
Abstract
Background
The characteristics of patients with anticoagulant-associated intracerebral hemorrhage (AAICH) have not been well characterized in a population-based setting.
Methods
We attempted to ascertain all patients with ICH in Greater Cincinnati from May 1998 to July 2001 and August 2002 to April 2003 via retrospective review of ICD-9 codes 430–438.9 at all area hospitals and prospective surveillance at tertiary centers. Cases of ICH without coagulopathy and AAICH were compared with multivariate logistic modeling and survival analysis.
Results
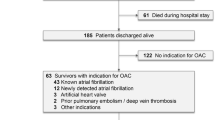
AAICH occurred in 190 of 1041 ICH cases (18%). In multivariate analysis, predictors of AAICH were cerebellar location of hemorrhage (p=0.01) and a history of coronary artery disease (p<0.001), ischemic stroke (p<0.001), atrial fibrillation (p<0.001) and DVT or PE (p<0.001). Relative to other ICH locations, only cerebellar ICH showed an excess risk of anticoagulant-associated hemorrhage (OR 2.2, 95% CI 1.2 to 4.0). In multivariate modeling the only predictor of cerebellar location of ICH was anticoagulation (p<0.001). Patients with AAICH were more likely to die than other ICH patients. The difference in morality occurred by day one (mortality 33.2% vs 16.3%, p<0.001) and remained stable through one year (mortality 66.3% vs 50.3%, p<0.001).
Conclusions
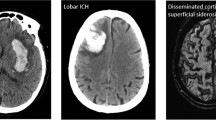
AAICH preferentially affects the cerebellum. Despite its association with amyloid angiopathy, lobar ICH was no more likely to be anticoagulant-associated than deep cerebral ICH. The excess mortality among AAICH patients accures within one day of hemorrhage. Patients with AAICH have a high burden of vascular risk factors. New treatments for AAICH with prothrombotic potential should be evaluated in randomized controlled trials before routine use.
Similar content being viewed by others

References
Smith NL, Psaty BM, Furberg CD, et al. Temporal trends in the use of anticoagulants among older adults with atrial fibrillation. Arch Intern Med 1999;159:1574–1578.
Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology 2006;66:1182–1186.
Flaherty ML, Woo D, Haverbusch M, et al. Racial variations in location and risk of intracerebral hemorrhage. Stroke 2005;36:934–937.
Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Ann Intern Med 2004;141:745–752.
Hart RG, Tonarelli SB, Pearce LA. Avoiding central nervous system bleeding during antithrombotic therapy. Stroke 2005;36:1588–1593.
Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults. National implications for rhythm management and stroke prevention: The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA 2001;285:2370–2375.
Burt VL, Whelton P, Roccella EJ, et al. Prevalence of hypertension in the US adult population. Results from the third National Health and Nutrition Examination Survey, 1988–1991. Hypertension 1995;25:305–313.
Hart RG, Boop BS, Anderson DC. Oral anticoagulants and intracranial hemorrhage. Facts and hypotheses. Stroke 1995;26:1471–1477.
Kase CS, Robinson K, Stein RW, et al. Anticoagulant-related intracerebral hemorrhage. Neurology 1985;35:943–948.
Hart RG. What causes intracerebral hemorrhage during warfarin therapy? Neurology 2000;55:907–908.
Mann DM, Jones D, Prinja D, Purkiss MS. The prevalence of amyloid (a4) protein deposits within the cerebral and cerebellar cortex in Down's syndrome and Alzheimer's disease. Acta Neuropathol (Berl) 1990;80:318–327.
Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med 2004;164:880–884.
Radberg JA, Olsson JE, Radberg CT. Prognostic parameters in spontaneous intracerebral hematomas with special reference to anticoagulant treatment. Stroke 1991;22:571–576.
Neau JP, Couderq C, Ingrand P, Blanchon P, Gil R, and the VGP Study Group. Intracranial hemorrhage and oral anticoagulant treatment. Cerebrovasc Dis 2001;11:195–200.
Flibotte JJ, Hagan N, O'Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology 2004;63:1059–1064.
Franke CL, de Jonge J, van Swieten JC, Op de Coul AA, van Gijn J. Intracerebral hematomas during anticoagulant treatment. Stroke 1990;21:726–730.
Becker KJ, Baxter AB, Cohen WA, et al. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology 2001;56:766–772.
Freeman WD, Brott TG, Barrett KM, et al. Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage. Mayo Clin Proc 2004;79:1495–1500.
Brody DL, Aiyagari V, Shackleford AM, Diringer MN. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care 2005;2:263–267.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Flaherty, M.L., Haverbusch, M., Sekar, P. et al. Location and outcome of anticoagulant-associated intracerebral hemorrhage. Neurocrit Care 5, 197–201 (2006). https://doi.org/10.1385/NCC:5:3:197
Issue Date:
DOI: https://doi.org/10.1385/NCC:5:3:197