Article Text

Abstract
OBJECTIVE Scintigraphy with [123I]metaiodobenzyl guanidine ([123I]MIBG) enables the quantification of postganglionic sympathetic cardiac innervation. Recently, myocardial [123I]MIBG scintigraphy has been found to be useful in distinguishing Parkinson's disease, a Lewy body disease, from other akinetic rigid syndromes. Some patients initially diagnosed with dementia of the Alzheimer's type (DAT) are discovered to have an alternative disease such as dementia with Lewy bodies (DLB), despite the application of stringent diagnostic criteria. In the present study, examinations were performed to clarify the usefulness of myocardial [123I]MIBG scintigraphy in improving the differential diagnosis between patients with DLB and DAT.
METHODS Fourteen patients with DLB and 14 patients with DAT underwent scintigraphy with [123I]MIBG, combined with orthostatic tests and cardiac examinations.
RESULTS In all patients with DLB, the heart to mediastinum (H/M) ratio of MIBG uptake was pathologically impaired in both early and delayed images, independently of the duration of disease and autonomic failure. All patients with DAT had successful MIBG uptake in the heart regardless of duration of disease and autonomic failure. Orthostatic hypotension was seen in four patients with DAT and 13 patients with DLB.
CONCLUSIONS [123I]MIBG myocardial scintigraphy might detect early disturbances of the sympathetic nervous system in DLB and might provide useful diagnostic information to discriminate DLB from DAT. The distinction between DLB and DAT may be improved by greater emphasis on cardiac sympathetic disturbances.
- metaiodobenzyl guanidine
- dementia with Lewy bodies
- dementia of the Alzheimer's-type
- autonomic function
Statistics from Altmetric.com
Dementia of the Alzheimer type (DAT) is characterised clinically by a progressive decline in memory and higher cortical functions.1 Neuropsychiatric features including depression, delusion, agitation, or hallucinations may emerge in advanced disease stages. About 60% of patients with DAT also exhibit mild or moderate parkinsonian signs during their illness.2
In recent years, dementia with Lewy bodies (DLB) has been acknowledged as the second most common senile degenerative dementia after DAT.3 Patients are clinically characterised by a fluctuating intellectual decline combined with neuropsychiatric features such as depression, visual hallucinations, delusions, and hypersensitivity to classic neuroleptic drugs. Parkinsonian signs or symptoms are present in most patients and may be associated with postural instability and falls.4 A recent retrospective study suggested that DLB and DAT are clinically different because of the fluctuating dementia, visual hallucinations, and marked parkinsonian features in DLB.4 However, because of overlapping symptoms, the clinical distinction of patients with DLB and DAT may be difficult. Litvan et al have reported that most cases of misdiagnosis in Lewy body disease including Parkinson's disease (PD) and DLB present themselves with progressive supra- nuclear palsy (PSP), multiple system atrophy (MSA), and DAT.5 Although the usefulness of myocardial [123I]metaiodobenzyl guanidine ([123I]MIBG) scintigraphy in the differentiation of PD from PSP and MSA has recently been established,6 7 this method has not yet been shown to be useful in differentiating DLB from DAT.
Metaiodobenzyl guanidine is a physiological analogue of noradrenaline (norepinephrine) and is actively transported into noradrenaline granules of sympathetic nerve terminals by the noradrenaline transporter.8 [123I]MIBG myocardial scintigraphy can be performed very safely9 and is used clinically to estimate local myocardial sympathetic nerve damage in various heart diseases,10-13 autonomic nerve disturbance in diabetic neuropathy,14 disturbance of the autonomic nervous system in neurodegenerative disease,6 7 15-18pure autonomic failure,19 and familial amyloidotic polyneuropathy.20
It is of particular interest to distinguish between DAT and DLB during life, because accurate clinical diagnosis of the dementias is critical for proper management and assessment of prognosis.21-23
Therefore, the aim of this [123I]MIBG myocardial scintigraphic study was to describe the sympathetic dysfunction of DLB and to explore the contribution of the myocardial accumulation of MIBG to the differential diagnosis between DAT and DLB.
Methods
PATIENTS
A consecutive series of patients attending the Department of neurology were recruited for this study. In total 28 patients with progressive dementia, parkinsonian features, and psychiatric symptoms of unknown aetiology and relevance were studied. Fourteen were considered to have probable DAT, and others to have probable DLB. All patients underwent routine laboratory tests, the mini mental state examination (MMSE), and other psychometric tests. There were no findings of non-degenerative cognitive disorders such as cerebrovascular diseases and intracranial mass lesions in the MR images of the brain and cerebral blood flow by SPECT. None of the subjects had any history of cardiovascular or thyroid disease or hyperlipidaemia, and none had ever used any drugs known to affect [123I]MIBG accumulation.24 All were normotensive, and diabetes mellitus was excluded by testing the urine and blood sugar. No abnormalities indicating ischaemic heart disease, arhythmia, or hypertrophy were seen on ECG, wall motion studies, or [99mTc]tetrofosmin cardiac perfusion scan.
The group with probable DAT comprised 14 patients. The inclusion criteria for probable DAT were those of the National Institute of Neurological Disease and Stroke/Alzheimer's Disease and Related Disorders Association.1 The mean (SD) age was 70.9 (5.1) years for the 10 women and four men, and the mean (SD) MMSE score was 18.5 (5.9). The mean (SD) duration of illness was 36.5 (24.2) months. Clinical data from the time of the MIBG scintigraphy are listed in table 1.
Characteristics of patients with DAT
The group with probable DLB comprised 14 patients. The inclusion criteria for DLB were the clinical criteria of the Consortium on DLB International Workshop.4 The criteria for DLB include three core features (fluctuating cognitive functions, recurrent visual hallucinations, and spontaneous parkinsonism), and two or more core features are necessary for a diagnosis of probable DLB. Exclusion was based on the exclusion features of the Consortium on DLB International Workshop criteria.4 The mean (SD) age was 73.6 (6.6) years for the nine women and five men, and the mean (SD) score of the MMSE was 19 (5). The mean duration of illness was 41.9 (31.1) months. Clinical data obtained at the time of the MIBG scintigraphy are listed in table 2. There were no significant differences in the duration of illness, age, and MMSE score between the DAT and DLB groups. At the time of examination, five patients with DLB were on antiparkinsonian medication, which included levodopa (n=4), bromocriptine (n=2), and droxidopa (n=1). Levodopa improved parkinsonism of these four patients with DLB. All subjects had no family history of memory disorder. The Hachinski score25 was less than 5, and the DSM-IV criteria26 were fulfilled for all patients. Informed consent was obtained from all subjects or their caregivers before the study, and no adverse reactions were found in all the patients on whom [123]I-MIBG myocardial scintigraphy was performed.
Detail of patients with DLB
[123I]MIBG IMAGING
After patients had been in a supine position for 20 minutes, 111MBq [123I]MIBG (Daiichi Radioisotope Laboratories, Tokyo, Japan) was injected intravenously. The energy discrimination was centred on 159 keV with a 20% window. Early and delayed single photon emission computed tomography (SPECT) was performed 20 minutes and 3 hours after injection, respectively. Planar imaging for 2 minutes in the anterior and left anterior oblique projection was performed during SPECT automatically. Planar scans and SPECT and were performed with a triple head gamma camera equipped with a low energy, high resolution parallel hole collimator (GCA9300A/HG, Toshiba, Tokyo, Japan). The detector system was interfaced to a dedicated nuclear medicine computer (GMS5500A, Toshiba). The data acquisition matrix of planar imaging was 128×128.
RELATIVE MIBG UPTAKE RATIO
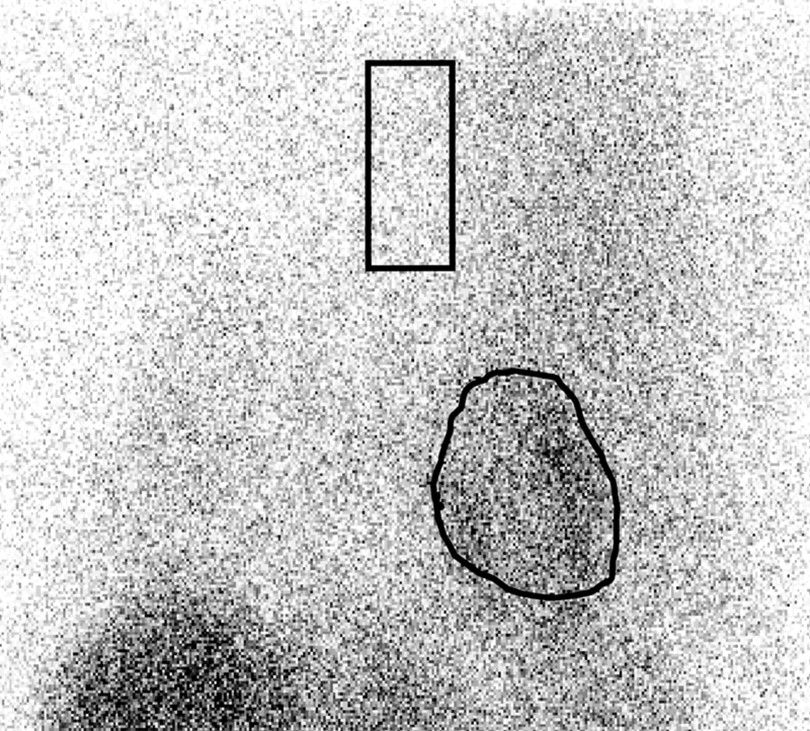
Relative organ uptake was determined by setting the region of interest (ROI) on the anterior view. The left ventricular ROI was drawn manually, including the left ventricular cavity, and a rectangular ROI was set on the upper mediastinum area (fig 1). Heart to mediastinum (H/M) ratio was calculated by dividing the count density of the left ventricular ROI by that of the mediastinal ROI. The same ROIs were then applied to the delayed image to obtain better reproducibility. Background subtraction was not performed from any ROI count. Using the H/M ratio, which is a quantitative standard measure in nuclear medicine,27 clearly reduces the influence of technical variables of different cameras and protocols and allows the comparison of results among different centres.7 8 The H/M ratio has often been used as a simple quantitative measure.27

Definition of regions of interest (ROIs) on the anterior planar image.
ORTHOSTATIC TEST
Blood pressure was initially recorded after a 20 minute rest in a supine position, and it was subsequently recorded for 10 minutes after standing. A diagnosis of orthostatic hypotension was made when the systolic blood pressure fell by 20 mm Hg or more or when the diastolic blood pressure fell by at least 10 mm Hg within 10 minutes of standing.28
STATISTICAL ANALYSIS
Results are expressed as mean values (SD) and analyzed by the Student's t test and one way analysis of variance (ANOVA). Correlations were evaluated by Spearman's rank correlation test. A p value<0.05 was considered to be statistically significant. All statistical analyses were performed using Stat View 5.0 software on a Macintosh computer.
Results
Reduced cardiac accumulation was seen in both early and delayed images in patients with DLB. In patients with DAT, successful cardiac uptake of MIBG was found both in the early and delayed images (fig 2).

Planar cardiac imaging of [123I]MIBG in a patient with DAT (A) early, (B) delayed, and with DLB (C) early, (D) delayed.
There were significant differences in the mean value of H/M ratios in both early and delayed images between patients with DLB and those with DAT (early H/M ratio :DLB 1.31 (0.17), DAT 2.26 (0.29), delayed H/M ratio: DLB 1.18 (0.10), DAT 2.22 (0.30); fig 3). There was no correlation between the H/M ratio and the duration of disease in either the patients with DAT or those with DLB. In both patient groups, there were no significant differences in the H/M ratio between those with and without OH.

Distribution of heart to mediastinum uptake (H/M) ratio of MIBG in patients with DAT and those with DLB. The box plots show the median values (thick line), the 25th (lower line of box) and 75th percentiles (upper line of box); T bars indicate the 10th and 90th percentiles; small filled boxes represent mean values of the H/M ratio.
Thirteen patients had orthostatic hypotension in the DLB group. In the DAT group, four patients had orthostatic hypotension, and it was seen in relatively elderly patients (mean age of DAT with orthostatic hypotension: 76.8 (3.9), mean age of DAT without orthostatic hypotension: 68.5 (3.4); p<0.05).
Discussion
Firstly, it is important to note that the cases of DLB and DAT cited in this study were clinically diagnosed. Pathologically confirmed cases would have been ideal. However, the clinical criteria employed have been validated against pathologically confirmed cases, and have been reported to have a positive predictive value, as well as high sensitivity and specificity.29-31
In the current study, cardiac uptake of MIBG was grossly impaired in all patients with DLB, and this impairment was independent of the severity and duration of illness. None of the patients with DAT showed a reduced myocardial MIBG accumulation. This feature of myocardial MIBG accumulation was valuable in differentiating patients with DLB from those with DAT.
We think that the myocardial [123I]-MIBG was a more reliable marker than orthostatic hypotension in distinguishing DLB from DAT.
When the most typical presentation of DLB—early neuropsychiatric features and dementia, and mild parkinsonian signs—occur in patients with DLB, it is easy to discriminate DLB from DAT. But patients with DLB presenting with only dementia in the early stage are difficult to differentiate from those with DAT.32 33 Lopezet al 34 reported that the difficulty in differentiating DLB from DAT was caused by the character of the Lewy bodies, which are part of the neuropathological range of DAT and can sometimes exist without clinical manifestations. The [123I]-MIBG method may have great potential to become a useful diagnostic tool, particularly in such patients with DLB who do not show typical signs and symptoms.
Non-invasive imaging with radioiodinated MIBG can assess efferent adrenergic neuronal functions in the heart. The MIBG competes with noreadrenaline for neuronal uptake and is taken up by a low affinity non-neuronal mechanism.35 Scanning during the first 15–20 minutes postinjection mainly reflects the greater influx of MIBG into extraneural spaces in the myocardial tissue, rather than into the neuronal components. The neuronal accumulation of MIBG reaches its peak 3–4 hours after injection.36 The second scan displays the neuronal uptake of MIBG more explicitly. Therefore, myocardial MIBG uptake was assessed 20 minutes and 3 hours postinjection in this study. Denervated myocardium treated with epicardial phenol and subjected to ganglionectomy showed a decrease in tissue noradrenaline and MIBG.37 38 These experimental findings suggest that MIBG uptake reflects actual adrenergic neuronal function in the myocardial tissue in vivo.
These findings underscore the postganglionic pattern of involvement of the autonomic nervous system in patients with DLB, as recently reported in several in vivo studies of Lewy body disease.6 The lack of MIBG positivity, even in the early images, suggests a loss or destruction of cardiac sympathetic nerve endings.38 In the sympathetic nervous system, Lewy bodies have been found in the hypothalamus, the intermediolateral cell columns of the spinal cord, the sympathetic ganglia, and the cardiac plexus39-41 in patients with Parkinson's disease. In patients with DLB, Lewy bodies may also be widely distributed throughout the central and peripheral nervous system33 42; it is also important to note that in patients with Parkinson's disease, postganglionic damage of the sympathetic nerves may cause a lack of cardiac MIBG uptake.6 7
According to previous studies.6 16 17 antiparkinsonian drugs in clinical use have no effect on the MIBG uptake.
Disturbance of the noradrenaline transporter has been reported in cardiac diseases and diabetic neuropathy14 Takatsuet al showed a reduction of cardiac [125I]MIBG accumulation in mice treated with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP). It is suspected that MPTP damaged not only the dopaminergic neurons, but also the postganglionic sympathetic nerves.43 In DLB, it might be speculated that a disturbance of the noradrenaline transporter could be a cause of reduced cardiac uptake of MIBG, as well as in Parkinson's disease.17
Our data suggest a strikingly high prevalence of orthostatic hypotension in patients with DLB, and orthostatic hypotension seemed almost as reliable a marker as myocardial [123I]MIBG scintigraphy. There have been some reported cases of pathologically established DLB with orthostatic hypotension.33 Moreover, syncope due to autonomic dysfunction is also a feature of DLB.4 In patients with DLB, postganglionic damage of the sympathetic nerves may mainly cause orthostatic hypotension as well as a lack of cardiac MIBG uptake. However, orthostatic hypotension was influenced by many factors such as age related changes, diseases, and drugs. Additional studies with increased sample size are needed to assess the presence, degree, and mechanisms of orthostatic hypotension in DLB.
Patients with DAT also experience autonomic disturbances.44 Orthostatic hypotension is often seen in elderly people and may result from age related physiological changes.45 This may be one of possible explanations of autonomic disturbances of patients with DAT, because orthostatic hypotension was seen in relatively elderly patients with DAT in this study. The lesion responsible for cardiac autonomic dysfunction in DAT is unknown, but a defective central control of the autonomic nervous system is a possible explanation. In fact, pathological lesions and neurochemical changes have been found in the hypothalamus and brain stem of patients with DAT.46 47 Regardless of autonomic dysfunction, the mean value of the H/M ratio in the DAT group is similar to those found for a group of normal controls in our former study.6 17 27 The successful MIBG accumulation in patients with DAT in this study supports the hypothesis that the cardiac autonomic dysfunction in such patients might be due to defective central regulation or age related physiological change, or both.
In conclusion, this study has documented myocardial imaging with [123I]MIBG in 14 patients with DAT and 14 patients with DLB. The findings indicated that [123I]MIBG myocardial scintigraphy might detect early disturbances of the sympathetic nervous system in DLB and also give us useful diagnostic information in differentiating DLB from DAT. Further prospective clinicopathological studies, including cardiac MIBG scintigraphy, are needed to confirm this conclusion.
Acknowledgments
The research was presented in part at the 10th International Symposium on the Autonomic Nervous System, Hawaii, 31 October–2 November 1999. We thank Drs Yoshihiro Yasukawa, Kenichi Sakajiri, Kazuo Iwasa, and Hirofumi Miyaji.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Linked Articles
- Editorial commentary