Article Text

Abstract
Objective: To investigate the relations between premorbid and current mental ability, mood, and white matter signal abnormalities detected by T2 weighted brain magnetic resonance imaging (MRI) and impairment of balance and mobility in older adults.
Methods: 97 subjects from the Aberdeen 1921 birth cohort underwent brain MRI, evaluation of balance, and measurement of gait speed. White matter hyperintensities detected on T2 weighted MRI scans were rated by three independent raters on three variables: white matter lesions; periventricular lesions; and brain stem lesions.
Results: Decreased gait speed was correlated with impaired visual acuity (p = 0.020), shorter stature (p = 0.008), a lower childhood IQ (p = 0.030), a lower current Raven’s progressive matrices score (Raven score) (p < 0.001), a higher hospital anxiety and depression scale (HADS) score (p = 0.004), and an increased grade of brain stem lesions on MRI. Inability to balance was correlated with Raven score (p = 0.042), brain stem lesions (p = 0.003), white matter lesions (p = 0.003), and periventricular lesions (p = 0.038). Binary logistic regression identified brain stem lesions (odds ratio (OR) 0.22; 95% confidence interval 0.09 to 0.54) and HADS depression score (OR 0.75; 0.58 to 0.97) as the only significant associations with balance. Structural equation modelling detected an association between two latent traits representing white matter disease and an integrating function, respectively.
Conclusions: In this cohort, white matter lesions, periventricular lesions, and brain stem lesions were associated with impaired balance. Current mental ability was strongly related to gait speed. There appears to be a concordance between motor skills and intellect in old age, which is degraded by white matter disease.
- white matter disease
- gait
- balance
- magnetic resonance imaging
- HADS, hospital anxiety and depression scale
- MMSE, mini-mental state examination
Statistics from Altmetric.com
White matter signal hyperintensities are often noted in T2 weighted magnetic resonance images (MRI) of the aging brain1–5 and are associated with recognised vascular risk factors.6–10 The pathogenesis of white matter lesion development is unknown but it may be progressive11 and involve more than one disease process.12 The clinical significance of white matter lesions detected on T2 weighted MRI in a healthy (apparently asymptomatic) elderly population is uncertain. To date, deep/subcortical or periventricular white matter lesions detected on MRI and computed tomography (CT) have been associated with cognitive change,5,13–16 depressed mood,17,18 gait impairment,5,19–21 balance impairment,21,22 and urinary dysfunction23 in older adults. In addition to hemispheric white matter, the brain stem is also well visualised with T2 weighted axial MRI.
Balance and mobility problems often affect older people19,24,25 and are risk factors for falls.26,27 Mobility depends not only on physical functions such as visual acuity, but also on mental state, in particular cognitive impairment and depressed mood.3,17 As white matter lesions are also correlated with cognitive impairment and depression, any influence they may have on mobility could be mediated through cognitive status or mood. Alternatively, impaired mobility, cognition, and low mood may all be associated with some more fundamental processes degraded by white matter lesions. Previously, we found that walking time—a measure of mobility20,25—correlated not only with current functional independence and disease status in old age, but also with childhood IQ.28 Mobility in old age may thus reflect the effects of disease and age related decline on the background of a level determined by central nervous system development in childhood. Childhood intelligence quotient (IQ) may provide a useful index of childhood neurodevelopment.
In this study we investigated the effects of white matter, periventricular, and brain stem lesions on balance and mobility in a birth cohort with childhood IQ data.
METHODS
Sample
We have recruited community dwelling adults in Grampian, who took part in the 1932 Scottish mental survey, to a longitudinal study of brain aging and health, the Aberdeen birth cohort 1921 (ABC 1921) study. Participants were given psychometric tests, scored on the hospital anxiety and depression scale,29 and selected physical measures, including demispan, visual acuity, walking time, and balance. Detailed methods of all but the balance measurement have been described previously.28,30 Ninety seven ABC 1921 participants aged 78 to 79 years (58 male and 39 female; all white) met criteria for brain MRI examination. These were: a mini-mental state examination (MMSE)31 score of > 24, being able to walk, having no clinically diagnosed neurological disease, completing balance and walking assessments unaided, and the absence of any contraindications to MRI or claustrophobia.
Single leg balance ability
We tested single leg balance ability using a method originally devised by Tinetti and colleagues32 and used by others.26,33 Participants were asked to choose the leg upon which they could balance most comfortably and were then instructed to flex the opposite knee until the foot left the floor. They were then asked to balance for as long as possible in this manner. A nurse recorded whether or not participants managed to exceed a period of five seconds. There was only one trial of this test, and balance ability was recorded as success or failure.
Brain imaging
For MRI we used a 1.0 Tesla Siemens Magnetom Impact instrument (Erlangen, Germany). A T2 weighted fast spin echo sequence was acquired in the axial plane with a repetition time of 4000 ms, echo time of 96 ms, and acquisition time of 1 minute 53 seconds. The slice thickness was 5 mm, with an interslice gap of 1.5 mm. MR images were analysed by three observers—ADM (A), SAL (B), and RTS (C)—to facilitate measurements of interobserver variation. White matter hyperintensities were rated using a semiquantitative rating scale devised by Fazekas et al.34 This method yields two separate brain white matter lesion scores: a subcortical/deep white matter lesion score and a periventricular lesion score. Each variable is scored on a four point scale of increasing severity. White matter lesions are scored between 0 (normal), 1 (punctate), 2 (coalescing), and 3 (confluent). Periventricular lesions are scored between 0 (normal), 1 (pencil thin line/caps), 2 (smooth haloes), and 3 (irregular). We extended this lesion scoring method to include brain stem lesions, because there is no difficulty in identifying hyperintense signals on cranial MR images of the brain stem when these are present. Brain stem lesion were scored on a four point scale between 0 (normal), 1 (punctate), 2 (coalescing), and 3 (confluent) (fig 1). A simple mean was calculated for each MRI lesion variable. Two ratings made by observer A were added to ratings made by observers B and C on the same variable. The total for each variable (four scores from three independent observers) was divided by the number of ratings to give mean white matter lesion, periventricular lesion, and brain stem lesion ratings for each participant. This gave an overall mean for each MRI variable.

T2 weighted magnetic resonance images of the pons showing (A) normal appearance (grade 0), (B) punctate change (grade 1), (C) coalescing change (grade 2), and (D) confluent change (grade 3) in the brain stem.
Statistical analyses
Following data checking and inspection, we first tested hypotheses relating single variables to rating scores for white matter lesions, periventricular lesions, and brain stem lesions. As we hypothesised that there are complex interrelations between physical and psychological variables of interest we proceeded to multivariable analyses, using general linear modelling for walking time and logistic regression modelling for balance (individual participants entered as a 0/1 outcome for ability to balance). These models identified those variables with significant associations (effect size is presented as partial η2), after adjusting for the potential confounding effects of other variables. Finally, recognising that these analyses are unable fully to address the likelihood that several of our measures are representative of underlying common factors, we proceeded to structural equation modelling.
The EQS structural equation modelling program was then used to construct and test latent trait models of association among key variables.35 This method is also known as confirmatory factor analysis, which we have used in other clinical areas to demonstrate that several measured variables are indicators of a more general underlying factor (sometimes also called a latent trait). For example, we have shown that the many symptoms of hypoglycaemia experienced by people with type 1 diabetes are indicators of three latent factors (neuroglycopenia, autonomic response, and general malaise),36 and that symptoms of non-psychotic mood problems are indicators of three underlying factors (general psychological distress, anxiety, and depression).37 The same procedures were used to account for associations among white matter lesion measures and measures of cognitive ability, walking, balance, and mood. It was hypothesised that there were two general factors underlying our measured variables: white matter lesions—with white matter lesion, periventricular lesion, and brain stem lesion as indicators of general white matter pathology; and higher integrated functions—with Raven’s progressive matrices score (Raven score), walk time, balance, and hospital anxiety and depression scale (HADS) as correlated indicators of high level integrated brain activity. Additionally we inquired whether these two latent variables were correlated. Two types of relaxation of this strict model were allowed. First, cross loadings were allowed to indicate which measured variables were affected by both latent traits. Second, a few associations were allowed among measured variables in cases where the latent traits and their associations left large residual associations. All scores were organised such that a higher score meant more brain lesions and poorer function (that is, a lower Raven score, a higher depression score, longer walking time, and so on).
RESULTS
Single variable associations with white matter lesions
There was no significant difference detected by analysis of variance between men (n = 58) and women (n = 39) for walking time (p = 0.29) or ability to balance (p = 0.43). A longer walking time was significantly associated with increased brain stem lesions (F = 7.11, p = 0.009; partial η2 = 0.070), but not with white matter lesions (F = 3.33, p = 0.071) or periventricular lesions (F = 2.47, p = 0.12). Several variables correlated with walking time (table 1). Inability to balance was significantly associated with increased brain stem lesions (means, 1.26 v 0.70, p = 0.003), white matter lesions (1.52 v 1.01, p = 0.003), and periventricular lesions (1.56 v 1.18, p = 0.038). Significant differences were noted for some individual psychological and physical variables between those subjects who were able to balance on one leg and those who were not (table 2).
Non-parametric correlation coefficients of walking time with physical and psychological variables in 97 Aberdeen 1921 birth cohort subjects who underwent magnetic resonance imaging
Mean values of variables for those ABC 1921 birth cohort subjects who were able (n = 76) and not able (n = 21) to balance on one leg for five seconds
Multivariate modelling of associations with white matter lesions
Entering those variables that were significant individually into a combined general linear model identified Raven score (F = 13.60, p < 0.001; partial η2 = 0.129) and HADS depression score (F = 4.47, p = 0.037, partial η2 = 0.046) as the only independently significant associations with walking time. Once the Raven score and HADS depression score were adjusted for, brain stem lesions were no longer significant (F = 2.86, p = 0.094), neither was childhood IQ or any of the physical measures. Including ability to balance in the model (F = 13.4, p < 0.001; partial η2 = 0.127) eliminated any significant effect of HADS depression score, but the Raven score remained significant (F = 15.8, p < 0.001; partial η2 = 0.146). Binary logistic regression identified brain stem lesion rating (odds ratio (OR) 0.22, 95% confidence interval (CI) 0.09 to 0.54) and HADS depression score (OR 0.75, 95% CI 0.58 to 0.97) as the only significant associations with balance ability. No other variable significantly improved the model.
Structural equation modelling of white matter lesions
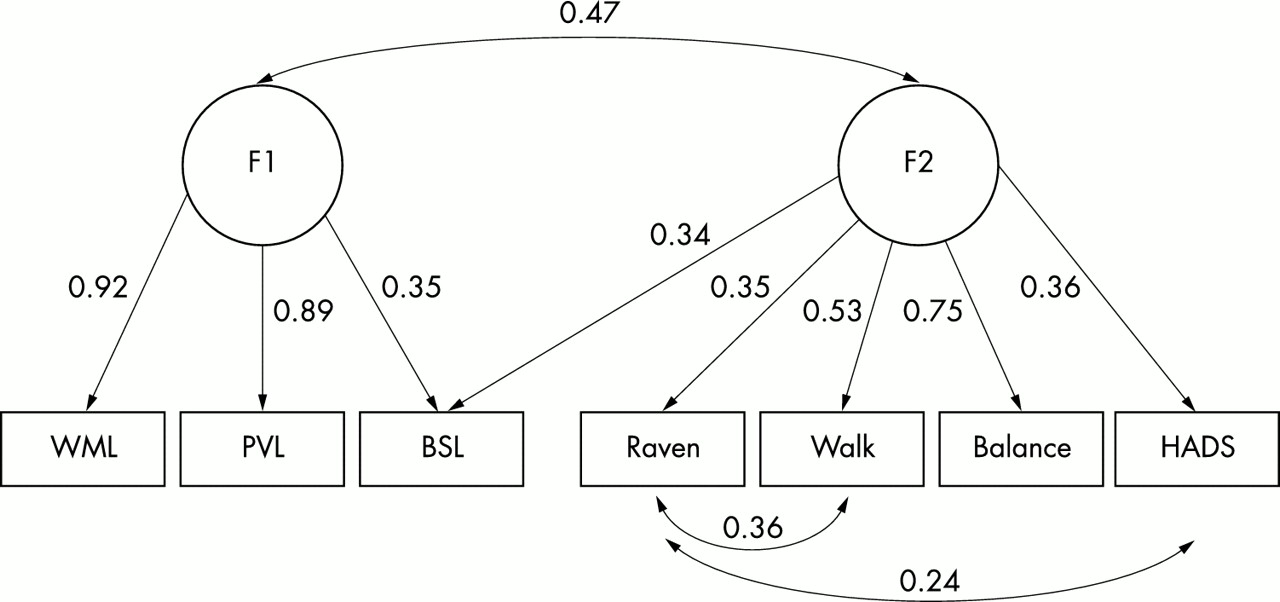
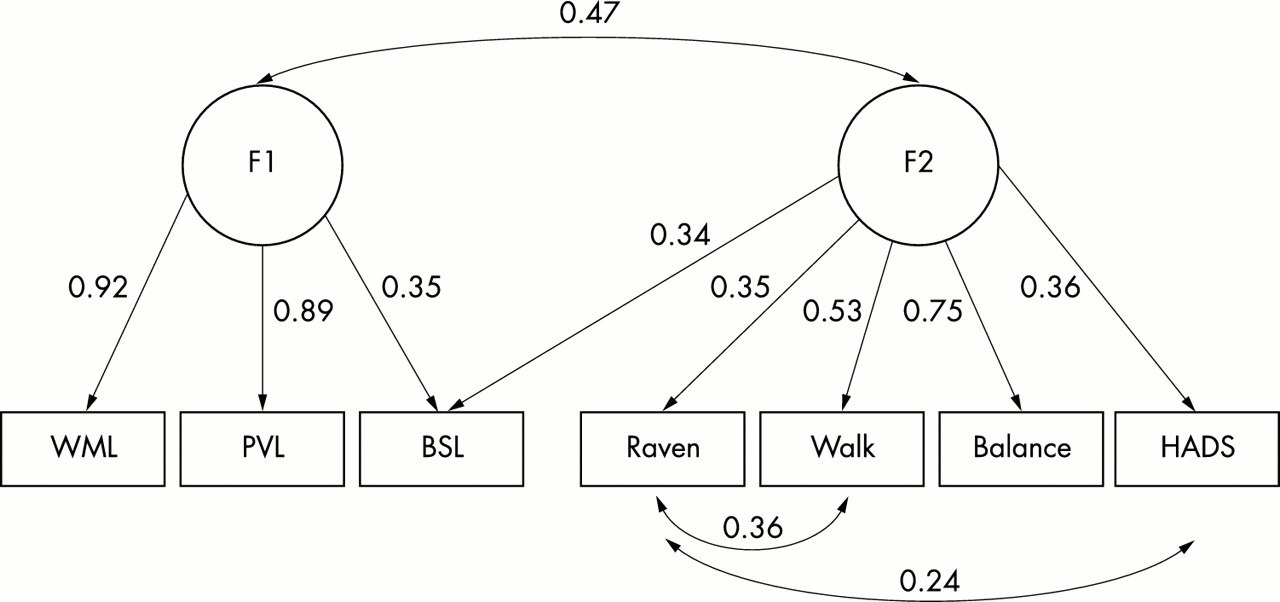
The model that was fitted to the data is shown in fig 2. Following common practice we describe the fit of the model in technical terms and then describe its meaning in a more accessible way. The fit indices were as follows: average of the off-diagonal absolute standardised residuals = 0.04; χ2 = 11.0, df = 10, p = 0.36; Bentler–Bonett normed fit index = 0.95; Bentler–Bonett non-normed fit index = 0.99; comparative fit index = 0.99. The Wald test indicated that none of the paths should be dropped from the model and the Lagrange multiplier test indicated that there were no additional paths that might improve the model significantly.
{kind=link}
{kind=link}
Structural equation model of the relations between magnetic resonance imaging detected white matter lesions (WML), periventricular lesions (PVL), and brain stem lesions (BSL) with fluid intelligence (Raven’s progressive matrices), hospital anxiety and depression score (HADS), walking time, and balance. All correlations reflect a worsening in outcome compared with the latent traits.
The three measures of brain white matter lesions did load significantly on the first latent variable, with white matter lesion and periventricular lesion having especially high loadings. This supports our hypothesis that to some degree the three measures of white matter lesions are indicators of general brain white matter disturbance. Balance and walk time load highly on the second latent trait, with moderate loadings for Raven score and HADS depressions score, confirming the hypothesis of associations among the integrated functions of cognitive and motor ability and mood. Again, this means that these four somewhat disparate seeming variables are indicative of a general underlying organisational capability of the brain. There was a sizeable association between the two latent traits (0.47), suggesting an effect of white matter lesions on higher control functions. The presence of brain stem lesions resulted in further loading on the second latent trait, indicating an additional influence of brain stem lesions on integrated functions, especially balance (the highest loading measure on latent trait 2). Technically, only two correlated residual terms were added to the model. The Raven score had an additional influence on walk time, and depression was associated with lower Raven scores. Adding these two specific paths indicates that these associations were not adequately captured by the variables’ links to the second latent trait. In summary, white matter lesions as a whole had a general deleterious effect on higher motor and cognitive functions, with brain stem lesions having an additional effect on higher functions as a whole.
DISCUSSION
In this sample of older people, those who walked slower were shorter, had worse visual acuity, poorer balance, lower childhood IQ, were of lower current fluid intelligence, and had more depressive symptoms. People who walked slower also had more brain stem lesions on MRI, and these were also associated with poorer balance. Further, balance was impaired in those participants who had more depressive symptoms.
Multivariable modelling of these data identified the key associations. Walking time relates to balance and current fluid intelligence. These two variables explain over 27% of the variance in walking time. However, the causal direction is unclear in this analysis: indeed, there may be some “common cause” that explains the correlation between walking time and balance. Balance, in turn, relates to the number of brain stem lesions seen on MRI and to depressed mood, while other variables—such as height, visual acuity, childhood IQ, and white matter lesions on MRI—are known to correlate with current mental ability. Current mental ability may therefore be acting as a proxy for a basket of influential variables, none of which exerts a large effect on its own, or it may itself be the key factor. Entering these other variables together with balance explains only 17.5% of the variance in walking time. Thus, for Raven’s matrices to be acting as a proxy, other variables not considered in this study but correlating with fluid intelligence are required to explain a further 10% of variance in walking time.
The principal variables that we did not consider were isometric strength and joint deformities.38,39 However, in this relatively healthy sample (most participants were able to balance on one leg for five seconds) these factors are unlikely to explain all the missing variance. Moreover, previous reports have noted a relation between walking time and education,38 similar to our positive correlation with childhood IQ, although not with education itself. In the Rotterdam study, education was highly correlated with mental ability in old age, but not with the presence of white matter lesions on MRI,13 supporting a direct effect of fluid intelligence on walking speed. Similarly, in the cardiovascular health study those upper limb tasks that required more cognitive input (such as buttoning up a shirt) were more strongly linked to white matter lesions and lacunar infarcts than simpler tasks such as finger tapping.3,10 Previously we found that childhood IQ was an independent predictor of functional independence in old age.28 The significant association between childhood mental ability and walking time disappeared when other variables are entered in the model. This is consistent with a hierarchy of locomotor function, progressing from balance through gait speed to more complex tasks such as getting in and out of baths, which are more dependent on mental ability.
The multivariable and logistic regression models suggest important associations between MRI white matter lesions and both physical and psychological variables. Structural equation modelling affords the construction of a model that articulates general and specific associations among MRI and behavioural variables. Two latent traits emerged. One can be thought to represent white matter disease load throughout the central nervous system. The other represents higher processing that integrates complex functions such as problem solving, walking, and balancing; this integrating trait also correlates with depressed mood. Figure 2 shows the strong influence of white matter disease load on this integrating trait. In addition, brain stem lesions have a unique and separate degrading effect. We now hypothesise that childhood IQ and childhood motor ability were similarly integrated in this cohort.
Guttmann and colleagues concluded previously that there is some degree of overlap between the pathophysiological mechanisms underlying cognitive change and impaired mobility, and the relative severity determined by the topographic distribution of white matter lesions.20 Our data are consistent with this hypothesis. However, cross sectional data may overestimate the influence of white matter lesions on mental ability in old age.20
In our study, the severity of white matter lesions in cortical and subcortical regions correlated highly with brain stem white matter lesions. If the latter are determinants of balance, an observed association of cortical and subcortical white matter lesions with mobility may lead to their being spuriously weighted in any causal relation. Areas of hyperintense signal observed within the anatomy of the brain stem could indicate damage to vestibulospinal tracts, lateral lemniscus, medial longitudinal fasciculus, cerebellar peduncles, vestibulocerebellar and numerous cerebellovestibular connections, all of which pass through the brain stem, or to damaged motor fibres in the corticospinal and spinocerebellar tracts.40 Because vestibular fibres and vestibular nuclei are recognised to communicate between regions thought to be associated with balance and mobility,40 it is credible to hypothesise that damage to the brain stem (indicated by MR signal hyperintensity) might affect balance and hence mobility. A similar argument can be proposed for the effect of depressed mood on walking speed. Although not all studies have found a direct association between depressed mood and white matter lesions,41 most show an effect.3,17 Many factors in addition to white matter lesions are certain to influence mood. Brain stem lesions were associated with balance independently of mood.
Although previous reports suggest that subcortical/deep white matter or periventricular lesions may be associated with gait or balance impairments,3,19–21,25 this is the first report to detect an association between T2 weighted MRI brain stem hyperintensities and balance and mobility. This is likely to be generalisable beyond this cohort, as even with a wide variety of semiquantitative methods for white matter lesion rating, remarkably consistent associations with cognitive and physical variables have been found in samples drawn from different populations.5,13–16,19–22,42
The limitations of quantification in this study are not confined to MRI abnormalities. While the collection of valid and reliable psychometric data is well established, the quantification of impaired mobility is less secure. We chose two established, simple, but fairly crude measures of the risk of falling. More detailed assessment may have helped identify exact mechanisms associated with brain stem lesions. For example, assessment of sway and isometric strength would strengthen future studies. Identification of significant associations between variables recognised as risk factors for impaired mobility and falls suggests that the measures used are both sensitive and valid. The choice of Raven’s progressive matrices as a cognitive measure was informed by its suitability in cerebrovascular disease compared with other tests.43 The cardiovascular health study, for instance, chose a modified MMSE and digit symbol substitution test.3 The use of Raven’s matrices avoids confounding by motor or language impairments (secondary to cerebrovascular disease), and functional neuroimaging can demonstrate a wide range of areas involved in its use within both cerebral hemispheres.44 It is thus ideally suited to testing the hypothesis that white matter lesions represent disrupted neuronal connections.
The sample size was adequate to detect medium sized effects, and we were able to explain a fair proportion of variance in the outcome variables. The effects we detected were consistent with those observed in previous larger studies. “Premorbid” mental ability data helps to develop complex causal CNS mechanisms to explain impaired mobility. Working from the original observation of a significant association between childhood IQ and gait speed, we now hypothesise that childhood IQ reflects completeness of brain maturation, is a strong predictor of CNS processing, and integrates complex tasks such as walking. Raven’s matrices are an excellent estimate of the general cognitive factor g,45 another index of CNS processing. White matter hyperintensities are one of many age related factors that degrade CNS processing. Just as in childhood there is neurodevelopmental concordance between motor skills and intellect, we now argue for a similar concordance in old age.
Acknowledgments
The study was supported by the Henry Smith Kensington Estates Charity, Biotechnology and Biological Sciences Research Council, and the Chief Scientist Office of the Scottish Executive.
REFERENCES
Footnotes
-
Competing interests: none declared