Article Text

Abstract
OBJECTIVE To determine the effectiveness and safety of prophylactic antiepileptic agents in the management of acute traumatic head injury.
METHODS Systematic review of randomised controlled trials identified using MEDLINE, EMBASE, CINAHL, Dewent Biotechnology abstracts, and specialised databases of randomised controlled trials, by searching reference lists and contacting investigators.
RESULTS Ten eligible randomised controlled trials were identified, including 2036 patients. The pooled relative risk (RR) for early seizure prevention was 0.34 (95% confidence interval (95%CI) 0.21–0.54); based on this estimate, for every 100 patients treated, 10 would be kept seizure free in the first week. Seizure control in the acute phase was not accompanied by a reduction in mortality (RR=1.15; 95% CI 0.89–1.51), a reduction in death and neurological disability (RR=1.49; 95% CI 1.06–2.08 for carbamazepine and RR=0.96; 95% CI 0.72–1.26 for phenytoin) or a reduction in late seizures (pooled RR=1.28; 95% CI 0.90–1.81). The pooled relative risk for skin rashes was 1.57 (95% CI 0.90–2.75).
CONCLUSIONS Prophylactic antiepileptic drugs are effective in reducing early seizures, but there is no evidence that treatment with such drugs reduces the occurrence of late seizures, or has any effect on death and neurological disability. Insufficient evidence is available to establish the net benefit of prophylactic treatment at any time after injury.
- head injuries
- epilepsy, post-traumatic
- anticonvulsants
Statistics from Altmetric.com
Seizure activity in the early post-traumatic period after head injury may cause secondary brain damage as a result of increased metabolic demands, raised intracranial pressure, and excess neurotransmitter release. Although concern about the adverse effects of early seizure activity has been the primary therapeutic rationale for the prophylactic use of antiepileptic drugs in the management of acute traumatic head injury, recent pathophysiological studies have shown that some antiepileptic drugs may also have neuroprotective effects. For example, phenytoin has been shown to reduce neuronal damage in animal models and in vitro models of hypoxia. The neuroprotective effect of phenytoin may be mediated by a voltage dependent blockade of sodium channels.1 2 These results suggest that antiepileptic drugs may have a beneficial effect on neurological outcome after head injury that is independent of their effect on seizure activity. On the other hand, antiepileptic drugs have unusually narrow therapeutic margins and well documented toxicity, even in neurologically stable patients. The most common adverse effects are impaired mental and motor function and serious side effects including deaths from haematological reactions have also been reported.3 The injured brain’s response to antiepileptic drugs is such that toxic effects could be more pronounced, and neurological recovery may be delayed. A survey of board certified neurosurgeons in 1973 showed that 60% used antiepileptic drugs prophylactically in patients with head injury.4 We have been unable to identify any contemporary reports of current practice variations in this area although wide variations in other aspects of the early management of patients with head injury have been documented.5 Recent recommendations by the task force of the Brain Trauma Foundation suggest the use of early antiseizure prophylaxis in patients with head injury, although the guidelines acknowledge that this is an area of considerable clinical uncertainty.6
Whether prophylactic use of antiepileptic drugs is associated with favourable neurological recovery, either independent of seizure activity or associated with it, has not been previously reviewed. To examine the effectiveness and safety of antiepileptic agents in the treatment of acute traumatic head injury, we conducted a systematic review of randomised controlled trials. We estimated the “number needed to treat”7 to provide clinically interpretable measures of benefit and non-fatal adverse effects.
Methods
INCLUSION CRITERIA
The review included all controlled trials of antiepileptic agents, in which study participants had a clinically defined acute traumatic head injury of any severity, and subjects were assigned to treatment or control (placebo controlled or no drug) groups on the basis of random or quasirandom allocation. Trials in which the intervention was started more than eight weeks after injury were excluded. There were no language restrictions.
IDENTIFICATION OF RELEVANT TRIALS
MEDLINE (1966–August 1996) was searched using a combination of the Cochrane Collaboration optimally sensitive search strategy for randomised controlled trials,8 and head injury related terms in conjunction with the MeSH subject heading “epilepsy, post-traumatic” and free text terms using wild card characters: (epileps* or convuls*) near (posttraum*or post-trauma* or inju*). The resulting citations were examined and citations potentially relevant to this review were retrieved in full and reviewed further. EMBASE (1982–November 1996) was searched using a similar approach as well as the BIDS Index to Scientific and Technical Proceedings (1981–November 1996), CINAHL (1982–October 1996), and Dewent Biotechnology abstracts. The following specialised registers of controlled trials were searched: the United Kingdom based Intensive Care National Audit and Research Centre’s database, the database of the Cochrane Stroke Group and Cochrane Epilepsy Group, and the Cochrane Library. Several additional journals and conference proceedings were hand searched. The reference lists of all relevant articles identified were checked. A letter was sent to the first author of all reports to ask for further information on the published report and asking them to assist in identifying any further trials which may have been conducted by them, or other investigators. We also contacted pharmaceutical companies who manufacture antiepileptic agents, asking them to identify any further published or unpublished trials and we contacted the National Institute of Neurological Disorders and Stroke, Epilepsy Division, National Institute of Health, United States. Eligibility was determined by reading the reports of possible trials, and correspondence with the trialists. We independently scored all trials meeting the inclusion criteria on quality, using a five point scale in which a maximum score of 5 indicated high quality of randomisation and allocation concealment, and the minimum score was 1.9Disagreement was resolved by discussion.
Summary of trials of prophylactic antiepileptic drugs in head injury that met the inclusion criteria
DATA EXTRACTION
For each report, we gathered information on the participants, the antiepileptic drug used, and the treatment regimen; duration of follow up, early seizures (seizures occurring in the first week after injury), late seizures, non-fatal adverse effects (skin rashes, neurobehavioural changes), neurological disability, and death. As data are often selectively reported, a list was sent to all trialists of the outcomes of interest. These additional data, that may have been recorded but not featured in the public report, were requested. We sought data in simple categorical form and we did not extract time to death, time to seizure, or cumulative seizure data.
A PRIORI HYPOTHESES
Before analysing the results, we identified hypotheses concerning underlying differences in the studies which might explain heterogeneity. These were quality of allocation concealment, drug type, and drug dose. Studies with poor allocation concealment have previously been shown to yield stronger estimates of treatment effectiveness than studies with adequate allocation concealment,10 and it would be reasonable to expect that drug type and drug dosage may be associated with treatment effects.
STATISTICAL METHODS
Relative risks and 95% confidence intervals (95% CIs) were calculated for each trial on an intention to treat basis. As in several trials a high proportion of initially randomised patients were found to be ineligible, our calculation included only eligible patients. Including all patients would have resulted in a misleading weight and precision in the meta-analysis. Heterogeneity between trials was tested using a χ2 test, in which p⩽0.05 was taken to indicate significant heterogeneity.11 As long as statistical heterogeneity did not exist for dichotomous data, summary relative risks and 95% CIs were calculated using a fixed effects model. Where the source of heterogeneity could obviously be related to allocation concealment, drug type, or drug dose, we stratified the analyses on that dimension. Numbers needed to treat were calculated for seizure prevention and for non-fatal adverse effects; these were also expressed as occurrence per 100 patients treated.
Results
The combined search strategy yielded a total of 6982 citations. On review, 83 citations were identified as possible reports of trials and the full text articles were reviewed further. Ten eligible controlled trials were identified including 2036 randomised patients (table). A further trial12-14 was initially included, but later excluded when translation from the Czechoslavakian showed that patient allocation was not random or quasirandom. Eligible trials included four unpublished trials, one of which had been reported as an abstract that included no usable outcome data.15 Those responsible for each of the unpublished trials were contacted and asked to provide data for the review, but at the time of writing these were still unavailable for inclusion. The remaining trials were published in 13 different trial reports: Glotzner et al 1983,16 McQueenet al 1983,17 Harris et al1984,18 Young et al 1983,19-21Bertch et al 1985,22 Temkin et al and Dikmen et al 1989–9123-25(these three reports are considered together as Temkin (1990) in the rest of the paper), Pechadre et al 1991,26and Manaka 1991 and 1992.27 28 The quality scores of the trials ranged across all possible values (1–5). None of the trial reports had sufficient information to complete quality scoring according to our instrument. Authors of three trials were able to supply additional information, but quality scoring for the remaining trials is not complete.
SEIZURE PREVENTION
The number of patients with early seizures (within the first week after injury) in each group was available for four trials, representing 890 randomised subjects. Figure 1 shows the summary relative risks. There was no statistical heterogeneity between trials (χ2=3.52; df=3; p=0.95). The studies all showed similar treatment effects with the exception of those of Young et al,19-21 which showed no treatment effect. The pooled relative risk for early seizure prevention was 0.34 (95% CI 0.21–0.54; p=0.000). On the basis of this estimate, the number needed to treat to keep one patient seizure free in the acute phase is 10. Alternatively, for every 100 patients treated with prophylactic antiepileptic drugs, 10 patients would be kept seizure free in the acute phase.

Summary relative risks (95% CIs) for patients kept seizure free in the first week (early seizures) and to the end of follow up (late seizures).
For late seizures, there was significant heterogeneity between studies (χ2=16.44; df=5; p=0.005) and therefore a summary relative risk was not calculated. Figure 1 shows the relative risks for the individual studies. The lack of blinding in the report by Pechadreet al 26 and different drug type in that by Glotzner et al,16 may account for some of the heterogeneity in the findings. A summary relative risk based on the remaining four studies was 1.28 (95% CI 0.90–1.81; p=0.046), with χ2=0.14 (df=3; p=0.990).
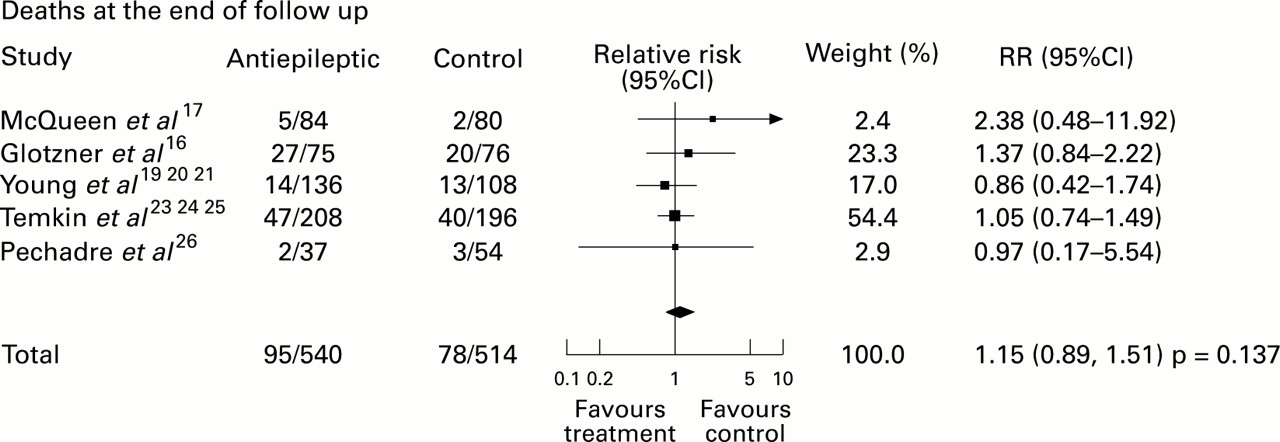
DEATH AND NEUROLOGICAL DISABILITY
Mortality data (from all causes at the end of follow up) were available from five studies, representing 1054 randomised patients (fig2). There was no statistical evidence of heterogeneity (χ2=2.02; df=4; p=0.75). No beneficial effect of prophylactic antiepileptic drugs was evident for mortality (pooled RR=1.15; 95% CI 0.89–1.51; p=0.137). Neurological disability on the Glasgow coma outcome scale was available for two trials (Glotzneret al 16 and Temkin (1990)) neither of which showed a beneficial effect. Glotzner et al 16showed a substantial trend towards a worse outcome (persistent vegetative state or death v rest) in the treatment group (RR=1.49; 95% CI 1.06–2.08; p=0.183) and Temkin (1990) showed no effect on neurological recovery (severe disability, vegetative state, or death v rest) (RR=0.96; 95% CI 0.72–1.39; p=0.755). The conflicting findings of these studies is possibly related to the different drug type used; Glotzner et al 16used carbamazepine, and Temkin (1990) used phenytoin.

{kind=link}
{kind=link}
Summary relative risks (95% CIs) for death at the end of follow up.
ADVERSE EFFECTS
Only two trials documented the occurrence of skin rashes and both reported an increase of skin rashes in patients taking the antiepileptic drugs (Temkin (1990): RR =1.39; 95% CI 0.77–2.49 and McQueen et al 17: RR=4.76; 95% CI 0.57–39.88; pooled RR=1.57; 95% CI 0.90–2.75; p=0.046). Based on the pooled relative risk, for every 100 patients treated, four will develop skin rashes. Only one trial (Temkin (1990)) documented adverse neurobehavioural effects; this trial showed cognitive impairments in the patients receiving antiepileptic drugs.24 The authors did not report an overall effect measure. Five trialists responded to our request for additional outcomes. All of these trialists, except Temkin, stated that no adverse effects or functional outcomes additional to that in the published report were documented.
Discussion
Although the randomised controlled trial is the optimum method of assessing the effectiveness of healthcare interventions, many interventions remain unsupported by trials and rest instead on pathophysiological explanations or conventional wisdom. Randomised controlled trials have been used in recent reviews of the effectiveness of the prophylactic use of antiepileptic drugs in traumatic head injury; on the basis of seizure end points, these reviews recommended that antiepileptic drugs may be used prophylactically in high risk patients for the first week after injury.6 29 In this systematic review, we sought end points that may be proxies of neurological recovery in addition to seizure end points, and found no further support for the use of antiepileptic drugs. The seizure control in the acute phase (pooled RR= 0.34; 95% CI 0.21–0.54) was not supported by a reduction in mortality (pooled RR=1.15; 95% CI 0.89–1.51) or a reduction in death or persistent vegetative state (RR=1.49; 95% CI 1.06–2.08 for carbamazepine; or RR=0.96; 95% CI 0.72–1.26 for phenytoin). The occurrence of late seizures was not reduced by antiepileptic prophylaxis at any time. There were insufficient data to examine non-fatal adverse effects, with the exception of a trend towards an increased risk for skin rashes (RR=1.57; 95% CI 0.90–2.75). From the information available, the net benefit of treating 100 patients would be that 10 would be kept seizure free in the acute phase, and four may develop skin rashes. However, the period of antiepileptic prophylaxis extended well beyond the first week in all the included trials. Therefore the number of patients who develop skin rashes if given only one week of treatment, as recommended by the Brain Trauma Foundation, may be less than this estimate. The wide confidence intervals of the pooled relative risks for death and neurological disability indicate that the true net benefit of prophylactic treatment is still in doubt.
The quality scores of the studies are difficult to interpret because of missing data. A high loss to follow up was reported in the largest study (Temkin(1990)). Much of this was due to early exclusion of patients found to be ineligible. As the postrandomisation assessment of eligibility was blinded, and the exclusions in the treatment and control group were similar, we did not consider that the estimate of treatment was biased. None the less, we ran the analyses both including and excluding the prerandomisation losses, and found no substantial difference in the estimate of the pooled RR when using the available data. Although considerable effort was made to obtain and include in the systematic review the data from the four unpublished trials, these data were unavailable for inclusion. Because of the problem of publication bias, the estimates presented in this systematic review may be overoptimistic.
Conclusions
Despite the reduction in early seizures associated with prophylactic treatment after acute traumatic head injury, and the hypothesised association of seizures with secondary brain damage, there is no evidence that prophylactic antiepileptic drugs used at any time after head injury, reduce death and disability. Insufficient evidence is available to establish the net benefit of treatment at any time after head injury.
Acknowledgments
This research was funded by the NHS R and D Maternal and Child Health Programme. There are no conflicts of interest.