Article Text

Abstract
OBJECTIVES To describe the clinical and EEG features of adult patients with very mild absences, late onset generalised tonic clonic seizures, and frequent absence status.
METHODS Patients were referrals to a clinic for epilepsies. They all had clinical assessment and EEG, video EEG, or both for documentation of absences.
RESULTS Of 86 adults with idiopathic generalised epilepsies and EEG/video-EEG documented absences, 13 patients showed similar clinico-EEG features with: (a) “phantom absences” consisting of mild ictal impairment of cognition associated with brief (3-4 s), generalised 3-4 Hz spike/multiple spike and slow wave discharges; (b) infrequent, mainly late onset, generalised tonic clonic seizures, and (c), absence status which occurred in six of them either in isolation or terminating with generalised tonic clonic seizures. None of the patients had myoclonic jerks or photosensitivity. Two patients were father and daughter and another patient had a family history of infrequent generalised tonic clonic seizures.
CONCLUSION It seems that this is an idiopathic generalised epilepsy syndrome in adults which has not been previously recognised.
- epilepsy
- absences
- generalised convulsions
- non-convulsive status epilepticus
Statistics from Altmetric.com
Though considered rare in adults, typical absences with onset in childhood and puberty are reported to persist into adult life in 7%-81% of cases.1-10 The clinico-EEG features of typical absences are syndrome related.8 11 Most patients have syndromes of idiopathic generalised epilepsy such as juvenile absence epilepsy, juvenile myoclonic epilepsy, eyelid myoclonia with absences, perioral myoclonia with absences, and reflex absences.11
In our studies over the past six years, we have identified 86 adults with idiopathic generalised epilepsy and EEG/video-EEG documented typical absences. Thirteen of these patients with remarkably similar clinico-EEG features could not be classified into the known syndromes of idiopathic generalised epilepsy.
Patients and methods
Our methods of studying and classifying patients with epileptic seizures at St Thomas’ Hospital have been previously detailed.7 8 Briefly, all patients with idiopathic generalised epilepsy and typical absences have serial video-EEG recordings and regular follow up. Video-EEG after partial sleep deprivation followed by at least 30 minutes recording on awakening is often performed, especially when prolonged routine video-EEG studies fail to record ictal phenomena. Ictal cognitive impairment during 3-4 Hz spike wave discharges is routinely tested by breath counting during hyperventilation.12
Syndromic diagnosis is established according to strict clinical and video-EEG criteria;11 13 when this is not possible, a seizure symptom categorisation is attempted.14 Patients, mainly children, developing seizures are prospectively studied, whereas those with the established condition are retrospectively investigated from the time of presentation to the onset of the disease with scrutinisation of old medical and EEG records.
The term “phantom absences” is to denote mild typical absences which are inconspicuous to the patient and imperceptible to the observer.8 15
Results
Of 410 consecutive patients older than 16 years with epileptic seizures, 136 (33.2%) had idiopathic generalised epilepsy. Of those 136, 86 (21% of all patients) had typical absences and among them, 13 patients (3.2% of the total or 9.6% of those with idiopathic generalised epilepsy) had phantom absences with generalised tonic clonic seizures.
The table shows the clinical data.
SEX AND AGE
Seven patients were men. The present mean age was 45.6 (SD 18.3); range 22-73; median 42 years).
AGE AT ONSET
The age at onset of phantom absences could not be determined because of the mildness of the symptoms. They are discovered on EEG/video-EEG recommended after the onset of generalised tonic clonic seizures. The mean age of onset of generalised tonic clonic seizures was 31.5 (SD 15) years; range 15 - 56 years; median 28 years). In six patients the mean age at onset of absence status was 32.3 (SD 15.1) years; range 15-56; median 32.5 years).
MEDICAL HISTORY AND POSSIBLE RISK FACTORS FOR EPILEPTIC SEIZURES
These were unremarkable for 12 patients. Patient 7 had a single, brief febrile convulsion at the age of 3 years.
FAMILY HISTORY OF EPILEPTIC SEIZURES
Patient 13 is the father of patient 7. Patient 2 has three nephews, each from a different sister, with idiopathic generalised epilepsy and infrequent spontaneous generalised tonic clonic seizures of late onset. There was no family history of epileptic seizures in the remaining 10 patients.
NEUROLOGICAL EXAMINATION/INTELLECT
This was normal for all.
NEUROIMAGING
All patients had normal high resolution brain MRI.
SEIZURE TYPES
Absences
Phantom absences constituted the most characteristic and consistent feature of these patients. However, none of the patients admitted that absences interfered in their daily life although most of them had demanding professions such as computer programming, civil engineering, and major business and administration. Two of the patients were driving. This was despite mild impairment of cognition consisting of errors and discontinuation of breath counting during the brief generalised spike wave discharges disclosed on video-EEG recordings with breath counting (fig 1, fig 2).7 12 Seven patients retrospectively admitted momentary lack of concentration and forgetfulness which in their opinion was of no practical relevance. Patient 6 was aware of “occasional, very brief episodes of quick flicker of the eyeballs upwards accompanied by a brief lack of concentration”. Also, the daughter of patient 2 retrospectively recognised, after reviewing with her the video-EEG recorded phantom absences with mild eyelid flickering, that her mother occasionally had such events which disappeared after initiation of treatment with sodium valproate.

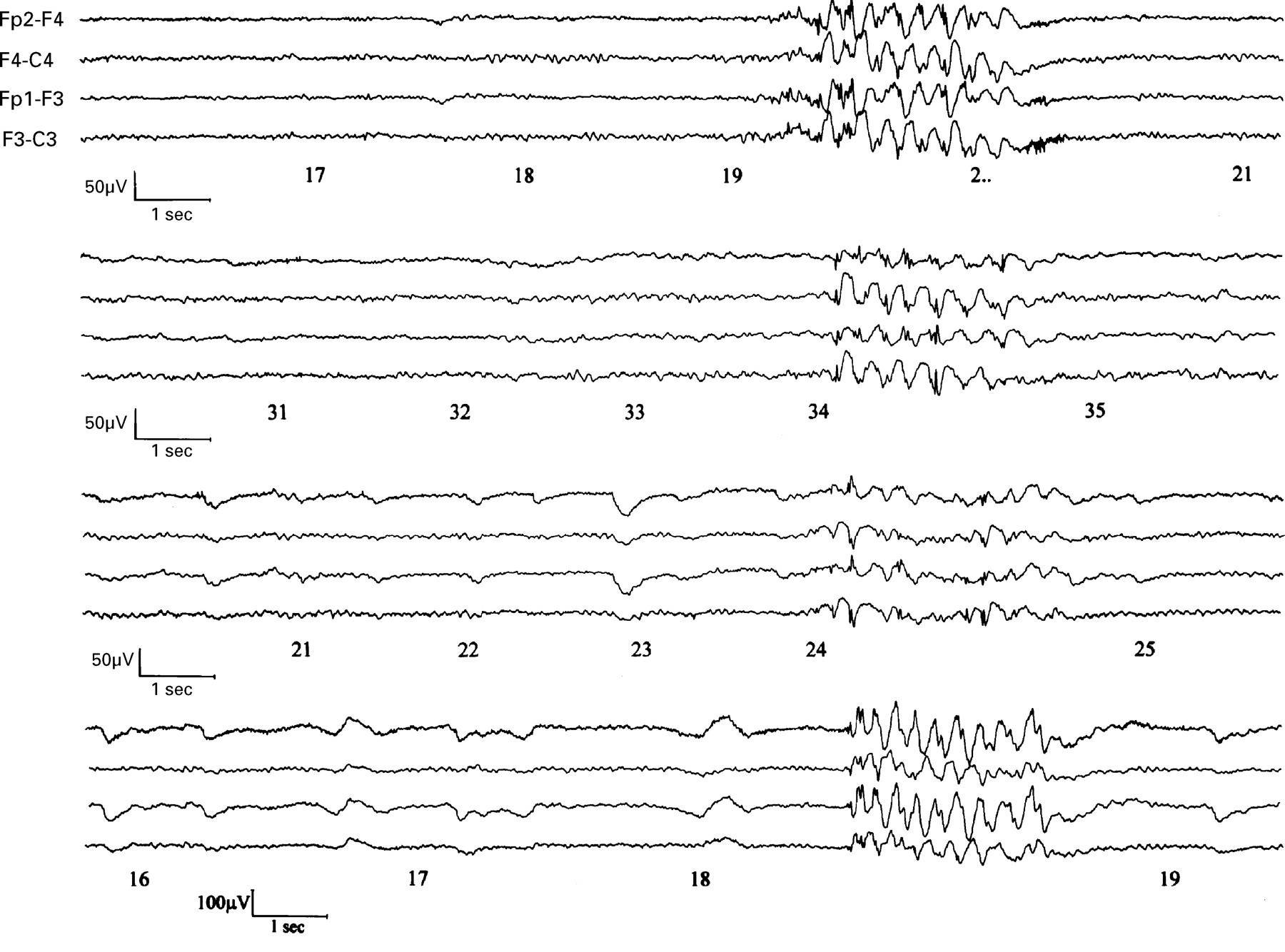
Video-EEG of patient 5 during hyperventilation with breath counting. Generalised discharges of 3-4 Hz spike/multiple spikes and slow waves were associated with ictal delay in pronouncing the next sequential number (39) during breath counting (numbers annotated).

Video-EEG of patients 7, 8, 11, and 10 (consecutively from top down). Generalised discharges of 3-4 Hz spike/multiple spikes and slow waves are associated with ictal delay in pronouncing the next sequential numbers during breath counting (numbers annotated). Only 4 EEG channels are shown.
Generalised tonic-clonic seizures
These are infrequent with eight patients having only one to three generalised tonic clonic seizures in their lifetime. The maximum frequency did not exceed one to two per year. Generalised tonic clonic seizures showed no specific circadian distribution except in two patients in whom they occurred on awakening.
Absence status
Six patients had absence status either in isolation or terminating in generalised tonic clonic seizures (fig 3). Absence status was the first overt clinical manifestation in five patients. The patients were mildly to moderately confused, slow, felt strange, and they were aware of the impending generalised tonic clonic seizures. Two of the patients were able to write down how they felt during the status.15One patient’s (patient 5, fig 1) bizarre experiential subjective ictal manifestations during repeated episodes of absence status have been previously detailed.15 The duration of the status varied even in the same patient from 30 minutes to two days.
{kind=link}
{kind=link}
{kind=link}
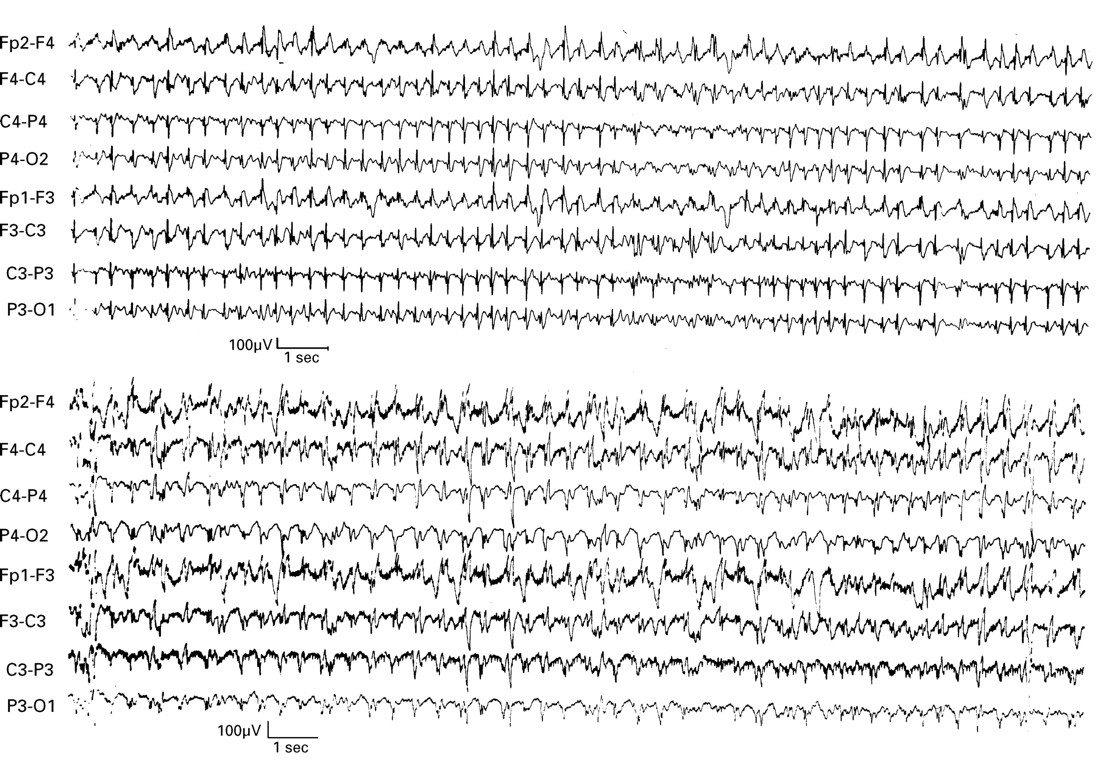
(Upper) Video-EEG of patient 1 during absence status. (Lower) EEG of patient 2 during absence status.
None of the patients had myoclonic jerks.
INTERICTAL AND ICTAL ELECTROCLINICAL MANIFESTATIONS ON EEG OR VIDEO-EEG STUDIES
The background activity was normal in all patients.
Focal paroxysmal abnormalities recorded in six patients consisted of short transient localised slow, sharp waves or spikes, occurring either independently or in association with the generalised discharges.
Generalised discharges were typically brief (two to four seconds) usually lasting for no more than five seconds. They consisted of spike/multiple spikes and slow waves at 3-4 Hz (fig 1 and fig 2). Occasionally, brief fragmentations were seen. Mild cognitive impairment was the only clinical ictal symptom during the generalised discharges and was manifested by hesitation, discontinuation, and errors in breath counting (fig 1 and fig 2). Neither eye or eyelid manifestations or myoclonic jerks were recorded in the long video-EEGs with the exception of two patients (2 and 6) who showed mild ictal eyelid fluttering.
None of the patients was photosensitive.
Absence status (fig 3) showed continuous generalised mainly 3 Hz spike/multiple spike slow wave activity which was interrupted by intravenous diazepam. Clinically, patients were moderately confused, disoriented, and slow in their reaction during the status.
SEIZURE PRECIPITATING FACTORS
Tiredness, sleep deprivation, and alcohol indulgence were reported by four patients. Two of the patients (3 and 5) had an increase of absence status or generalised tonic clonic seizures during weekends and mainly on vacations which one of them attributed to overexcitement. No clear precipitating factors were found in the other seven patients. Generalised tonic clonic seizures occurred on awakening in only two of them.
DIAGNOSIS ON REFERRAL
Absences were unrecognised in all patients on referral despite previous EEG recordings of generalised 3-4 Hz spike/polyspikes and slow waves in eight of them. Furthermore, absence status was misdiagnosed as complex partial seizures in four patients. Eight patients had previous EEGs which showed brief generalised spike wave discharges but ictal impairment of cognition was not recognised because level of consciousness was not appropriately tested.8 11 12 Five patients were already on antiepileptic drugs such as sodium valproate (two patients), phenytoin (three patients), carbamazepine (one patient), and primidone (one patient). One patient (6) had a two day long absence status with a series of generalised tonic clonic seizures soon after 500 mg vigabatrin twice daily was added to his medication of 300 mg phenytoin and 600 mg sodium valproate daily.
TREATMENT AND OUTCOME
The follow up period ranged from six months to seven years (mean 3.5 years). Four patients (1, 2, 7, and 9) are seizure free on monotherapy with sodium valproate. Patient 4 is seizure free on sodium valproate and phenytoin; an attempt to reduce phenytoin resulted in recurrence of seizures and the patient became again seizure free after reinstitution of phenytoin. Patient 13 is seizure free on 225 mg phenytoin daily. Patient 3 continues to have infrequent generalised tonic clonic seizures without absences or absence status despite substituting phenytoin with 1000 mg sodium valproate twice daily. Patient 6 had less frequent and less severe episodes of absence status with occasional generalised tonic clonic seizures on 1000 mg sodium valproate daily. The other five patients refused to take medication. Three of them were lost to follow up (8, 11, and 12) and another one (10) continues to have infrequent generalised tonic clonic seizures. Patient 5 is of interest in that he refused to take medication continuously but could prevent generalised tonic clonic seizures by taking 2000 mg sodium valproate orally after the onset of absence status. He had three to four such episodes of absence status annually without generalised tonic clonic seizures in five years of follow up. In 1996 he started medication with 50 mg lamotrigine twice daily. Absence status increased to 12 within a year and three further episodes occurred within three months of increasing lamotrigine to 100 mg twice daily. All episodes of absence status terminated within 20-40 minutes after ingestion of 2000 mg sodium valproate. However, once a generalised tonic clonic seizure occurred six hours after termination of absence status.
Discussion
That these patients had idiopathic generalised epilepsy is beyond any doubt. They all had generalised seizures, EEG showed generalised discharges of spike/multiple spikes and slow waves, physical state, intelligence, and MRI were normal. The absences were very mild, brief (usually 2-4 s), and caused inconspicuous impairment of cognition which was not clinically disturbing to the patient. Although not classic11 13 they fulfilled the criteria of typical absences with more than 2.5 Hz generalised discharges of spike waves.14 We use the term “phantom absences” because of their clinically elusive and inconspicuous character. Despite minor clinical manifestations during the absence, these patients by definition13 14 had active, clinical absence seizures manifested by mild impairment of cognition as shown with errors and discontinuation during breath counting in video-EEG. It should also be emphasised that the phantom absences in these adults do not represent aborted past childhood or juvenile absences modified by age or medical treatment.16
The age at onset of phantom absences in these patients was practically undetermined and their detection was the result of special attention and specifically oriented examination with video-EEG in our department.
The other cardinal characteristic of this idiopathic generalised epilepsy is the occurrence of infrequent, late onset generalised tonic clonic seizures without consistent circadian distribution and specific precipitating factors. The mean (32 years) and median (28 years) age at onset of generalised tonic clonic seizures was far higher than in any other idiopathic generalised epilepsy syndrome.7
One or more episodes of absence status occurred in half of the patients. It is difficult to explain the high frequency of absence status in these patients with so brief and mild absences and infrequent generalised tonic clonic seizures. It is possible that under the influence of not fully understood precipitating factors, phantom absences may cluster and evolve into absence status facilitated by either the lack of or inappropriate treatment.
Patients are not photosensitive and never had myoclonic jerks either in association or independently of the absences.
The diagnosis of idiopathic generalised epilepsy in these patients is unquestionable but it is impossible to classify them among any of the recognised or the newly described syndromes of idiopathic generalised epilepsy.11 13 Certainly, the clinico-EEG features of these 13 patients were markedly different from the four syndromes with typical absences proposed by the Commission.13 Absences in idiopathic childhood absence epilepsy and juvenile absence epilepsy are characterised by severe impairment of consciousness, longer duration, and frequent automatisms which are never mild to escape detection and recognition.7-9 11 13 Myoclonic absence epilepsy is a cryptogenic syndrome of generalised epilepsy with typical absences characterised by impairment of consciousness and rhythmic myoclonic jerks.17 None of our patients had typical absences of the severity of idiopathic childhood absence epilepsy, juvenile absence epilepsy, or myoclonic absence epilepsy in childhood or adolescence.
Juvenile myoclonic epilepsy is the only syndrome recognised by the Commission,13 in which absences may be as inconspicuous as in our patients.18 However, the cardinal symptom of myoclonic absence epilepsy is myoclonic jerks on awakening which none of our patients had. Furthermore, absence status rarely occurs in juvenile myoclonic epilepsy and onset of generalised tonic clonic seizures is usually around in the midteens.
Even the newly described syndromes of idiopathic generalised epilepsy with absences such as eyelid myoclonia with absences19 and perioral myoclonia with absences20 are notably different from phantom absences. Eyelid myoclonia with absences is a predominantly photosensitive epileptic syndrome with absences unequivocally betrayed by pronounced eyelid myoclonia. Perioral myoclonia with absences is characterised by perioral myoclonia. None of the 13 patients had evidence of such absences or photosensitivity.
Genton et al 21 reported that among 253 consecutive cases of idiopathic generalised epilepsy, 32 (15.4%) patients had rare generalised tonic clonic seizures with generalised spike wave discharges in the interictal EEG. Onset of generalised tonic clonic seizures was from childhood to adulthood and there was no particular circadian distribution of the generalised tonic clonic seizures. Although clinical absences were never reported by such patients or by their families it is possible that some of them had phantom absences which escaped diagnosis because they were not tested for mild impairment of cognition. It is also possible that some of the cases with benign grand mal epilepsy in adults22 belong to this group although in only three of the 59 reported patients generalised spike wave discharges were recorded.22
In conclusion, we present clinico-EEG findings of 13 patients with idiopathic generalised epilepsy manifested by phantom typical absences, infrequent mainly late onset generalised tonic clonic seizures, and absences status in six of them. Irrespective of whether this is a previously unknown syndrome as we propose or a continuum among the idiopathic generalised epilepsy as others23 may prefer, its recognition is important for diagnosis and management. This is important particularly in view of the late onset generalised tonic clonic seizures which are usually associated with structural brain lesions and the absences and absence status which in adults are often misdiagnosed as complex partial seizures.7
Acknowledgments
The Special Trustees of St Thomas’ Hospital and Epilepsy Research Foundation are gratefully acknowledged for their grants for our studies on the classification of epilepsies. Without the technical expertise of Mr Shaun Rowlinson, Mrs Sue Sanders, Mrs Ann Baker, Mrs Christine Carr, and Mr Peter Walsh the video-EEG recordings would not be possible.
References
Clinical details