Article Text

Abstract
OBJECTIVES Cardiovascular reflex tests have shown both sympathetic and parasympathetic failure in Parkinson's disease. These tests, however, describe the autonomic responses during a restricted time period and have great individual variability, providing a limited view of the autonomic cardiac control mechanisms. Thus, they do not reflect tonic autonomic regulation. The aim was to examine tonic autonomic cardiovascular regulation in untreated patients with Parkinson's disease.
METHODS 24 Hour ambulatory ECG was recorded in 54 untreated patients with Parkinson's disease and 47 age matched healthy subjects. In addition to the traditional spectral (very low frequency, VLF; low frequency, LF; high frequency, HF) and non-spectral components of heart rate variability, instantaneous beat to beat variability (SD1) and long term continuous variability (SD2) derived from Poincaré plots, and the slope of the power law relation were analysed.
RESULTS All spectral components (p<0.01) and the slope of the power-law relation (p<0.01) were lower in the patients with Parkinson's disease than in the control subjects. The Unified Parkinson's disease rating scale total and motor scores had a negative correlation with VLF and LF power spectrum values and the power law relation slopes. Patients with mild hypokinesia had higher HF values than patients with more severe hypokinesia. Tremor and rigidity were not associated with the HR variability parameters.
CONCLUSIONS Parkinson's disease causes dysfunction of the diurnal autonomic cardiovascular regulation as demonstrated by the spectral measures of heart rate variability and the slope of the power law relation. This dysfunction seems to be more profound in patients with more severe Parkinson's disease.
- Parkinson's disease
- heart rate
- autonomic nervous system
Statistics from Altmetric.com
Impaired autonomic cardiovascular regulation has been associated with an increased risk of mortality both in patients with heart disease and in randomly selected general populations. Autonomic dysfunction involving both the sympathetic and parasympathetic systems has also been demonstrated in Parkinson's disease using cardiovascular reflex tests based on heart rate and blood pressure responses to various stimuli.1-6 However, the clinical significance and pathophysiology of these findings in Parkinson's disease are poorly understood.
As cardiovascular reflex tests show great individual variability7 and only provide information obtained from responses to stimuli during short periods under experimental conditions, alternative methods for evaluation of the autonomic nervous system are needed. Conventional time and frequency domain analysis techniques based on the linear fluctuations of heart rate obtained from 24 hour ECG recordings provide useful tools for assessing quantitatively the tonic autonomic effects on the heart.8The conventional time and frequency domain measures of heart rate variability analysed from ambulatory ECG recordings, previously used as predictors of cardiac arrhythmia and mortality in coronary heart disease,9-11 are diminished in CNS disorders such as stroke, epilepsy, brain injuries, and in some degenerative neurological diseases.12-14 A recent study has also reported diminished variability of standard RR intervals and spectral measures of heart rate variability in Parkinson's disease.15
As the heart is not a periodic oscillator under normal physiological conditions the measures of heart rate variability are insufficient in outlining the changes in heart rate dynamics.16 17Therefore, new methods based on non-linear dynamics and fractal analysis have been introduced to quantify complex heart rate dynamics and to complement conventional measures of its variability.18-20 Dynamic measures of heart rate variability have provided important information on cardiovascular mortality as some of them have been shown to be more powerful predictors of death than the traditional risk markers both in elderly people21 and in patients with impaired left ventricular dysfunction.22 23 However, heart rate dynamics have been reported as being unpredictable in patients with previous myocardial infarctions.24
The aim of this study was to evaluate diurnal autonomic cardiovascular function during daily activities in untreated patients with Parkinson's disease by analysis of the traditional spectral and non-spectral components of heart rate fluctuation in conjunction with two dimensional vector analysis and power law relation analysis of heart rate dynamics. We also analysed the correlation of heart rate variability to the disease severity and clinical autonomic nervous system (ANS) symptoms.
Patients and methods
PATIENTS
Sixty consecutive patients with idiopathic Parkinson's disease fulfilling the Parkinson's Disease Society Brain Bank25clinical criteria were included in the study from patients that were referred to the Department of Neurology in Oulu University Hospital because of extrapyramidal symptoms. The patients were independent in their daily activities and had no previous antiparkinsonian medication. Patients with manifestations of other central or peripheral nervous system disorders and patients with any other disease or medication known to affect the ANS were excluded. The clinical disability of the Parkinson's disease was graded using the Hoehn and Yahr26staging and the Unified Parkinson's disease rating scale (UPDRS).27 The clinical severity of autonomic failure was graded using a rating scale to assess 11 different modalities of ANS measures (postural dizziness and disturbances of sweating, urinary function, bowel function, sexual function, heart rate regulation, salivation, and breathing and signs of peripheral circulation disturbances, sluggish pupillary reactions, and seborrhoea), the dysfunction being graded from 0 to 2 (0=absent, 1=mild, 2=moderate to severe).3 Orthostatic hypotension was evaluated in a test where the patients rose after a 30 minute rest taken in a supine position and stood still in an upright position for 10 minutes. The blood pressure was recorded just before and immediately after standing up, as well as at 1 minute intervals during the standing.
One patient was excluded because of recurrent supraventricular arrhythmias during the recording of ECG responses, which made the data ineligible for analysis. Three further patients were excluded due to technical disturbances in the ECG recordings. The clinical follow up of the patients was continued after the study trial period, the mean follow up time being 3 years (range 1.3–4.6 years). This post-trial follow up disclosed one case of progressive supranuclear palsy and one case of multiple system atrophy, which were also excluded from the study.
The control group consisted of 47 healthy age matched subjects selected from among healthy people who were participating in a trial comparing the characteristics of hypertensive and normotensive subjects randomly selected by their social security code from the population of the city of Oulu. They all underwent a complete physical examination and had no disease or medication affecting the ANS in their history. The demographic data of the patients and controls are given in table 1. All patients and controls gave their informed consent before their inclusion in the study. The study was approved by the ethics committee of the Medical Faculty, University of Oulu, and was carried out according to the principles of the Declaration of Helsinki.
Demographics of the patients with PD at baseline and of the control subjects
METHODS
A two channel 24 hour ambulatory ECG recording (Delmar Avionics® electroscanner) was performed in all the patients and control subjects. During the recording in a hospital ward the subjects were encouraged to continue their daily activities.
The ECG data were sampled digitally and transferred from the Oxford Medilog scanner to a microcomputer for analysis of heart rate variability. All RR interval time series were first edited automatically, after which careful manual editing was performed by visual inspection of the RR intervals. Each RR interval time series was passed through a filter that eliminates premature beats and artefacts and deletes the filling gaps using previously described methods.28 In the final analysis of the linear and non-linear components of heart rate variability 24 hour measurements were divided into segments of 8000 RR intervals, and only segments with >85% sinus beats were included. The mean duration of all RR intervals and the SD of all RR intervals (SDNN) were computed as time domain measures reflecting slow fluctuations of RR intervals. SDNN reflects primarily the very low frequency fluctuation in heart rate behaviour, possibly reflecting the peripheral vascular resistance and thermoregulation.29
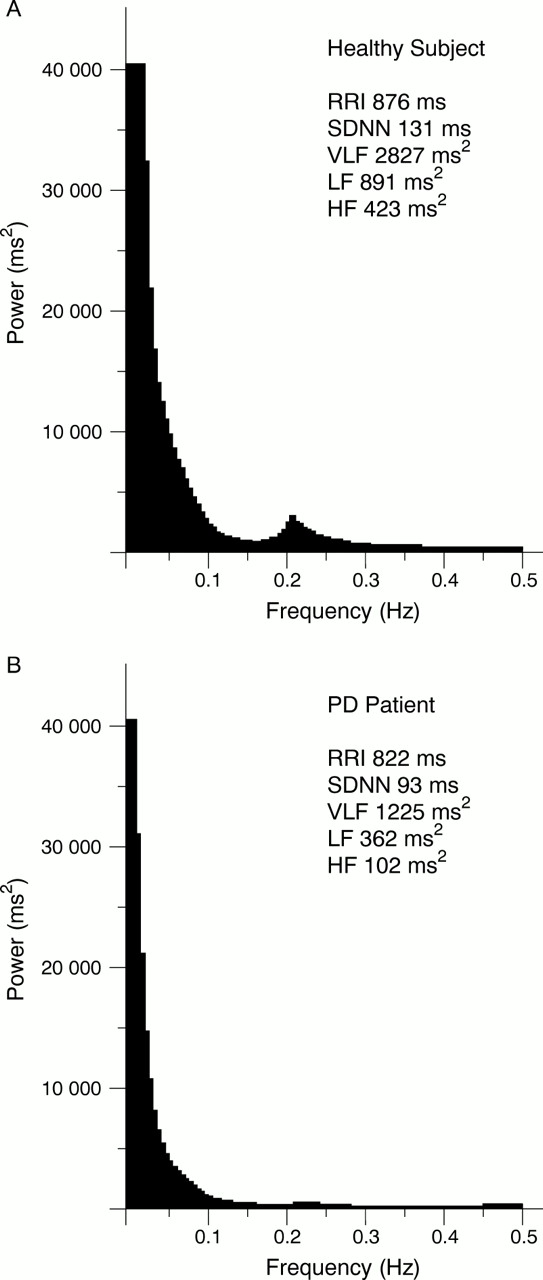
An autoregressive model was used to estimate the power spectrum densities of heart rate variability.30 The power spectra were quantified by measuring the area in three frequency bands: 0.005 to 0.04 Hz (very low frequency, VLF), 0.04 to 0.15 Hz (low frequency, LF) and 0.15 to 0.4 Hz (high frequency, HF). The HF fluctuation of RR intervals mainly reflect the cardiovagal modulation and the inspiratory inhibition of vagal tone, whereas the LF and VLF bands are affected by sympathetic excitation,31 sympathovagal balance,32 and arterial pressure oscillations.33
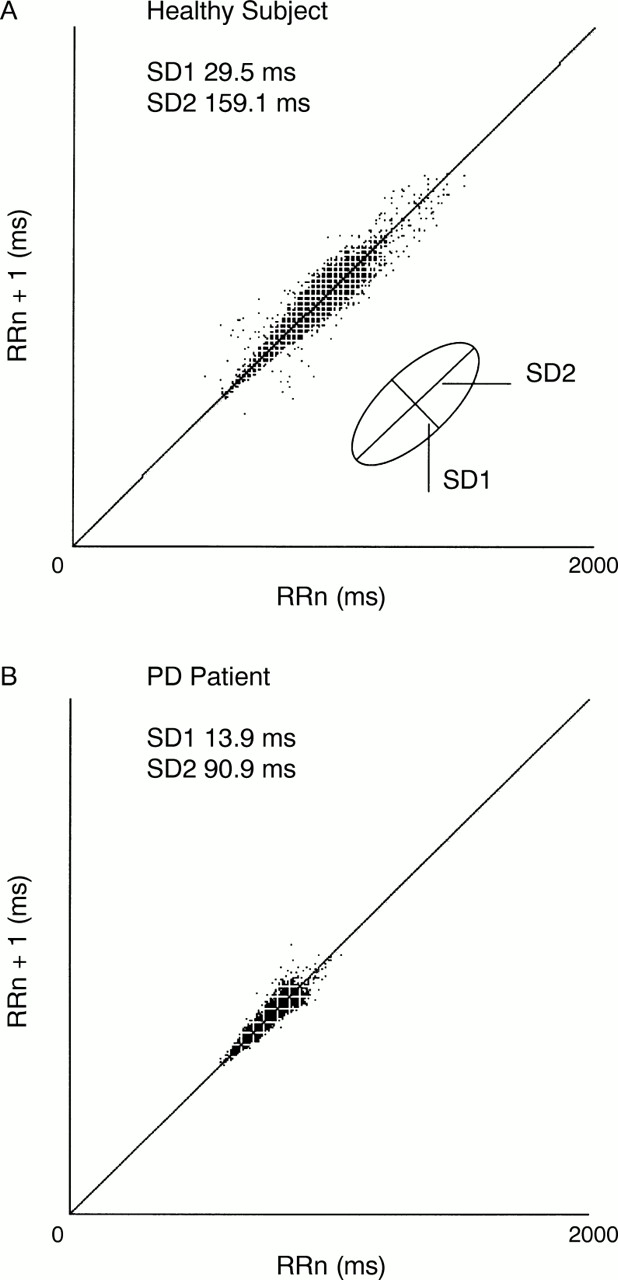
For quantitative two dimensional vector analysis, the SD of continuous long term RR interval variability (SD2) and the instantaneous beat to beat RR interval variability (SD1) were analysed and visually presented as Poincaré plot scattergrams in which each RR interval is plotted as a function of the previous one.28 34 The markings of the plot are gathered around a line of unitary slope passing through the origin and it graphically represents both quantitatively and qualitatively the type of RR variation included in the recording. In quantitative analysis of the Poincaré plots, SD1 describes the magnitude of beat to beat RR interval variability reflecting vagal modulation of the heart rate and has a relatively strong correlation with the HF spectral component; SD2 describes the long term RR interval fluctuations and reflects the magnitude of both VLF and LF spectral components. A potential advantage of the Poincaré method over spectral analysis techniques is that it is not sensitive to stationary irregularities and trends in the RR intervals being therefore more suitable for HR variability analysis from uncontrolled ambulatory ECG recordings.34
The power law relation of RR interval variability, a spectral measure reflecting the distribution of the spectral characteristics of R-R interval oscillations, was calculated from the frequency range of 10-4 to 10-2, characterising mainly slow heart fluctuations, using a previously described method.11 The point power spectrum was logarithmically smoothed in the frequency domain, and the power was integrated into bins spaced 0.0167 log(Hz) apart. A robust line fitting algorithm of log (power) on log (frequency) was then applied to the power spectrum between 10-4 to 10-2, and the slope of this line was calculated. This frequency band was chosen on the basis of previous findings regarding the linear relation between log (power) and log (frequency) in the frequency band.11 35 The physiological background of the spectral distribution is not exactly known, but it is influenced by the autonomic input to the heart as the slope of the power law relation is especially steep in denervated, transplanted hearts.36 Figures 1, 2, and 3present examples of the power spectrum analysis of HR variability, Poincaré plots and power law relation slopes from a healthy subject and a patient with Parkinson's disease whose values represent the median of the spectral parameters for the group.

(A) Spectral analysis of heart rate variability in a healthy subject and (B) a patient with Parkinson's disease. The area from 0.005 to 0.04 Hz represents VLF power, the area from 0.04 to 0.15 Hz LF power, and the area from 0.15 to 0.4 Hz HF power.

(A) Poincaré plots from a healthy subject and (B) a patient with Parkinson's disease. SD1 Indicates SD of instantaneous RR interval variability measured from axis 1, and SD2 of long term continuous RR interval variability measured from axis 2.

{kind=link}
{kind=link}
{kind=link}
(A) Slopes of power law relation of a healthy subject and (B) a patient with Parkinson's disease.
DATA ANALYSIS
Statistical analysis was performed using the Mann-Whitney two sample test to compare the values of the control subjects and those of the patients. The correlation between the clinical parameters of Parkinson's disease and the various measures of heart rate variability was analysed with Spearman's correlation coefficient. The patients, dichotomised according to the severity of the major signs of Parkinson's disease, were analysed with the Mann-Whitney two sample test. The data were not adjusted for multiple comparisons. The significance for all analyses was set at p<0.02.
Results
In the patients the SDNN values (p=0.024), and the VLF (p=0.001), LF (p=0.009), and HF (p=0.004) spectral components were lower than those of the control subjects. The RR interval did not differ (p=0.905) between the patients and the control subjects. The SD1 and SD2 of the Poincaré measures in the patients did not differ significantly from the values in the control subjects (p=0.053 and p=0.186). The slope of the power law relation of the heart rate variability was deeper (p=0.002) in the patient group than in the control subjects. The mean values of the various measures of heart rate variability in the patients and the control subjects are presented in table 2.
Measures of heart rate and heart rate variability in patients with Parkinson's disease (PD) and control subjects
The total UPDRS score and its motor subscale had a negative correlation with the VLF and LF spectral parameters. Of the cardinal motor signs of Parkinson's disease the severity of hypokinesia showed a correlation with the slope of the power law relation. The correlation coefficients of the clinical parameters and the heart rate variability measures are presented in table 3. When the effect of the severity of the major signs of Parkinson's disease was analysed in a dichotomised manner, the patients with minimal hypokinesia (UPDRS hypokinesia score 1) had higher HF (389 v 143 ms2, p=0.008) spectral powers than the patients with more severe hypokinesia. Age correlated with the time domain (SDNN, p=0.002) and the spectral parameters VLF (p<0.001), LF (p<0.001), and HF (p=0.003), and also with the slope of the power law relation (p<0.001). The severity of tremor and rigidity, the presence of orthostatic hypotension, and the duration of the disease did not correlate with the HR variability indices. No individual clinical sign or symptom of autonomic dysfunction was associated with the heart rate variability measures, whereas the total score of the signs of autonomic dysfunction had a negative correlation with the LF (r=0.39, p=0.003) spectral component.
Correlation coefficients (Spearman's) between different clinical measures and heart rate parameters in patients with Parkinson's disease
Discussion
The present study is the first to show suppressed 24 hour heart rate variability in untreated patients with Parkinson's disease. Not only were the traditional time and frequency domain measures of heart rate variability diminished, but the slope of the power law relation of heart rate variability was also affected by the cardiovascular autonomic dysfunction associated with Parkinson's disease. The UPDRS total and motor scores and the hypokinesia score had a negative correlation with the spectral measures of heart rate variability and the slope of the power law relation.
Previous studies on patients with Parkinson's disease using cardiovascular reflex tests have shown suppressed heart rate responses to different stimuli such as normal breathing,5 deep breathing,4 37 the Valsalva manoeuvre,3 5and tilting.1 3 5 Blood pressure responses to tilting have also been more pronounced in patients with Parkinson's disease than in healthy subjects.1 2 5 Decreased heart rate variability analysed from 100 RR intervals has been shown in patients with Parkinson's disease, with Shy-Drager syndrome, and with spinocerebellar ataxia, including patients with olivopontocerebellar atrophy.38 In a cross sectional study with a few patients, using traditional time domain and spectral heart rate variability measures analysed from 24 hour ambulatory ECG, patients with Parkinson's disease had lower SDNN values, LF (0.04–0.15 Hz) values, and HF (0.15–0.4 Hz) values in the night period than healthy controls.15 In the present study, even untreated patients with Parkinson's disease showed diminished SDNN values and all the power spectrum measurements were lower in the patients than in the controls, suggesting ANS involvement in the pathophysiological process of Parkinson's disease early in the course of the disease.
In the present study the UPDRS total and motor scores and the severity of hypokinesia were associated with the heart rate variability measures. However, because the association was not strong, the mechanisms causing the motor disability in Parkinson's disease may differ from those leading to impairment of the cardiovascular autonomic regulation. Moreover, the increasing severity of clinical autonomic dysfunction signs such as seborrhoea, pupillary dysfunction, and peripheral circulation disturbances was related to a decrease in the LF power, suggesting shared pathophysiological mechanisms. The disease duration did not correlate with the heart rate variability, which may be explained with the long disease duration in patients with Parkinson's disease with tremor as the dominant sign, the overall disability of their disease being mild. In accordance with earlier studies39 40 we found a decrease of all the spectral power components of heart rate variability with advancing age.
Even though the roles of the sympathetic and parasympathetic nervous systems in the regulation of heart rate fluctuation are unclear, both systems are linked with the cardiovascular dysfunction of patients with Parkinson's disease. Of the power spectrum frequency bands the HF band is thought to reflect the parasympathetic activity mediated by the vagus nerve, whereas the LF band is thought to be dependent on negative feedback of the baroreflex arch mediated by both sympathetic and parasympathetic activity in an upright position and mainly by vagal activity in a supine position.41 42 Our results suggest that autonomic cardiovascular dysfunction in Parkinson's disease is multidimensional as all the spectral components were lower in our patients than in the controls and the steepness of the power law relation slopes was increased. As this slope is especially steep in denervated hearts—for example, in heart transplants— the results in our patients may be due to peripheral sympathetic pathology, which has also been shown in patients with early Parkinson's disease using new investigatory techniques such as [123]I-metaiodobenzylguanidine myocardial scintigraphy and 6-[18F]fluorodopamine PET.43-45
The pathological processes in Parkinson's disease involve both the sympathetic and parasympathetic nervous systems because Lewy bodies and neuronal degeneration have been found throughout the central autonomic network—that is, in the hypothalamus, locus ceruleus, dorsal vagal nucleus, and nucleus ambiguus, as well as in the intermediolateral column cells in the spinal cord, and in postganglionic sympathetic neurons in the prevertebral and paravertebral ganglia in addition to the dopaminergic striatonigral pathway.46 Thus, theoretically, cardiovascular dysregulation could relate to a central or peripheral pathophysiology, which is also supported by our results indicating both sympathetic and parasympathetic dysfunction.
Our results show that heart rate variability analysis of ambulatory ECG, using both conventional spectral and non-spectral dynamic methods of heart rate variability, provides a feasible method for assessing the ANS functions. The advantages of 24 hour ambulatory ECG recordings are good reproducibility and the information concerning the low frequency bands of spectral heart rate variability gathered over longer time periods than standard cardiovascular reflex tests can provide.9 41 47 Our results agree with previous studies using standard cardiovascular reflex tests and methods assessing cardiac sympathetic denervation, demonstrating both parasympathetic and sympathetic dysfunction early in the course of Parkinson's disease. Because of great interindividual variation in the heart rate variability measures used in this study, these parameters can only be used to assess autonomic dysfunction at a group level as is also the case with standard cardiovascular reflex tests.44 However, this method may provide new information on the pathophysiological mechanisms leading to autonomic cardiac dysregulation. Our finding that the slope of the power law relation of 24 hour heart rate variability is steeper in patients than in healthy subjects give rise to the question as to whether these measures could be used as predictors of mortality in patients with Parkinson's disease, because the power law relation has been proved to be a more powerful predictor of death than traditional risk markers in elderly subjects35 and in patients with recent myocardial infarction.36 It has been proved to be even better than the spectral parameters that are independent predictors of outcome in patients with coronary heart disease and after acute myocardial infarction.
Conclusion
The analysis of HR variability from a 24 hour ambulatory ECG recording disclosed an extensive dysfunction of the tonic cardiovascular autonomic regulatory system in untreated Parkinson's disease. The conventional and dynamic spectral measures show a negative correlation with the UPDRS total and motor scores and hypokinesia scores. Of the dynamic measures the slope of the power law relation especially seems to be sensitive to abnormalities in the HR fluctuation of Parkinson' disease.
Acknowledgments
This study was supported by a grant from the Maire Taponen Foundation and the Finnish Neurology Foundation.