at −1.96 MCID-SE, which is used as a cut-off for clinically important deterioration. Please note different scaling for the MCID-SE for EQ-VAS (left- top graphic). EQ-VAS, EuroQol-health quality visual analogue scale; MCID-SE, minimum clinically important differences related to varying individually obtained SE.
When looking at the EQ-VAS and the IN-QoL functional, patients with MGUSP and MMN tend to show a stable but clinically unimportant deterioration.
Discussion
We were able to develop the IN-QoL for patients with inflammatory neuropathies (GBS, CIDP, MGUSP and MMN), through a stepwise rigorous methodological approach based on a dataset that emerged from six generally applied QoL measures, collected in a large patient population, and subjected to Rasch analysis. As expected, this new QoL questionnaire, the IN-QoL, showed multidimensionality. After EFA, two underlying factors were detected, leading to two subsets, the so-called IN-QoL mental and IN-QoL functional subsets. These subsets fulfilled all Rasch model requirements of being free of item misfit and bias, without disordered thresholds or local dependency, and showing good internal reliability. The items in the IN-QoL show no bias with regard to the group factor ‘diagnosis type’ meaning that each item functions the same for each illness independently. The IN-QoL is the only Qol measure for inflammatory neuropathies with an interval level of data analysis.
The IN-QoL and its mental subset showed a strong correlation with the EQ-VAS, which is a measurement in which the patient’s own voice is reflected, providing information on their health quality status, thus showing acceptable correlation between a subjective and objective outcome measure, which is becoming more and more important.26–29 The lack of correlation of the functional subset with the EQ-VAS could be due to the fact patients rating their ‘health quality’ mostly based on their mental impact and insecurity rather than their ‘functional’ health.30 Also, for example, in patients with GBS and CIDP, functional recovery does not necessarily imply a good health quality due to residual complaints like fatigue, pain, depression, and so on which is a known common complaint in these patients.30–33
Responsiveness of the IN-QoL and its mental subset was demonstrated through a modern approach to determine a responder by using the MCID-SE method. With this method, the EQ-VAS showed responsiveness as well, however, determining responsiveness of VAS scores through the MCID-SE method may lead to underestimating or overestimating true change.34 Although the pain VAS, which was examined in this study, met the requirements of the Rasch model, its behaviour was not linear as one would expect from interval data. In a recent review, Kersten et al discuss the literature and conclude that the VAS score is in fact not an interval or ratio score, but behaves like an ordinal score.35 We have studied the values of the EQ-VAS in our study population, and it did show some disordered thresholds and a tendency to non-linearity, although far less than the pain VAS in the article by Kersten et al. Therefore, our findings regarding the EQ-VAS responsiveness should be interpreted with some caution, as it might be an overestimation.
Regarding responsiveness, it was to be expected that the patients with GBS (and the patient with CIDP to a lesser extent) would show the most responsiveness, due to a more dynamic course of the disease, as was also previously seen at other levels of assessing outcome in these disorders.23 36 The lack of responsiveness in patients with MGUSP and MMN may be caused by the indolent nature of the illness, the relative short follow-up period of 1 year and/or less impact of treatment medication, although most patients with MGUSP did not receive any treatment, thus expecting a stable or non-improved clinical picture.37 One may argue how responsiveness in each illness should be defined. The concept of being responder should be part of a consensus meeting among experts in the field of inflammatory neuropathies alongside patient’s representatives.38 Aspects like the clinical dynamics (fast vs slow, acute vs chronic) and direction of changes as well as the desire which type of trial to be conducted (improvement or maintenance) are just some pivotal aspects that should be taken into consideration when defining a responder taking into account its clinical relevance.
Our study and the new scale have some limitations. The new scale has not yet been tested prospectively in a larger population with inflammatory neuropathies, and responsiveness has been determined in a relatively small patient population. Currently, a follow-up study (PeriNomS II) is being designed in which we can assess our scale prospectively. Our scale’s cross-cultural validity needs to be investigated as well, which is essential for a questionnaire to be used in international trials.37 39 40 Nevertheless, we believe that the development of this disease-specific, interval-based QoL questionnaire is a first major step in measuring such an important aspect from a patient’s point of view, while not neglecting the proper clinimetric necessities.
Furthermore, we have shown that our patients are quite well capable of assessing their own quality of health by simply asking them to rate it in a direct question (the EQ-VAS). The use of endless lists filled with questions to establish their QoL could be seen as a roundabout way to a very important aspect of a patient’s life, compared with letting patient’s themselves tell us their quality of health.
For future studies in inflammatory neuropathies, we suggest to use the IN-QoL as well as the EQ-VAS. Despite the limitations of overestimating or underestimating the EQ-VAS responsiveness by using the MCID-SE method as discussed above, we still believe that it is important to have an outcome measure in which a patient can rate their own health and to help correlate our scale in future studies with the patient’s own voice regarding their QoL. We would however advise to transform the EQ-VAS to an interval scale before determining its responsiveness in future studies.
By using these two outcome measures, we will be using the best, interval-based, QoL questionnaire for inflammatory neuropathies available so far, and this will also provide the opportunity to correlate the IN-QoL measure with the patient’s own quality of health assessment in a prospective study. Eventually, if there still remains a strong correlation, we might be able to forgo long questionnaires for assessing QoL in future studies all together, and simply ask the patient how they rate their own QoL.
Acknowledgments
The authors thank the patients who took part in this study, the GBS-CIDP foundation international and Talecris Talents program for funding this study and the members of the PeriNomS study group for supporting this project.
References
Footnotes
Contributors Study design: CGF, ISJM. Statistical analysis: THPD. Study recruitment: PeriNomS study group. Final report: THPD, ISJM, CGF.
Funding Study funding: GBS8CIDP Foundation International and Talecris Talents program. The study funding had no role in any of the following: design and conduct of the study, collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript. Only financial support was provided to perform the study.
Competing interests CGF reports grants from the European Union’s Horizon 2020 research and innovation programme Marie Sklodowska-Curie grant for PAIN-Net, Molecule-to-man pain network (grant no. 721841), European Union 7th Framework Programme (grant n°602273), the Prinses Beatrix Spierfonds (W.OR12801), Grifols and Lamepro outside the submitted work. ISJM received funding for research from the Talecris Talents program, the GSB CIDP Foundation International, the European Union 7th Framework Programme (grant n°602273), Grifols and Lamepro. Furthermore, a research foundation at the University of Maastricht received honoraria on behalf of him for participation in steering committees of the Talecris ICE Study, LFB, CSL Behring, Novartis and Octapharma.
Ethics approval METC Erasmus MC.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators A A Barreira, Brazil; D Bennett, UK; L H van den Berg, the Netherlands; P Y K Van den Bergh, Belgium; F Bombelli, France; V Bril, Canada; A Campanella, Italy; E A Cats, the Netherlands; D R Cornblath, USA; R Costa, France; G Devigili, Italy; P A van Doorn, the Netherlands; C G Faber, the Netherlands; J Franques, France; F Gallia, Italy; K C Gorson, USA; R D Hadden, UK; A F Hahn, Canada; R A C Hughes, UK; I Illa, Spain; H Katzberg, Canada; A J van der Kooi, the Netherlands; G Lauria, Italy; J-M Léger, France; R A Lewis, USA; M P T Lunn, UK; I S J Merkies, the Netherlands; S I van Nes, the Netherlands, E Nobile-Orazio, Italy; N C Notermans, the Netherlands; L Padua, Italy; J Pouget, France; L Querol, Spain; J Raaphorst, the Netherlands, MD; M M Reilly, UK; I N van Schaik, the Netherlands; M de Visser, the Netherlands.