Article Text

Abstract
OBJECTIVE To test the hypotheses that visuoperceptual and attentional ability are disproportionately impaired in patients having dementia with Lewy Bodies (DLB) compared with Alzheimer's disease (AD).
METHODS A comprehensive battery of neuropsychological tasks designed to assess working, episodic, and semantic memory, and visuoperceptual and attentional functions was given to groups of patients with DLB (n=10) and AD (n=9), matched for age, education, and mini mental state examination (MMSE), and to normal controls (n=17).
RESULTS Both patient groups performed equally poorly on tests of episodic and semantic memory with the exception of immediate and delayed story recall, which was worse in the AD group. Digit span was by contrast spared in AD. The most striking differences were on tests of visuoperceptual/spatial ability and attention. Whereas patients with AD performed normally on several subtests of the visual object and space perception battery, the DLB group showed substantial impairments. In keeping with previous studies, the AD group showed deficits in selective attention and set shifting, but patients with DLB were more impaired on virtually every test of attention with deficits in sustained, selective, and divided attention.
CONCLUSIONS Patients with DLB have substantially greater impairment of attention, working memory, and visuoperceptual ability than patients with AD matched for overall dementia severity. Semantic memory seems to be equally affected in DLB and AD, unlike episodic memory, which is worse in AD. These findings may have relevance for our understanding of the genesis of visual hallucinations, and the differential diagnosis of AD and DLB.
- dementia with Lewy bodies
- Alzheimer's disease
- memory
- attentional
Statistics from Altmetric.com
Dementia with Lewy bodies (DLB) is a common cause of dementia. As many as 12%-36% of patients with a clinical diagnosis of AD meet neuropathological criteria for a diagnosis of DLB, which makes DLB the second commonest cause of dementia in elderly people.1 2Numerous synonyms have been used to categorise dementia associated with Lewy bodies, including diffuse Lewy body disease (DLBD),3senile dementia of Lewy body type (SDLT),2 4 and Lewy body variant of Alzheimer's disease (LBV).5 We have chosen to use the term DLB as recommended by a recent consensus group.1 Pathologically DLB is characterised by Lewy body formation in the cerebral cortex, brain stem nuclei (substantia nigra and locus coeruleus), and components of the basal forebrain cholinergic system (BFCS).6 The clinical features of DLB include a cortical dementia with fluctuating confusion, spontaneous parkinsonism, sensitivity to neuroleptic drugs, and psychiatric manifestations especially well formed and recurrent visual hallucinations early in the course of the disease.7-9
By comparison with Alzheimer's disease (AD), relatively little is known about the neuropsychological deficits in DLB. A retrospective study of a few pathologically verified cases suggested that the pattern of cognitive impairment in DLB is different from the one in AD, with greater deficits in visuospatial function in the cases of DLB.5 Subsequent studies of patients with a clinical diagnosis of probable DLB have also shown significantly worse performance on tests of visuospatial function,10-12 but these studies all suffer from the weakness of having used tests such as clock face drawing or block design that confound visuoperceptual, visuospatial, and praxic ability. Data regarding attentional and executive function in DLB are more controversial. This is a potentially important issue since it has been suggested that cholinergic depletion, and resultant attentional dysfunction, underlies the tendency to fluctuations and hallucinations which characterise DLB.2 6 Whereas Hansen et al 5 found greater impairment on the FAS test of verbal fluency in DLB than in AD, the same group of researchers later reported equivalent impairment in groups of DLB and patients with AD.13 Likewise, Gnanalingham et al 10 found no difference on this test, or on the Nelson card sorting test. The only study that has used more theoretically motivated tests of attentional and executive ability14 15 found greater impairment in DLB on a computerised test of spatial working memory, but this study did not include tests of perceptual ability. Semantic memory, which is impaired fairly consistently early in the course of AD16 has not been investigated in DLB.
Attentional function has been extensively evaluated in AD (for reviews see Perry et al 16 and Hodges and Patterson17). It is clear that not all components of attention are equally impaired early in the course of the disease. Selective attention, especially the ability to inhibit inappropriate responses, seems to be particularly vulnerable in the very mild stages of AD, with deficits in divided attention following in its wake, whereas sustained attention is the most resistant component.16 As far as we are aware, there have been no reported studies that have included tests of a range of attentional abilities in DLB. The pattern of attentional deficits in DLB remains, therefore, an open question.
Although impairment in attentional function has been suggested to underlie the hallucinations in DLB, we hypothesised that deficits in perceptual processing might have a key role either alone or in combination with the attentional disorder.
The aim of this study was to compare well matched groups of patients with DLB and AD using a comprehensive battery of neuropsychological tests designed specifically to evaluate a range of attentional and visuoperceptual abilities as well as semantic and episodic memory. We predicted that patients with DLB would have comparatively greater deficits on perceptual or attentional tasks than the patients with AD. In keeping with prior studies, we expected to find more impairment of episodic memory in AD. As semantic memory breakdown is one of the hallmarks of AD it is important to see if deficits can be found in other dementias.
Methods
SUBJECT GROUP
Thirty six subjects participated in the study: nine with AD; 10 with DLB; 17 normal controls (NC). The patients with AD were chosen from patients undergoing evaluation at the University of Cambridge Neurology unit. The diagnosis of probable AD was made by a neurologist according to the criteria developed by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS), and the Alzheimer's Disease and Related Disorders Association (ADRDA).18 The patients with DLB were chosen from the same unit and from the Psychiatric Services for the Elderly in Cambridgeshire and represent all suitable patients with DLB presenting over a 12 month period. The diagnosis of DLB was according to the clinical criteria of the consortium on DLB International workshop.1 All patients with DLB had had well formed visual hallucinations within 1 month of assessment but were not hallucinating at the time of their examination, whereas none of the patients with AD experienced visual hallucinations. As discussed more fully below, we had hoped to test patients with AD with and without hallucinations and during the course of the study screened some hallucinating patients with AD, but all had mini mental state examination (MMSE) scores below 10 and were unable to comply with the test battery. Subjects were excluded if they had a history of known or suspected cerebral ischaemic event, alcohol misuse, head injury, or other major physical illness. The patients with AD and those with DLB were matched for age and dementia severity according to the MMSE (table1). The control subjects were selected from the MRC-CBU subject panel. The three groups did not differ significantly in age (F (2,35)=1.5; p>0.5), or education (F (2,33)=1.6; p>0.5) was between patients with AD and controls. All testing was performed in the subjects' homes and was spread over two sessions each of about 2 hours. The project was approved by the local research ethics committee.
Demographic details and MMSE scores (mean (SD)) of the patient groups and controls
NEUROPSYCHOLOGICAL TESTS
Memory
Verbal short term memory (STM)—The forward and backward digit span test from the WAIS-R was used.
Episodic memory—The logical memory subtest of the Weschler memory scale-revised19 was used, which involves listening to two short passages with immediate recall and 30 minute delayed recall. Both stories were administered, each containing 25 elements, and the score was taken as the mean of the two stories. To test recognition memory we used the shortened 25 item version of the recognition memory test (RMT) for words and faces.20
Semantic memory—Subjects were given the stringent 30 item graded naming test,21 and a shortened version of the category fluency subtest of the Hodges and Patterson semantic battery22 in which subjects had to produce as many examples as possible in 2 minutes from each of the following categories: animals, fruits, and household items.
Perceptual and spatial abilities
The following subtests from the visual object and space perception (VOSP) test were used.23
Figure-ground discrimination—In this screening test subjects were asked to indicate whether an “X” was present or not. The X is degraded and presented within a visually complex background (maximum score=20).
Fragmented letters—In this test of perceptual ability, subjects were asked to identify letters that increased in their level of degradation (maximum score=20).
Silhouette identification—Subjects were asked to name or identify silhouettes of animals (n=15) and objects (n=15) viewed from unusual angles.
Object decision—In this test of stored structural description, subjects were asked to choose the real object from amongst three foils. All were presented as silhouettes and the objects were graded in difficulty (maximum score=20).
Cube analysis—This required subjects to count the number of cubes in three dimensional structures consisting of cubes in which some cubes were not visible (maximum score=10).
Tests of attention and executive function
Sustained attention—We used the elevator counting task from the test of everyday attention (TEA)24 in which subjects are required to count strings of tones, ranging from 3 to 14, from a recorded tape (maximum score=7).
Auditory selective attention—This was assessed using the elevator counting with distraction task, also from the TEA,24 which is similar to the first task except that subjects are required to count a string of low tones while ignoring high pitched tones (maximum score=10).
Visual selective attention—This was tested using the map search task from the TEA24 in which subjects have to identify target symbols from competing and irrelevant distractors on a map. This is a timed task of selective attention with minimal memory component (maximum score=80).
Stroop test—This version25 of the classic paradigm measures the interference effect that a more automatic process, in this case reading words, has on a more effortful process. Subjects are initially required to read out words (red, green, blue, and tan) that are printed in ink of an incongruous colour. The critical interference task (colour-word, CW) is then to read another list of colour names, but this time to name the colour of the ink in which the word is printed. The first task of reading words produces an automatic response that is reflected in the increased time taken on the second task (maximum score=112).
Dual performance test of Della Sala et al26 —This is a timed paper and pencil task of divided attention that has been modified from the visual tracking-digit span test of Baddeley et al.27It consists of two tasks that are each performed on their own before being performed simultaneously. Firstly, the subject's digit span is determined. Then, strings of digits at the subject's span are given continuously for 2 minutes with the proportion of correct strings being recorded. The second task involves crossing out boxes linked to form a trail on a sheet of A4 paper and the number of boxes crossed in 2 minutes is calculated. The dual performance task is then performed with the subjects repeating digit spans while simultaneously crossing boxes on a trail for 2 minutes. In performing the dual task, subjects may use different strategies by concentrating on one task at the expense of the other and so any measure of the effect of divided attention between the two tasks must, therefore, take into account data from both single tasks as performed alone and simultaneously (see below).
The shortened Nelson version of the Wisconsin card sorting test28 —This was employed as a test of strategy formation and task switching.
Letter fluency—This was included as a task requiring intact attentional and executive abilities. Subjects were asked to generate as many words as possible beginning with the letters F, A, and S (excluding proper nouns) each within 1 minute. The score was taken as the total number of correct responses.
ANALYSIS
The results were analysed using analysis of variance (ANOVA) with post hoc pairwise Tukey's test to explore significant main effects.
Results
MEMORY
Table 2 shows that forward digit span was well preserved in the AD group with a significant, but mild degree of impairment in DLB (NC=AD>DLB). For reverse digit span the degree of deficit was greater in both patient groups, but still with a difference between AD and DLB (NC>AD>DLB).
Mean (SD) neuropsychological test results for the patient groups and controls
On all measures of episodic memory there were highly significant main effects of group with post hoc analyses showing that both AD and DLB groups were impaired relative to controls. The two patient groups were equally impaired on both the words and faces versions of the RMT, but the AD group were significantly worse on immediate and delayed recall of stories (NC>DLB>AD). Comparison of the percentage recall of the stories after a delay is particularly revealing: whereas the controls retained 78%, the DLB group recalled 28% and the AD group a mere 4%.
On tests of semantic memory the degree of impairment in the two patient groups was equivalent. For both the graded naming test and the total number of items correctly produced on the category fluency test there were highly significant group differences with an equivalent degree of impairment in the two patient groups (NC>AD=DLB). The performance of the groups on tests of episodic and semantic memory is illustrated in figs 1 and 2.

(A) Mean correct forward and backward digit spans and (B) mean score for immediate and delayed logical memory story recall.
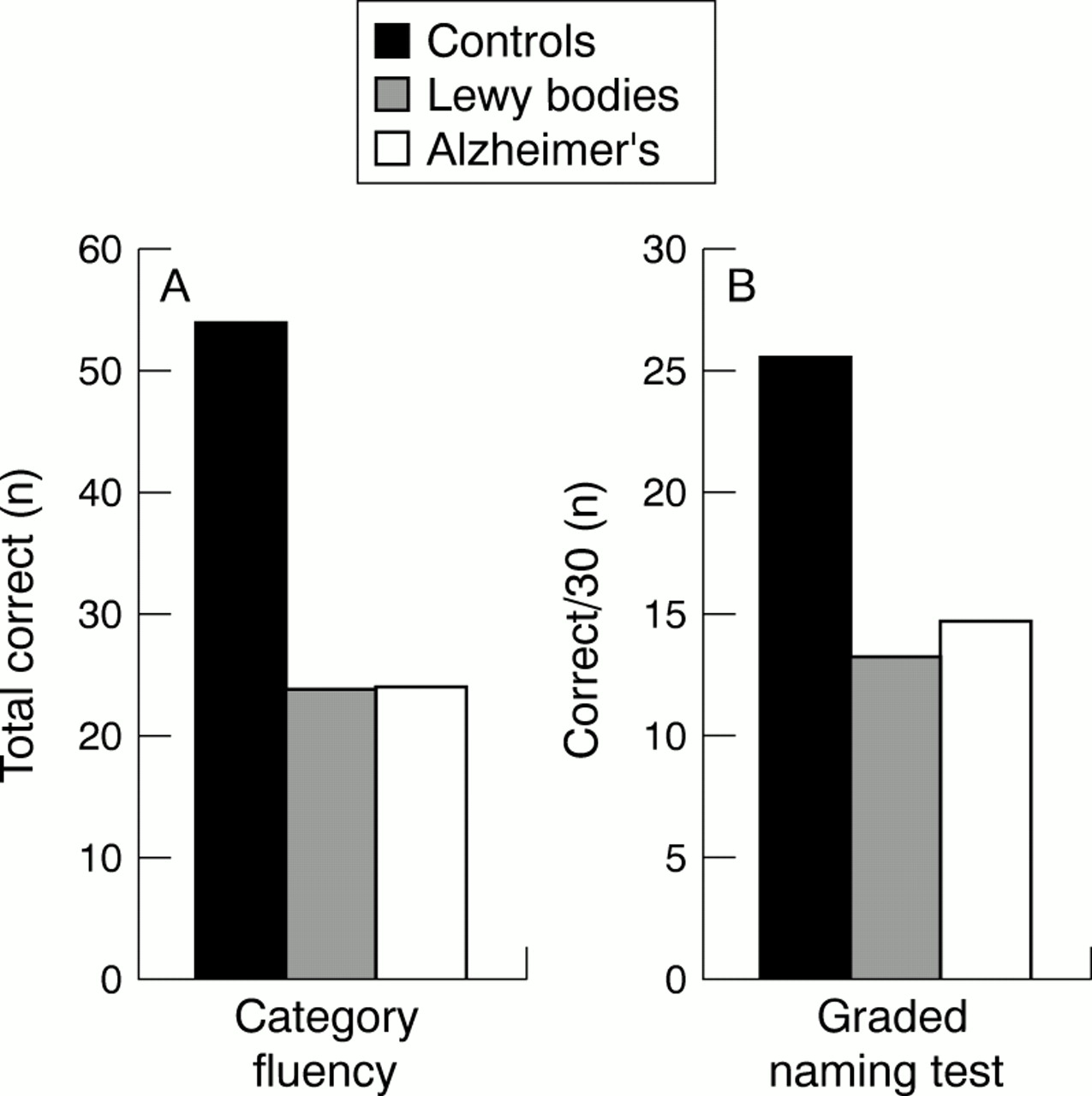
(A) Overall total number of correct items listed for each of the categories animals, fruits, and household items and (B) total number of correct items on the graded naming test.21
In summary, the AD and DLB groups both showed major deficits in episodic and semantic memory with more significant impairment in the AD group on one measure of verbal episodic memory (immediate and % recall of stories after a delay). Verbal short term memory, as measured by digits forward, was relatively spared in the AD group.
PERCEPTUAL AND SPATIAL TESTS
By contrast with the similar levels of performance of the patient groups on several of the memory tests, the patients with DLB showed significantly greater deficits on some of the tests of visuoperceptual and spatial ability. On the screening (figure-ground discrimination) test from the VOSP, the three groups performed equally well indicating that the patients with AD and those with DLB were able to understand the task and retained basic low level visuoperceptual abilities. On the fragmented letters, object decision, and cube analysis subtests, there were, however, highly significant group differences; post hoc analyses disclosed impairment in the DLB group relative to both controls and patients with AD, but no difference between controls and the AD group (NC=AD>DLB). On the silhouette identification test, the AD and DLB groups were equally impaired relative to controls. To illustrate these differences between the groups, their data have been normalised to allow for the differing maximum scores on the subtests as shown in fig3.

Percentage correct scores for various subtests from the visual object and space perception (VOSP) test.23
TESTS OF ATTENTION AND EXECUTIVE ABILITY
In common with their performance on tests of perceptual and spatial ability, the DLB group also showed substantially greater impairment than those with AD on some attentional tasks. On the elevator counting test of sustained attention, the AD group performed normally by contrast with a significant difference between the controls and DLB groups (NC=AD>DLB).
Analysis of two tests of selective attention—the elevator counting with distraction and map search test, both taken from the TEA —also disclosed major deficits with the following patterns on post hoc tests: elevator with distraction (NC>AD=DLB); map search (NC>AD>DLB). The performance of the three groups on the TEA tests is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage correct scores for three subtests from the test of everyday attention (TEA).24
Although six patients with DLB attempted the Stroop, only four were able to complete the critical colour-word interference component and all four were markedly slow and made numerous errors. The number completing the task was considered too small to allow a meaningful comparison with the three groups. The AD group (n=9) were clearly highly impaired relative to the controls.
On the Della Sala test of divided attention, all three groups performed equally well on the simple span task (task 1) as judged by the proportion of correct spans (NC=AD=DLB). On task 2, which involves timed box cancellation, both patient groups were slow, particularly the patients with DLB (task 2: NC>AD>DLB). An analysis of the number of boxes crossed in the dual task condition (task 3) showed differences between all groups, with greater impairment in DLB although the proportion of spans correctly repeated in 2 minutes was equivalent across the groups. As mentioned in the methods, any analysis of the effect of divided attention needs to consider the scores from both single tasks performed alone and simultaneously. Therefore a measure for the dual task decrement for box crossing was calculated as follows:

This gives a measure of the change in time taken by a subject to fill one box on the dual task compared with the single task, adjusting for the proportion of correct digit span sequences. The decrement score was identical in the AD and control groups, but substantially greater in DLB. An ANOVA of the decrement score confirmed a significant difference between groups and it was clear that only patients with DLB were impaired (NC=AD>DLB).
Only one patient with DLB was able to attempt the WCST, the others became hopelessly muddled. Comparison of the AD cases (n=9) and normal controls showed a significant difference (p<0.01).
On the FAS test of verbal fluency, both patient groups performed poorly, producing a highly significant group difference, but post hoc tests indicated that only the DLB group were significantly impaired.
In summary, both patient groups showed substantial deficits in the domains of attention and executive ability with the exception of sparing of sustained attention and normal performance on the critical dual task component of Della Sala's test in the AD group. The DLB group showed substantially greater impairment than the patients with AD on the Stroop and WCST (which most patients were unable to attempt) as well as some of the less demanding tests, notably the map search test from TEA, and Della Sala's test of dual attention.
Discussion
Although prior studies5 11 13 have pointed to disproportionate involvement of visuoperceptual and attentional processes in DLB, interpretation has been limited by the lack of specificity of the tests employed. The results of the present study, the first to employ a comprehensive battery of theoretically motivated tests, confirm that patients with DLB have substantially greater impairment of attentional and visuoperceptual abilities than patients with AD matched for age, education, and overall dementia severity.
The fact that the patients with DLB showed significantly greater impairment than the AD group on a range of tasks raises the possibility that they were simply more demented. The MMSE is a crude method of assessing dementia severity and equivalence on this task should not necessarily be taken as evidence of equivalent cognitive impairment. An alternative method of matching subjects for future studies of this type would be to use a broader assessment instrument which takes into account cognitive and functional abilities in everyday life.16
The various tests of working, episodic, and semantic memory disclosed a mixed set of findings. Although the patients with DLB showed more impaired digit spans, semantic memory and recognition were equally poor in patients with DLB and those with AD. The AD group, however, were substantially poorer in immediate and delayed recall of prose; the patients with DLB showed 28% retention compared with only 4% for the AD group. It is interesting to speculate why the difference in episodic memory between the two patient groups was disclosed by the logical memory test, which requires the structured recall of two stories. The fact that patients with AD have particular difficulty on free recall tasks and show a rapid loss of information has been extensively documented.29-32 The issue of whether AD produces a disproportionate effect on recall, as opposed to recognition, is complex as the tasks have different psychometric properties: recognition memory tests tend to have major ceiling effects in normal subjects.33 Recall of prose material also depends on semantic processing and has different retrieval demands. Studies employing the doors and people test, which was specifically designed to equate recall and recognition of verbal and visual material, and the California verbal learning test,30 have suggested equivalent impairment of recall and recognition in AD.32
On three subtests of the VOSP,23 the fragmented letters, object decision and cube analysis tasks, patients with DLB showed impairment relative to both controls and the AD group, whereas on the silhouette identification test, DLB and AD groups were equally impaired. The last task requires subjects to name or identify the silhouette profile of objects and animals viewed from unusual perspectives and draws on both perceptual and semantic abilities. The simple recognition of a silhouette as a real (versus unreal) object, or animal, is thought to require an intact structural description that has been linked to the right temporal lobe.23 Naming and other forms of accurate item specific identification require additional semantic processes that are associated with the left temporal lobe.34 The other tests from the VOSP that were failed by patients with DLB do not require semantic processes for their completion and can be considered, therefore, “purer” tests of perceptual or spatial ability. The finding of impaired identification of fragmented letters was particularly striking.
Although originally conceived in terms of right versus left hemispheric function,23 the cognitive abilities underlying performance on the spatial and perceptual subtests of the VOSP can be recast more in terms of ventral (what) versus dorsal (where) visual processing streams.35 36 According to this widely accepted dichotomy, the ventral pathway, or stream of information, proceeds from primary visual to visual association areas in the inferior-temporal region and underlies object recognition by the association of visual information with semantic knowledge about the perceived objects. Components of the VOSP which depend primarily on ventral processing are, therefore, the object decision, silhouette identification, and fragmented letters subtests. The dorsal stream is responsible for computing the location of objects in space, the guidance of hand movements during grasping, and complex visuospatial analysis: the cube analysis subtest of the VOSP draws heavily on the dorsal pathway. Based on the current findings, it seems that patients with DLB have severe deficits in both dorsal and ventral processing streams. Impairments of this type are seen in AD but typically occur at a later stage of the disease.37 38
Semantic knowledge has not previously been investigated in DLB, but seems from our study to be involved to an equivalent degree in AD and DLB. Both of the tests employed in the current study—the graded naming and category fluency tests—required a spoken response and can clearly be failed for other reasons, most notably a breakdown in the postsemantic aspects of name retrieval. It should be noted, however, that neither patient group produced phonological errors, implying breakdown at either a semantic level or in the processes of mapping semantics to phonology. It is obviously important that future studies include a wider range of verbal and non-verbal semantic tasks. The neural basis of the semantic deficit in AD remains somewhat controversial,17 39 but based on the findings in patients with semantic dementia, who have profound and focal atrophy in the inferolateral temporal lobe, we have speculated that the semantic impairment in AD reflects involvement of this region.17 40 To date, neuropathological studies in DLB have not quantified the degree of regional neuropathology in the way that the presumed spread of neurofibrillary tangles and plaques has been charted in Alzheimer's disease.41 42 On the combined evidence from visual and semantic tasks, we hypothesise, however, that visual association areas, including those involved with the ventral and dorsal processing streams, should show greater pathological involvement in DLB than in AD, but that the anterior and inferolateral temporal areas involved with semantic processing are perhaps equivalently involved in the two disorders.
Turning to the results of the attentional and executive tasks, patients with DLB showed pervasive deficits over and above those demonstrated in AD. The attentional deficits involved in sustained, selective, and divided attention are shown by their performance on the TEA elevator counting and map search tests and Della Sala's dual tasks, respectively. The vast majority of patients with DLB were unable to complete the more demanding Stroop and WCST tests. It seems, therefore, that attentional processes are even more impaired in DLB than in AD. The status of attention processing has been extensively investigated in AD, but variability in the tasks used and the level of overall dementia of the subjects in various studies makes it difficult to draw firm conclusions about the stage at which different components of attention become involved: a recent comprehensive review of the literature,43 concluded that attentional deficits in AD probably follow in the vanguard of episodic memory impairment, that selective attention is the most vulnerable component of attention, that sustained attention is the most resistant with divided attention occupying an intermediate position. This pattern was substantiated in the present study in that the AD group showed deficits on the tests of selective attention/response inhibition (Stroop, TEA elevator counting with distraction and map search), but performed normally on the critical dual task component of the Della Sala test. In DLB, by contrast, there seems to be a global breakdown in all aspects of attention, at least by the stage at which our patients presented. These findings are in keeping with the hypothesis that severe cholinergic deletion may underlie the attention deficit in DLB.
Our findings are potentially relevant to understanding the cognitive basis of hallucinations. The genesis of the hallucinations remains uncertain but the cholinergic depletion found in DLB has been strongly implicated. Cholinergic deficits are profound in DLB and exceed those found in AD.6 Such deficits correlate with the degree of cognitive impairment and are greater in hallucinating than in non-hallucinating patients with DLB.2 The basal forebrain cholinergic system (BFCS), which is involved in DLB, provides the major cholinergic innervation to the cortex and extends to brain regions such as the thalamus, prefrontal cortex, and parietal lobes.44The BFCS is thought to have a pivotal role in the modulation of attentional processes. It has been suggested that a breakdown in attention function underlies the visual hallucinations that are so characteristic of DLB. Another possibility, however, is that severe deficits in perceptual ability are critical for the genesis of hallucinations, or that a combination of attentional and perceptual deficits are a prerequisite. For recent comprehensive reviews of the aetiology and pathogenesis of hallucinations see Manford and Andermann45 and ffytche and Howard.46
As the patients with DLB in our study showed deficits in both perception and attentional function, it was not possible to conclude which of these is more critical for the genesis of the visual hallucinations. Some provisional speculations are perhaps warranted, however, based upon collateral evidence. Patients with the visual variant of AD, also referred to as posterior cortical atrophy or the biparietal variant of AD, present with profound visual disorientation and show marked deficits on tests of visuospatial or perceptual ability, yet do not hallucinate.47-50 Similarly, patients with peripheral ocular causes of visual failure develop a range of illusory and hallucinatory phenomena, but do not have the complex formed hallucinations which typify DLB.46 It seems, therefore, that perceptual deficits alone are unlikely to be sufficient to generate the characteristic visual hallucinations found in DLB. Likewise, attentional impairment is ubiquitous in the middle stages of AD yet relatively few patients develop visual hallucinations. We propose that the combination of degraded visual information about the environment, plus impaired and perhaps fluctuating attentional ability is critical to the genesis of the visual hallucinations found in DLB. This hypothesis could be tested in various ways. We had hoped to include both hallucinating and non-hallucinating patients with DLB, as well as patients with AD with and without hallucinations. A four way comparison of this type would unravel the contribution of diagnostic group, which potentially confounds the present study. Such a study presents, however, considerable practical difficulties. It might be possible to accrue a group of non-hallucinating patients with DLB, but a recent comprehensive study found that over 90% of patients with DLB hallucinated during the course of their illness8 making it difficult to find non-hallucinating cases. Conversely, we have found that patients with AD develop hallucinations at a relatively late stage of their disease when it is impossible to complete a full battery of tests. The most useful strategy for future studies might be to follow an AD cohort longitudinally in an attempt to relate the onset of hallucinations with changes in cognitive performance. A further useful development would be to correlate the frequency and severity of hallucinations with the extent of cognitive deficit in a larger group of patients with DLB.
In conclusion, we have demonstrated that patients with DLB showed greater impairment in visuoperceptual and attentional processes than a matched group of patients with AD. The attentional deficit was pervasive and involved all aspects of attention. Semantic memory and recognition based episodic memory were equally impaired in the two groups, but the patients with AD performed worse on tests of prose recall.
Acknowledgments
This work was supported by a project grant from the Wellcome Trust. RJP was funded by Novartis.
References
Linked Articles
- Editorial commentary