
Summary
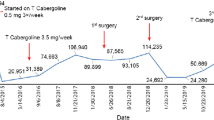
A 44-year-old woman developed acute severe visual field defects and was operated on a macroprolactinoma. Since complete resection of the tumor was not possible, radiotherapy was performed and in addition to hormone replacement therapy, bromocriptine (up to 60 mg daily) was started without however complete normalization of PRL levels. Four years later PRL levels increased to 105 µU/ml despite continuation of dopamin agonist (mesulergin) treatment. As shown by ophthalmological examination and computer tomography there were no signs of regrowth of the pituitary tumor. At that time the patient complained of severe lumbar pain and myelography revealed a tumor mass in the spinal cord (L1–L2). Since the spinal tumor was not removable, laminectomy was performed. Histology and immunohistochemistry demonstrated a metastasis of the prolactinoma. Radiotherapy and bromocriptine in extreme doses (140 mg daily) together with an antiestrogen were not able to improve the neurological deficits (paraparesis) and to lower the PRL levels. This case of a metastasis of a prolactinoma after operation, radiotherapy, and dopamin agonist treatment stresses the importance of close surveillance of patients with prolactinomas without PRL normalization during dopamin agonist therapy and shows for the first time the possibility of ectopic PRL production due to an intradural spinal metastasis.
Similar content being viewed by others

Abbreviations
- ACTH:
-
adrenocorticotropin
- FSH:
-
folliclestimulating hormone
- GH:
-
growth hormone
- Gy:
-
Gray
- L:
-
lumbar
- LH:
-
luteinizing hormone
- µU/ml:
-
microunits per milliliter
- mU/ml:
-
milliunits per milliliter
- PRL:
-
prolactin
- TBG:
-
thyroxine-binding globulin
- TSH:
-
thyrotropin
- T4 :
-
thyroxine
- T3 :
-
triiodothyronine
References
Azria M, Kieckel JR, Lavene D (1979) Contribution a l'étude de l'interaction de la triacetyloleandomycine avec l'ergotamine ou la dihydroergotamine. J Pharmacol 10:431–436
Bassetti M, Spada A, Pezzo G, Giannattasio G (1984) Bromocriptine treatment reduces the cell size in human macroprolactinomas: A morphometric study. J Clin Endocrinol Metab 58:268–273
Breidahl HD, Topliss DJ, Pike JW (1983) Failure of bromocriptine to maintain reduction in size of a macroprolactinoma. Br Med J 287:451–452
Chiodini PG, Liuzzi A, Cozzi R, Verde G, Oppizzi G, Dallabonanza D, Spella B, Silvestrini F, Borghi GP, Luccarelli G, Rainer E, Horowsky R (1981) Size reduction of macroprolactinomas by bromocriptine and lisuride treatment. J Clin Endocrinol Metab 53:737–743
Cohen DL, Diengdoh JV, Thomas DGT, Himsworth RL (1983) An intracranial metastasis from a PRL secreting pituitary tumour. Clin Endocrinol 18:259–264
Dallabonanza D, Spelta B, Oppizzi G, Tonon C, Luccarelli G, Chiodini PG, Liuzzi A (1983) Reenlargement of macroprolactinomas during bromocriptine treatment: report of two cases. J Endocrinol Invest 6:47–50
Eversmann T, Fahlbusch R, Rjosk H, von Werder K (1979) Persisting suppression of PRL secretion after long-term treatment with bromocriptine in patients with prolactinoma. Acta Endocrinol (Kbh) 92:413–427
Feiring EH, Davidoff LM, Zimmermann HM (1953) Primary carcinoma of the pituitary. J Neuropathol Exp Neurol 12:205–223
Flückiger E, del Pozo E, von Werder K (1982) Physiology, Pharmacology and Clinical Findings. Monographs on Endocrinology. Springer, Berlin Heidelberg New York, p 196
Jefferson G (1955) The invasive adenomas of the anterior pituitary. Sherrington Lectures No 3, University Press, Liverpool
King AB (1951) The diagnosis of carcinoma of the pituitary gland. Johns Hopkins Hosp Bull 89:339–353
Kraus JE (1945) Neoplastic diseases of the human hypophysis. Arch Pathol 39:343–349
Labrie F, Ferland L, DiPaolo T, Veilleux R (1980) Modulation of prolactin secretion by sex steroids and thyroid hormones. In: MacLeod RM, Scapagnini U (eds) Central and Peripheral Regulation of Prolactin Function. Raven Press, New York, p 97–113
Landolt AM (1975) Ultrastructure of human sella tumors. Acta Neurochir Suppl 22:94–103
Martin NA, Hales M, Wilson CB (1981) Cerebellar metastasis from a prolactinoma during treatment with bromocriptine. J Neurosurg 55:615–619
Ogilvy KM, Jakubowski J (1973) Intracranial dissemination of pituitary adenomas. J Neurol Neurosurg Psychiatry 36:199–205
Rogol AD, Rosen SW (1974) Prolactin of apparent large molecular size: The major immunoactive prolactin component in plasma of a patient with a pituitary tumor. J Clin Endocrinol Metab 38:714–717
Schwinn G, Dirks H, McIntosh C, Köbberling J (1977) Metabolic and clinical studies on patients with acromegaly treated with bromocriptine over 22 months. Eur J Clin Invest 7:101–107
Suh HK, Frantz AG (1974) Size heterogeneity of human prolactin in plasma and pituitary extracts. J Clin Endocrinol Metab 39:928–935
Thorner MO, Perryman RL, Rogol AD, Conway BP, MacLeod RM, Login IS, Morris JL (1981) Rapid changes of prolactinoma volume after withdrawal and reinstitution of bromocriptine. J Clin Endocrinol Metab 53:480–483
Völker W, Gehring WG, Berning R, Schmidt RC, Schneider J, von zur Mühlen A (1982) Impaired pituitary response to bromocriptine suppression: reversal after bromocriptine plus tamoxifen. Acta Endocrinol (Khb) 101:491–500
Wass JAH, Williams J, Charlesworth M, Kingsley DPE, Halliday AM, Doniach I, Rees LH, McDonald WI, Besser GM (1982) Bromocriptine in management of large pituitary tumours. Br Med J 284:1908–1911
von Werder K, Clemm C (1974) Evidence for “big” and “little” components of circulating immunoreactive prolactin in humans. FEBS Lett 47:181–184
von Werder K, Fahlbusch R, Landgraf R, Pickardt CR, Rjosk HK, Scriba PC (1978) Treatment of patients with prolactinomas. J Endocrinol Invest 1:47–58
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Landgraf, R., Rieder, G., Schmiedek, P. et al. Hormone-active intradural spinal metastasis of a prolactinoma — A case report. Klin Wochenschr 63, 379–384 (1985). https://doi.org/10.1007/BF01731658
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01731658