Article Text

Abstract
OBJECTIVES To evaluate the long term sequelae of perimesencephalic subarachnoid haemorrhage (PMSAH).
METHODS Twenty one consecutive patients were studied. All patients were examined by CT, angiography, MRI, multimodal evoked potentials, and transcranial Doppler sonography. All relevant clinical data during hospital stay and outcome at discharge were obtained by reviewing the charts. Long term follow up was evaluated by reviewing the outpatient files and dedicated outpatient review. Patients were specifically questioned about their perceived recovery, residual complaints, and present occupational status.
RESULTS Apart from the initial CT confirming the diagnosis of PMSAH all other examinations disclosed no abnormalities. None of the patients developed any complications during hospital stay, and all patients were discharged in good clinical condition and without neurological deficits. At long term follow up 62% of the patients had residual complaints consisting of headaches, irritability, depression, forgetfulness, weariness, and diminished endurance. Apart from four patients who had already retired before the PMSAH, only seven of the remaining 17 patients (41%) returned to their previous occupation, whereas nine patients (53%) retired from work and one man became unemployed. One patient had a recurrence of PMSAH 31 months after the first event.
CONCLUSION PMSAH can have considerable long term psychosocial sequelae, and may also recur. Prognosis may not be as good as previously reported.
- perimesencephalic subarachnoid haemorrhage
- negative angiography
Statistics from Altmetric.com
The most common cause of subarachnoid haemorrhages (SAHs) are aneurysms, which can be easily demonstrated on angiography in most cases.1 However, in 15% to 20% of the cases no causative source of SAH can be shown and the angiogram is negative.1 2 Several studies gave evidence that patients with SAH and a negative angiogram have a substantially better prognosis than patients with aneurysmal SAH.1-5 The rate of subsequent bleeding varies between 2% and 5%. From the pattern of bleeding on CT a particular subgroup of angiogram negative patients with SAH could be identified with blood confined to the perimesencephalic cisterns. Since the first description in 19856 various studies on perimesencephalic subarachnoid haemorrhage (PMSAH) have reported a good short term outcome and an excellent prognosis.2 4 6-10 It is regarded as a benign form of SAH as recurrent haemorrhage has never been found during follow up.
By contrast with these findings we report our series of PMSAH and the unique case of a patient who had recurrent PMSAH 31 months after the first event.
Materials and methods
Twenty one consecutive patients with the diagnosis of PMSAH were studied in this series. All relevant clinical data during hospital stay were obtained by reviewing the charts. Clinical grades were assessed according to the grading system of Hunt and Hess. Brain CT was performed to confirm diagnosis, and at least one subsequent CT study was obtained in every patient to rule out complications such as formation of hydrocephalus.
A four vessel digital subtraction cerebral angiography with multiple views was performed in all patients, and in most of the patients a reangiography 6 to 10 weeks later. To rule out an extracranial source of the haemorrhage an MRI of the neck and spinal cord was obtained. All patients were examined by multimodal evoked potentials and by daily transcranial Doppler sonography. Outcome at discharge was again obtained by reviewing the charts.
Long term follow up was evaluated by reviewing the outpatient files, and all patients were specifically reviewed to evaluate the degree of subjective recovery, residual complaints, and present occupational status.
Results
Eleven of the patients were men and 10 were women. The mean age at presentation was 55.8 years (range 25 to 82 years). All patients were alert and classified Hunt and Hess I or II. Initial CT indicated a PMSAH and subsequent CT studies showed resorption of blood. None of the patients developed hydrocephalus. Cerebral angiography was negative in all patients. An MRI of the neck and spine did not show an extracranial source of the haemorrhage in any of the patients. None of the patients developed cerebral vasospasm, brainstem dysfunction, or seizures. All patients were discharged from hospital in good clinical condition without neurological deficits.
In 14 patients angiography was repeated 6 to 10 weeks later and the results were negative in all cases.
Mean duration of follow up was 23 months (range 5 to 41 months). Eight patients (38%) considered themselves recovered and completely well.
Thirteen patients (62%) had residual complaints such as headaches, irritability, depression, forgetfulness, weariness, and reduced endurance. Apart from four patients who had already retired before their PMSAH, only seven of the remaining 17 patients (41%) returned to their previous occupation. Nine patients (53%) retired from work and one man became unemployed (table).
Only one of the patients had a history of rebleeding. In this study we document for the first time the unique case of a patient with recurrent PMSAH.
Case report
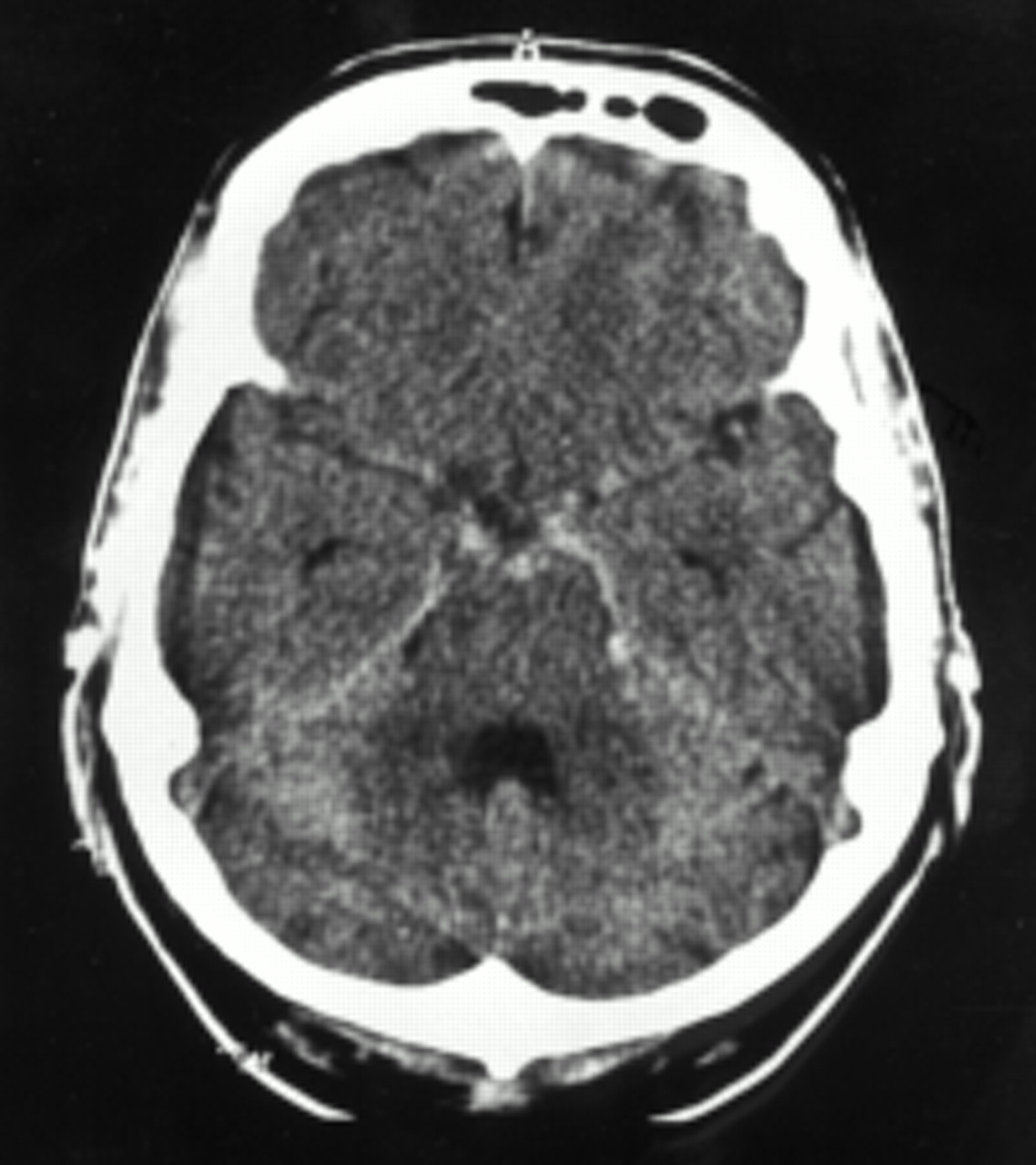
In 1996 a 48 year old man presented with sudden onset of severe headaches, neck pain, and nausea. There was no loss of consciousness and no history of hypertension. The patient had a normal neurological examination, and he was classified Hunt and Hess grade I. Lumbar puncture was positive confirming the suspected diagnosis of SAH, and CT on the day of the onset of symptoms showed extravasated blood in the perimesencephalic subarachnoid space (fig 1). Four vessel angiography with multiple views did not show any causative source of the bleeding, and angiograms of the external carotid arteries were normal as were MR images of the head and neck. The patient was treated conservatively and recovered rapidly without developing any complications. He was discharged in good clinical condition 14 days after the PMSAH. A second angiography 10 weeks later was negative; however, his capacity for work had not reached the premorbid level, he fatigued easily, and his concentration was poor.

After positive lumbar puncture a non-contrast enhanced CT shows extravasated blood in the perimesencephalic subarachnoid space.
Thirty one months later the patient again experienced sudden severe headaches, and CT showed a recurrent PMSAH (fig 2). A subsequent, third four vessel angiogram was again negative, and MRI of the head and neck showed no abnormalities. Somatosensory evoked potentials and brainstem auditory evoked potentials were normal and daily transcranial Doppler sonographic examination showed no vasospasm. The patient was treated conservatively, recovered, and was discharged from hospital without neurological deficits 13 days after the onset of the symptoms.
{kind=link}
{kind=link}
Non-contrast enhanced CT shows appearance of recurrent PMSAH 31 months after the first event.
Discussion
Aneurysms are the most common cause of SAH but in 15% to 20% of the cases the angiogram is negative. This might be due to occult aneurysms concealed by haemorrhage, vasospasm, thrombosis, inadequate technique, or small size of the lesion.1 2 Therefore a second angiography is recommended after an initial negative study. The frequency of detected aneurysms on further angiograms varies between zero and 21% but most of the causes of bleeding remain unresolved.1 9 The prognosis of these angiogram negative patients with SAH, however, is regarded as good and rates of subsequent bleeding are as low as 2% to 5%.1-5 A subgroup of patients accounting for about half of the patients with SAH with negative angiograms are seen to have a perimesencephalic distribution of blood.2 4 6 Perimesencephalic subarachnoid haemorrhage is regarded as a different entity from SAH because aneurysms are unlikely to be found. Nevertheless, the performance of an angiography is obligatory in cases of PMSAH as the likelihood of finding an aneurysm in patients with the perimesencephalic pattern of SAH is not zero.2 11 By contrast with angiogram negative non-PMSAH, in which a reangiography is mandatory, it is commonly accepted that repeated angiography in PMSAH can be omitted after a negative first angiogram. There are several reports of negative reangiographies in cases of PMSAH1 2 4 6-8 10 12 13and these findings match the results in our series (table). Goergenet al found a significant association between isolated PMSAH and negative angiography (p<0.005) and a specificity of PMSAH for negative angiography of 100%.7
There is much speculation about the source of bleeding in cases of PMSAH. Van Gijn et al deduced from the fact that angiography was negative and no subsequent haemorrhage occured in follow up that the source of the bleeding was non-aneurysmal.6 Assumed causes of these haemorrhages have been either rupture of fine arterial vessels8 9 13 or a venous tear.2 6 8 9 The assumption of a non-arterial source is supported by the fact that patients with PMSAH have been surgically explored but in no case has an aneurysm or vascular malformation been found.2 Despite all theories the exact anatomical source of PMSAH remains unknown. To rule out an extracranial source of the haemorrhage, we performed an MRI of the neck and spinal cord in our patients but all examinations were normal.
Since the first description in 19856 various studies on PMSAH have reported a good short term outcome and an excellent prognosis.2 4 6-10 By contrast with aneurysmal SAH all reported patients with PMSAH were alert and classified Hunt and Hess I or II. These findings are confirmed by our series of 21 patients. In accordance with other series none of our patients developed cerebral vasospasm as shown by daily transcranial Doppler sonographic examination. Although some authors report enlargement of the ventricles4 or formation of symptomatic hydrocephalus requiring shunting in some of their cases,6 8 we never saw any development of hydrocephalus in any subsequent CT studies. As in other series we did not find seizures. From these points of view we agree that short term outcome can be regarded as good.
A striking discrepancy between our and previous series, however, concerns the appearance of recurrent bleeding. Perimesencephalic subarachnoid haemorrhage is generally distinguished from SAH and regarded as a benign form as recurrent haemorrhage has never been found at follow up.2 4 6-10 Schwartz and Solomon reviewed the literature in 1996 and concluded that of the 169 patients reported who had PMSAH, none had experienced subsequent bleeding after a duration of follow up ranging from 8 to 51 months.2 By contrast with these findings we report the unique case of a patient who had recurrent PMSAH 31 months after the first event. In accordance with other patients with PMSAH neurological examination was normal and four vessel digital subtraction cerebral angiography was negative on the three occasions when it was performed. To exclude a dural fistula, visualisation of the external carotid artery and MRI of the head and neck were performed to rule out an extracranial source of the haemorrhage. Both examinations were repeatedly negative. Vasospasm was not seen, neither was dysfunction of the brainstem as multimodal evoked potentials were normal. The patient was discharged from hospital without neurological deficits 13 days after the onset of symptoms. So far, short term outcome has proved to be good, but the conception of PMSAH as an event occurring only once in a lifetime has to be revised.
Long term psychosocial outcome after PMSAH is also not as excellent as generally believed. Brilstra et al measured quality of life by means of the sickness impact profile and reported that patients showed less dysfunction than controls and concluded that a perimesencephalic haemorrhage does not reduce quality of life or capacity to work.14 However, despite having no neurological deficits, one third of the patients in the series of Canhao et al 4 felt unwell, and complained of headaches, neck pain, postural vertigo, and depressive symptoms. Although most of their patients returned to their previous occupations, a few retired from work. In our series residual complaints were frequent with only one third of the patients feeling completely well. About two thirds complained of headaches, irritability, depression, forgetfulness, weariness, and lessened endurance. The consequences of PMSAH for occupational status were even more serious. Apart from four patients who had already retired before the PMSAH, only seven patients returned to their previous occupation. Nine patients (53%) retired from work and one man became unemployed. These findings imply that long term oucome may not be as good as suggested and that PMSAH may have a major psychological impact.
References
Clinical summary of 21 patients presenting with perimesencephalic subarachnoid haemorrhage