Article Text

Abstract
Objectives: Huntington’s disease (HD) is an inherited autosomal dominant condition in which there is a CAG repeat expansion in the huntingtin gene of 36 or more. Patients display progressive motor, cognitive, and behavioural deterioration associated with progressive cell loss and atrophy in the striatum. Currently there are no disease modifying treatments and current symptomatic treatments are only partially effective in the early to moderate stages. Neural transplantation is effective in animal models of HD and offers a potential strategy for brain repair in patients. The authors report a safety study of unilateral transplantation of human fetal striatal tissue into the striatum of four patients with HD.
Subjects and methods: Stereotaxic placements of cell suspensions of human fetal ganglionic eminence were made unilaterally into the striatum of four patients with early to moderate HD. All patients received immunotherapy with cyclosporin A, azathioprine, and prednisolone for at least six months postoperatively. Patients were assessed for safety of the procedure using magnetic resonance imaging (MRI), regular recording of serum biochemistry and haematology to monitor immunotherapy, and clinical assessment according to the Core Assessment Protocol For Intrastriatal Transplantation in HD (CAPIT-HD).
Results: During the six month post-transplantation period, the only adverse events related to the procedure were associated with the immunotherapy. MRI demonstrated tissue at the site of implantation, but there was no sign of tissue overgrowth. Furthermore, there was no evidence that the procedure accelerated the course of the disease.
Conclusions: Unilateral transplantation of human fetal striatal tissue in patients with HD is safe and feasible. Assessment of efficacy will require longer follow up in a larger number of patients.
- neural transplant
- human fetal tissue
- safety trial
- HD, Huntington’s disease
- MRI, magnetic resonance imaging
- PD, Parkinson’s disease
Statistics from Altmetric.com
Huntington’s disease (HD) is an inherited neurodegenerative disorder typically presenting in midlife with a movement disorder, dementia, and psychiatric manifestations.1 The primary pathology is degeneration of the caudate and putamen2 with the principal cell loss being of medium spiny GABAergic projection neurons. The genetic defect involves an expansion of CAG repeats in exon 1 of a previously unknown gene, htt, located on the short arm of chromosome 4.3 Neither the function of the normal protein product, huntingtin, nor the process whereby an expanded polyglutamine repeat leads to selective neuronal pathology, is yet understood.4–8 Currently, the disease is incurable and leads to death within about 20 years from diagnosis. There has been a considerable amount of effort over the past decade to understand the genetic and molecular mechanisms responsible for the degenerative process in the hope that it will eventually be possible to interfere with this process to effect a slowing or reversal of the disease. However, this approach has not as yet produced a candidate for treatment and so other approaches have been explored including neuroprotective therapies9,10 and replacement of degenerated cells by fetal striatal cells.11
Transplantation of human primary fetal tissue is now well established for cellular repair in Parkinson’s disease (PD), with good evidence of clinical benefit.12,13 There is substantial evidence that a similar approach can yield functional recovery in animal models of HD,14–17 and several clinical trials have started (summarised in references18–22). To date, only a small number of HD patients have received striatal grafts and the approach remains experimental. There are now published reports of safety studies of neural transplantation in HD from three centres: Créteil, France,23 Los Angeles, USA,24 and Tampa, USA.25 One patient from the Tampa trial has come to postmortem examination and good graft survival and integration in the host brain was seen.25,26 However, in view of critical differences in techniques between these centres, and the fact that the tissue preparation and neurosurgical techniques are still being developed, it has been considered mandatory to demonstrate the safety of the specific set of techniques used in our UK based programme. It is probable that modifications and refinements based on accumulating experience in carefully studied individual patients will be needed before contemplating fully randomised control trials, a debate that is currently taking place in PD.27
We report here the first phase of a Medical Research Council supported clinical safety trial of neural transplantation in HD. This is a multicentre UK based trial affiliated to the organisations NECTAR (European Network for CNS Transplantation and Repair) and NEST-HD (The European Network for Striatal Transplantation in HD). NEST-HD includes one group that has already published safety and efficacy data on staged bilateral transplants in five HD patients23,28 and we acknowledge the generous assistance of our French colleagues in the design and implementation of the NEST-UK trial. The UK group consists of six centres, with five involved in patient assessment (Aberdeen, Belfast, Cambridge, Cardiff, and Manchester), one surgical centre (Cambridge), and one centre for PET scanning (the Hammersmith Hospital, London).
The potential risks of neural transplantation of primary human fetal tissue fall into five classes: (1) there is a potential risk of transferring pathological viruses, bacteria, fungi, or prions from infected donor tissues, thus the collection protocol involves exclusion criteria for patients at risk of sexually transmitted viruses and extensive viral screening of all maternal donor serum, including HIV and hepatitis B and C as well as bacterial and fungal screening of donors’ vaginal flora and products of conception; (2) inaccurate dissection and handling of donor tissues could lead to contamination with inappropriate cells, and there is also a theoretical possibility that, even with selective dissection and accurate implantation of the correct fetal tissues, the graft could overgrow causing distortion of or aberrant connections with the host tissue. This has not been a problem in any animal allograft experiment nor in any clinical trials of human fetal tissues in HD to date, but dissection of inappropriate mesenchymal tissues has led to severe adverse reactions in at least two cases of neural transplantation in PD29,30; (3) acute neurosurgical risks, including a well identified but low risk of cerebral haemorrhage after any stereotaxic penetration in the brain; (4) side effects of immunosuppression; (5) other unanticipated adverse effects. In this report we present the safety data at six months on the first four patients with mild to moderate HD who have received unilateral grafts of human fetal striatal tissue.
METHODS
Trial design
The trial design has been influenced by a number of constraints. After extensive discussions with ethical advisors, both at the UK Medical Research Council, who are sponsoring the trial, and in the local research ethics committee at Addenbrooke’s Hospital, Cambridge, it was decided that small numbers of patients should be involved until it can be demonstrated that the procedure does not cause harm and there is preliminary, but convincing evidence of efficacy. In addition, the technical aspects of tissue collection and surgery need to be optimised before involvement of larger numbers of patients. Sham surgery (that is, a burr hole with or without stereotaxic placement of the needle and infusion of vehicle, under general anaesthetic, with blinding of the patients and clinicians as to the patient’s status), as advocated by some for clinical trials of transplantation in PD,31 remains controversial32,33 and has been considered to be inappropriate by the European groups at this early stage of development of transplantation for HD. Furthermore, from both experimental and clinical studies it is known to take at least a year for the donor tissue to develop and connect to the host before the first signs of functional engraftment can be expected, making a two year follow up the shortest period likely to yield any clear conclusions regarding efficacy.
Based on these considerations, we have embarked on a two phase safety study. In phase 1, four HD patients have received unilateral intrastriatal grafts of human fetal striatal tissue with six months of postoperative assessment to record all surgically related complications. Following the absence of serious adverse effects in phase 1 of the trial, phase 2 will examine the safety of bilateral implants. This will involve the four patients in this study being considered for transplants in the contralateral striatum, and a further six patients will receive bilateral implants with a shorter interoperative interval of 2–14 days. Thereafter, all patients will progress to a longer term assessment of efficacy over a minimum of two years after the second transplant.
Patient selection
Inclusion criteria required for the trial patients:
to be over 18,
to have genetically confirmed HD,
to be in the early to moderate stage of the disease,
to have demonstrable motor signs,
to have one close primary informant (typically close relative or caregiver) to assist with patient support and assessment of day to day function,
to have participated for a minimum of one year preoperatively in the NEST-UK programme to assess the longitudinal development of HD and for the validation of reliable neurological, psychological, psychiatric, and imaging instruments to be used in the core assessment of intracerebral transplantation (CAPIT-HD34).
Exclusion criteria:
advanced disease, precluding the ability to give informed consent,
very early disease, such that patients are still employable in their usual occupation,
the presence of other concurrent major illness,
current serious psychiatric symptoms.
Selection of patients was made by a committee comprising representatives from each of the participating patient assessment centres. The final inclusion of patients was by random selection from a larger reference group in the NEST-UK cohort considered to be suitable for transplantation meeting the inclusion and exclusion criteria, although the first four were chosen solely from the Cambridge cohort of patients to facilitate the process of establishing the trial protocols.
Patient consent procedures
Patients were contacted by letter and invited to attend, along with their carer and any other relatives or friends that they wished to include, to discuss whether they would be willing to proceed to a neural transplant. The patient and carer were seen in turn by the neurologist, neurosurgeon, and neurobiologist using semi-structured interviews to discuss the rationale and potential risks and benefits of the procedure. Questions were encouraged and patients were given a detailed letter outlining the trial and the possible identifiable risks. Patients were asked not to give a final answer until they had taken time to discuss the implications of the surgery with family and friends. Preliminary consent was obtained one to three months in advance of the planned transplant date and final consent was given on the day before surgery.
Tissue collection and preparation
Details of the ethical agreements and methods used for tissue collection and preparation are described in Rosser et al,35 and included procedures adapted and modified from previous PD transplant programmes.36,37 Details of the tissue transplanted in each case is shown in table 1. In brief, permission to collect human fetal tissue was obtained from the Cambridge local regional ethics committee following the guidelines of the Royal Commission on Research Use of Fetal Material (the Polkinghorne report38) and subsequent guidance notes of the UK Department of Health.39 Permission to collect tissue was obtained from the maternal donor about one week before tissue collection.35 A high vaginal sample was cultured for pathogens and collection was performed in aseptic conditions during routine terminations of pregnancy that were performed under general anaesthetic with ultrasound guidance. Tissue was collected in hibernation medium and heparin on ice for transportation to the laboratory where it was dissected in phosphate buffered saline supplemented with 0.9% glucose in a tissue culture hood with the aid of a microscope. Striatal tissue was identified and washed four times with phosphate buffered saline/glucose to minimise any contamination from vaginal secretions. Samples were taken at each stage of cell preparation for microbiological culture. Diced pieces of fetal striatum (about 1 mm3) were stored for up to five days in hibernation medium, a technique demonstrated not to have a significant adverse effect on tissue viability.40,41 Tissue from two whole ganglionic eminences derived from one fetus was taken for unilateral transplantation into the striatum of each patient.
Summary of donor tissue preparation
On the day of transplantation, tissue pieces were washed free of the hibernation medium with phosphate buffered saline/glucose and subjected to an enzymatic digestion using trypsin (Worthington, 240U) for 20 minutes. Following this, DNase and trypsin inhibitor were added in a ratio of 1:1:1 and the tissue was spun at 1000 rpm for three to five minutes. The supernatant was removed and the tissue washed in Dulbecco’s modifed Eagle’s medium before adding 0.2 ml of grafting medium and triturating 10–15 times with a 200 μl disposable plastic pipette tip.
Neurosurgery and anaesthesia
The neurosurgical and anaesthetic procedures are described in full in Watts et al.42 All patients were subject to preoperative magnetic resonance imaging (MRI) for presurgical planning of stereotaxic tissue placement. Three of the patients required general anaesthesia for this, two because involuntary head movements interfered with image quality and one because of severe claustrophobia. Patients were allowed to breathe spontaneously using a propofol based technique. Patients were fully monitored with MR compatible monitors. Final planning took place under general anaesthesia on the day of surgery and included both 3T MRI and computed tomography (CT) for co-registration to ensure that there was no distortion of the coordinates on the MRI. For the transplantation surgery patients were ventilated and anaesthetised. Implantation took place through a burr hole using a specially manufactured needle of the minimum diameter compatible with accurate positioning (courtesy of the transplantation programme of the University of Lund, Sweden43). The aim was to deposit six tracts (two in the caudate, two in the anterior putamen, and two in the posterior putamen), and that each tract should comprise five deposits of 2.4 μl of the final tissue suspension deposited at 1 mm–2 mm intervals as the needle was withdrawn (12 μl per track, 60 μl total), although in some cases this had to be modified because of caudate atrophy in the host (see table 1). All injections were made into the non-dominant right hemisphere. Prophylactic antibiotics (1 g cefotaxime and 500 mg metronidazole) were administered intravenously with the premedication and continued thrice daily for 48 hours postoperatively.
Immunosuppression
Preoperatively 200 mg cyclosporin A and 60 mg of prednisolone EC was administered orally about six hours before beginning the procedure. At premedication 1 g methyl prednisolone was administered intravenously along with prophylactic antibiotics, the latter being continued for 48 hours after the transplantation.
“Triple” immunosuppression continued postoperatively and comprised oral cyclosporin A, with a trough therapeutic level of between 200 ng/ml and 300 ng/ml; prednisolone, starting at 40 mg and reducing to 5 mg daily by 12 weeks; and azathioprine at 1.5 mg/kg per day. Osteoporosis prophylactic treatment with Didronel PMO packs was instituted as soon as possible after transplantation. Gastric lining protection was instituted at premedication with ranitidine 150 mg twice daily or omeprazole 20 mg daily. Any longstanding treatments were continued, and septrin prophylaxis was given postoperatively.
Postoperative care
Patients were mobilised on the day after surgery. To enable detailed postoperative assessment, patients were kept in hospital for one week after surgery.
Neurological status, general examination (including blood pressure), biochemistry (renal function, liver function, glucose, trough cyclosporin levels), inflammatory markers (erythrocyte sedimentation rate and C reactive protein), haematological (full blood count) assessment were monitored daily in the first postoperative week. After discharge on day 7, follow up was performed with each of the above assessments weekly for the first six weeks then monthly thereafter. Creatinine clearance assessments were undertaken monthly. This constituted the minimum period of follow up for the safety assessment to six months. We continue to see patients at a minimum of six monthly intervals postoperatively, and will do so for a minimum period of two years after last surgical intervention according to the CAPIT-HD protocol, but with the intention to maintain follow up for life.
Clinical assessment
All patients are assessed on a regular basis using the consensus CAPIT-HD core assessment battery, which comprises the Unified Huntington’s disease rating scale (UHDRS; see below) and additional neuropsychological and neuropsychiatric tests, along with MRI and positron emission tomography (PET) scans at regular defined intervals preoperatively and postoperatively.34 The UHDRS has been established as a valid assessment tool for relevant features of HD, and seems to be appropriate for repeated administration during clinical studies.44 The UHDRS comprises four domains of clinical performance; motor, functional capacity, cognitive functions, and psychiatric abnormalities, all of which are recorded according to specified scales of severity.
In addition, patients received further assessments including timed hand tapping tests, similar to those used in PD,45 along with further computerised neuropsychiatric tests, and computerised neuropsychological tests (CANTAB46), not reported here. In this paper we present the preliminary UHDRS results and the hand tapping test (on the side contralateral to the graft) to evaluate the effect of the transplant in the immediate postoperative period. Further assessments relevant to efficacy (compared with safety) will be the subject of a future report.
Imaging
In addition to the regular general medical assessments and blood tests to monitor immunosuppressive therapy, the assessment protocol also included 3 Tesla MRI imaging for assessment of graft placement and tissue growth and PET scans with the dopamine D2 receptor ligand, (11C)raclopride. PET and MRI scans were performed 12 months before, and just before surgery, and will subsequently be performed at one and two years after transplantation to determine the presence of striatal-like tissue within the grafts.
All patients were imaged in the three months before transplantation using 3 Tesla MR imaging at the Wolfson Brain Imaging Centre (Bruker Medical, Etlingen, Germany). Imaging was repeated immediately befoe surgery with a Leksel stereotactic frame in place42 using the following sequences: T2/proton density (repetition time (TR) 6246 ms, echo time (TE) 120 ms/20 ms, slice thickness 4 mm, 1 mm gap, field of view (FOV) 35.8×16.8 cm, matrix size 512×240); FLAIR (TR 11500 ms, TE 135 ms, inversion time 2214 ms, FOV 35.8×16.8 cm, matrix size 512×240) and a 3D SPGR sequence (TR 20 ms, TE 5 ms, flip angle 20°, FOV 25.6×25.6×25.6 cm, matrix size 256×256×128) giving a spatial resolution of 1×1×2 mm. Imaging was repeated five to seven days postoperatively using the same T2/PD and FLAIR sequences as well as a haemosiderin sensitive gradient echo sequence (TR 1569 ms, TE 30 ms). These sequences were repeated at three and six months post-transplantation.
RESULTS
Data are shown for the six month postoperative period for all patients.
Microbiological screening of patients and donors
Donor microbiology
All maternal blood samples were negative for HIV, hepatitis B and C, toxoplasma, and syphilis serology. CMV IgG (but not IgM) was positive in all of the four maternal donors. Preoperative maternal donor cervical swabs were negative for chlamydia and HSV. Three maternal donors had negative cervical swabs for bacterial growth and one was positive for β-haemolytic streptococcus Lancefield Group B and Candida albicans, which were deemed to be commensal flora and not of pathogenic significance. These organisms were not present at any stage in the fetal tissue samples prepared from that donor.
Recipient virology
Recipient blood samples were also negative for HIV, hepatitis B and C, toxoplasma and syphilis serology. Three of the recipients were positive for CMV IgG, but not IgM. One recipient was negative for CMV and in that case PCR for CMV virus was performed on the hibernated fetal tissue and confirmed to be negative before transplantation.
Clinical course
Preoperatively all patients had normal biochemical (renal function, liver function, glucose, and C reactive protein), haematological (full blood count and erythrocyte sedimentation rate), and clotting tests. Chest radiographs and ECG were also within normal limits for all patients. Dental and anaesthetic assessments revealed no contraindication to undertaking surgery.
All four patients had cyclosporin levels that were in general within the therapeutic target range, indicating compliance. Renal function deteriorated after 6–12 weeks in all four patients as evidenced by a rise in serum creatinine and a fall in creatinine clearance. This was partially reversible by reducing the dose of cyclosporin and resetting the therapeutic range to 100–200 ng/ml (fig 1). Immediately postoperatively all four patients demonstrated a transient leucocytosis (range 13.9–21.8; normal, <11×109/l) without signs of infection or increase of inflammatory markers. This was most probably attributable to the effects of surgery and the introduction of corticosteroids and so no special action was taken. With continued immunotherapy patient 1 developed a mild macrocytic anaemia with a haemoglobin of 11.9 g/l and MCV of 104 fl, which resolved after withdrawal of the azathioprine, and patient 3 developed a mild normocytic anaemia (MCV 94 fl and haemoglobin 10.9 g/l) and a low lymphocyte cell count (0.1×109/l), which also resolved after withdrawal of azathioprine (fig 1).

(A) Postoperative haemaglobin, (B) white cell count, (C) creatinine, and (D) cyclosporin values are plotted for individual patients. Patients 1 and 3 both developed an anaemia that resolved with withdrawal of the azathioprine. In all patients the white cell count rose with corticosteroid administration initially and then fell because of the administration of cyclosporin A and azathioprine. Creatinine concentrations gradually rose, but this was reversible after the reduction of the therapeutic window for cyclosporin A to between 100 ng/ml and 200 ng/ml.
Other incidents are shown in table 2. Patient 2 had an episode of chest pain on day 17. Investigations (ECG, cardiac enzymes, and an exercise tolerance test) excluded ischaemic heart disease but revealed a mixed hyperlipidaemia, with a fasting cholesterol of 10.7 mmol/l, HDL of 1.08 mmol/l, and triglyceride of 8.2 mmol/l (the triglyceride level was too high to allow measurement of LDL), which required introduction of pravastatin and fenofibrate. Patient 3 had an episode of minor accidental head trauma on day 23 when he hit his head on the wall next to the bed while asleep. This resulted in headache, nausea, and vomiting that resolved spontaneously, and CT of the head revealed no abnormalities outside those expected for HD and the surgery. The associated symptoms resolved within 24 hours of the incident. The same patient also had a prolonged hoarse voice after an episode of laryngitis, which on direct laryngoscopy was suggested to be attributable to a left vocal cord palsy. However, there were no local signs of infection or malignancy, CT scan of the head and neck revealed no abnormalities, and the symptoms resolved spontaneously over a period of about six weeks as confirmed by further direct laryngoscopy.
Summary of all adverse incidents
Imaging
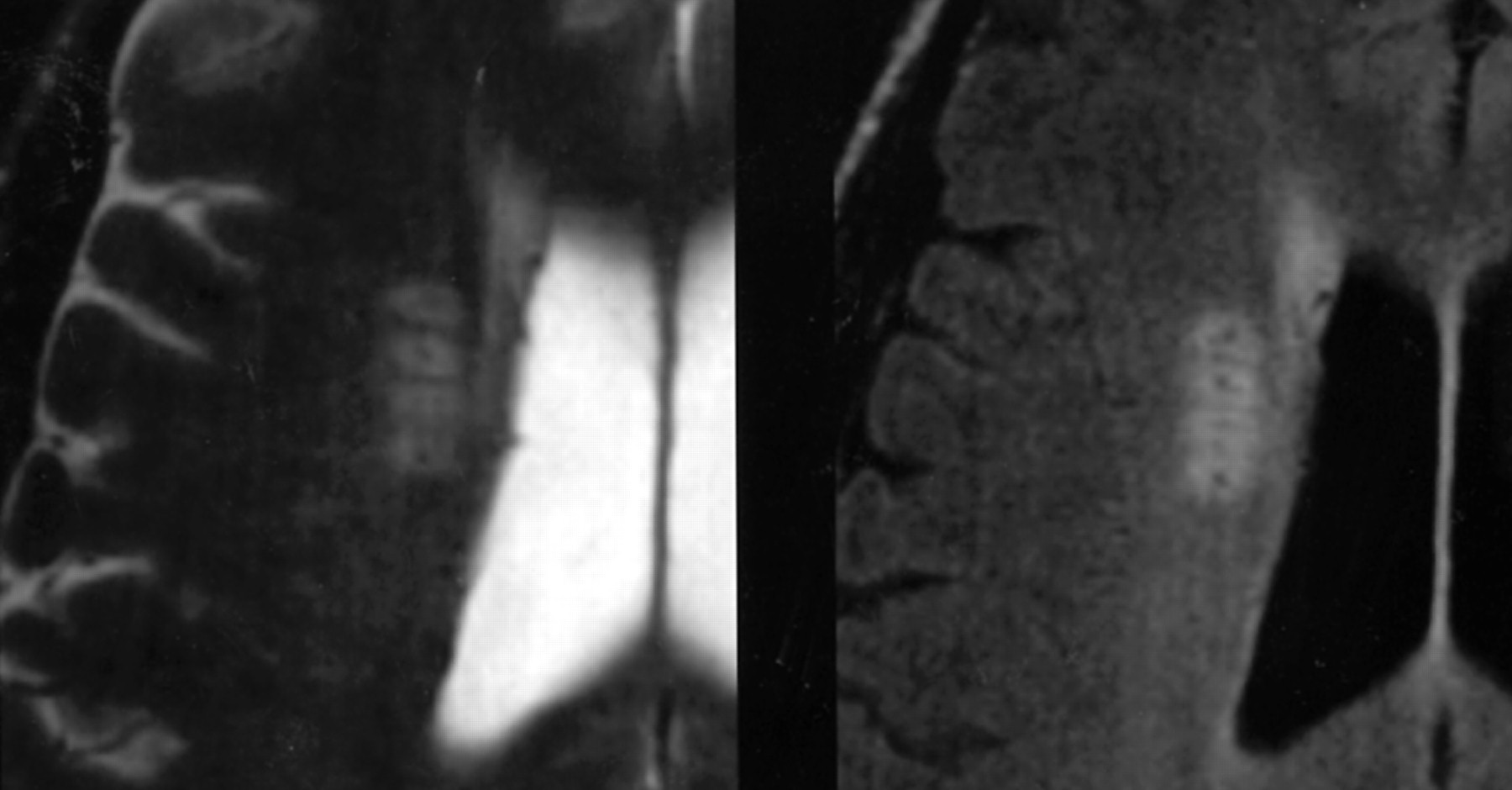
Preoperative MR images on all four patients showed evidence of caudate and putamen atrophy that was mild in three patients and moderately severe in one. The graft deposits could be seen in all four patients on MR imaging immediately after the operation, and thereafter at three and six months. All grafts were well placed within the caudate and putamen and there was no evidence of graft placement outside this area. Figures 2 and 3 show representative images from patients 1 and 2 respectively, and demonstrate the placement of the grafts. In figure 2 T2 hyperintensity is seen in the lateral right putamen in the early postoperative study that relates to the placement of two grafts. The early postoperative magnified T2 weighted and FLAIR sequences in patient 2 (fig 3) clearly demonstrate four graft tracts leading to the right putamen and one tract that leads to the right head of caudate. The area of signal abnormality is reduced in extent by three months, and although there is little change in the area of T2 abnormality seen on the imaged section at six months when compared with the three months study, the total volume of T2 abnormality demonstrated on all slices changed from 111.5 mm3 immediately postoperatively, to 71 mm3 and 164.0 mm3 at three and six months respectively. There has been no indication of uncontrolled or invasive growth of the implanted tissue in any of the four patients at the time of writing.

MRI from patient 1 is shown preoperatively (A), immediately postoperatively (B), and at three months (C), and six months (D) after surgery. T2 hyperintensity is seen in the lateral right putamen in the early postoperative study in patient 1 (B) that relates to the placement of two grafts. The total volume of T2 abnormality demonstrated on all slices changed from 111.5 cm3 immediately postoperatively, to 71 cm3 and 164.0 cm3 at three and six months respectively.
The figure shows the immediate postoperative FLAIR imaging in patient 2 where high signal is seen to surround the needle tracts themselves. In this sequence four deposits in the putamen and one in the caudate can be seen.
UHDRS and hand tapping scores
Figure 4 summarises the UHDRS motor, functional, and cognitive scores, and also hand tapping on the non-dominant side. All patients have been followed up for a minimum of six months postoperatively and for up to 60 months preoperatively using the CAPIT-HD battery of tests, although for clarity of presentation 36 months preoperative data are shown.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A), (B), and (D–F) illustrate a selection of scores from the UHDRS and (C) illustrates timed hand tapping tests done on the side contralateral to the graft. The broken line indicates the time of the neural transplant operation. For the total motor score of the UHDRS (A) an increased score indicates deterioration. For all other scores (B–F), a decreased score indicates deterioration. There were no significant changes in any test after transplantation. Timed tests were introduced late into the protocol and hence only 30 month preoperative data are available.
UHDRS total motor scores appear to deteriorate preoperatively and although there is a trend for them to improve postoperatively this is not significant. Stroop, verbal fluency, symbol digits, and hand tapping do not change significantly in the six months postoperatively. There were no significant psychiatric symptoms reported in either patients or their carers.
DISCUSSION
We report no serious adverse events in a six month follow up of unilateral implantation of cell suspensions of human fetal striatal tissue into four patients with early to moderate HD. There were no adverse events attributable to either anaesthesia or neurosurgery, and the grafts could be identified on MRI scans and were appropriately sited. Those adverse events that were seen were predictable and related to the immunotherapy. The efficacy of the procedure will require further follow up and will be the subject of a future publication. Three previous published reports of neural transplantation in HD patients have also been completed without serious incident in two23,24 but with three of seven patients having complications in the third25 although in these two studies tissue pieces rather than a suspension were implanted. Kopyov et al reported three patients each of whom received bilateral grafts in a single stage operation from multiple donors.24 In this study the grafts survived in all patients, as assessed by MRI, and grew within the implanted striatum without causing any displacement of surrounding tissue. No patients demonstrated any adverse effects of the surgery or the cyclosporin immunosuppression, nor did any patient exhibit deterioration after the procedure, as measured by the UHDRS at six months postoperatively. The same authors have also demonstrated MRS evidence of graft survival.47 As in the present study, the short postoperative follow up does not justify interpretations of efficacy from these data.21,22 Bachoud-Levi et al published a safety report of unilateral implants in five patients23 with a minimum of one year’s preoperative assessment, and a postoperative follow up of one year. Again there were no serious adverse events although these authors report poor compliance with respect to the immunosuppressive therapy. Some psychiatric events were also seen, in particular depression in both patients and carers, around the perioperative period, but neither of these problems seemed to be a significant problem in our study (see below). The same group have now reported evidence of efficacy in four of the five patients after contralateral implantation although the improvement was abruptly lost in one patient after an acute infection after the second implant.29 Recently, Freeman et al25 reported subdural haematomas in three of seven of their patients receiving striatal implants of human fetal tissue. However, it seems that these patients had comparatively advanced disease with greater striatal atrophy than those included in the either the Creteil or Los Angeles series, and it may be that more marked degrees of striatal atrophy should be regarded as a relative contraindication to transplantation at this early stage of clinical trials.
In addition, a recent study in PD31 reported dyskinaesias appearing in several patients two to three years after the completion of the safety study. For reasons outlined elsewhere27 we consider this to be for reasons related primarily to the novel tissue preparation and implantation approach rather than to tissue overgrowth. Adverse outcomes in these two trials do not imply that cell transplantation itself is inappropriate, but rather they emphasise the need for all novel surgical therapies to be firmly based on a sound experimental foundation and evaluated using detailed long term assessment protocols.
On a background of validated tissue preparation protocols35 we found no major microbiological growth in the tissue for transplantation. All four of the maternal donors tested positive for CMV IgG, but CMV IgM levels were not raised in any case. Thus, this most probably indicated previous exposure to CMV (which is a widespread and usually trivial infection), and not an active CMV infection. However, because of the experimental nature of these transplants, and in the light of the fact that the recipients were all in the early to moderate stages of HD and thus experiencing a reasonable quality of life at the time of transplantation, it was considered unreasonable to accept any risk of introducing CMV, particularly while they were receiving immunosuppressive therapy. Hence, in the one CMV negative recipient, PCR was performed to confirm that the fetal sample was not infected with CMV before implantation. A further difference between our study and the previous safety reports is the routine use of hibernation medium for storage of the fetal tissue. We have validated this method for human fetal striatal tissue both in vitro and in vivo for up to eight days,40,41 and in addition a similar approach has been used in clinical trials of neural transplantation in PD.48,49
There were no adverse events attributable to the neurosurgical procedures, and grafts could be identified on MRI scans and were appropriately sited. The scans demonstrated some reduction of signal volume between the immediate postoperative scan and the three month scan and a modest increase in volume between three and six months. The initial reduction in volume at three months is most probably explained by reduction of postoperative oedema, and the increased growth by six months probably represents the growth and development of the graft and is in line with all previous experimental and clinical studies. There have in the past been concerns that striatal tissue grafts might have had a tendency to “overgrow” in that occasional large grafts have been observed after transplants of human fetal striatal tissue into the immunosuppressed rodent hosts.50 However, such concerns have subsided after appropriate volumes of growth seen in subhuman primate to primate allografts,16,51 suggesting that the overgrowth is probably a problem of scaling in that human neurons are programmed for growth within a much larger brain than its rodent host. In addition, many of the signals required to regulate growth may be species specific and not well recognised in the xenograft paradigm. No evidence of uncontrolled growth was seen in these cases, but we intend to continue to monitor graft size in these patients indefinitely.
Most of the adverse events recorded in this study were related to the immunotherapy, in particular renal function test abnormalities that led to adjustment of the treatment. At the time of writing, the patients in this study were still taking immunosuppression, and thus we cannot confirm at this stage that the mild abnormalities of creatinine clearance have returned to baseline levels. In view of the fact that all patients experienced some side effects of the immunosuppression, we recognise that the absolute requirement for immunosuppression will need to be resolved as these studies progress. Indeed, recent experience indicates that for intracerebral allografts, lifelong immunosuppression is not required, and we expect to reduce and then eliminate immunosuppressive treatments from 6 to 12 months after implantation. We also plan to specifically investigate the requirement for immunotherapy in future studies, initially by comparing graft survival in patients given a standard immunosuppressive regimen as in this study with those given an abbreviated regimen. Interestingly, we did not experience the difficulties of compliance experienced by Bachoud-Levi et al,23 which may relate to the fact that patients in our study were generally at an earlier stage of the disease. As the condition progresses, increasing dementia and behavioural changes are likely to adversely affect compliance.
Clinical measures of performance and function were essentially unchanged, with no indication that the procedure produced any exacerbation of the underlying condition. We would not anticipate any evidence of efficacy at this short postoperative time interval, as experience with both experimental animal and clinical studies have demonstrated that a considerable period of time is required for grafts to develop, connect, and start to function.52
In conclusion, this study has demonstrated the safety and feasibility of implanting cell suspensions of human fetal striatal tissue in four patients with early to moderate HD, although we also recognise the need to continue collecting both safety and efficacy data on these patients. This will now enable us to proceed to the next phase of this programme in which patients will receive bilateral grafts. It is recognised that the experimental nature of this work means that there will probably be a requirement for continued modifications of these techniques according to the results of the efficacy study.
Acknowledgments
Dr N Antoun, Mrs R Bentley, Dr T Bak, Dr A Carpenter, Professor D A S Compston, Ms J Deans, Mrs C McFarlane, Mrs R Glew, Mrs K Haynes, Mrs A Kershaw, Mrs J Landucci, Professor A Lever, Mrs J Lucas, Professor N Quinn, Dr D Rubinzstein, Ms H Szatowicz, Mrs P Tyers, Professor D G T Thomas. Staff of neurosurgical theatres, ward A4, the Wolfson Brain Imaging Centre, and the Day Surgery Unit (Addenbrooke’s Hospital and Cambridge University). Trial steering committee: RO Weller (chair), A Björklund, O Quarrel, I Whittle, A Williams. AER is a Lister Institute Fellow. Funding support from MRC Clinical Trials grant G9825903. ISRCTN no 36485475.
Members of the NEST-UK consortium and affiliations R Armstrong, R A Barker, G Berrios, R M Burnstein, T Donovan, S Elneil, M Farrington, C ffrench-Constant, J H Gillard, T Harrower, A K Ho, J R Hodges, R Holt, C Hurrelbrink, H Hutchinson, M Jain, N Kennedy, D K Menon, C Palmer, J Pickard, A Prentice, B J Sahakian, K Smith, S Thornton, A J Wagle, L Watkins, C Watts, T Wreghitt (University of Cambridge); S A Simpson, J Moore (University of Aberdeen); P J Morrison, T F G Esmonde, N Chada, (Belfast City Hospital); S B Dunnett, A E Rosser (University of Cardiff); P Harper, R Harper, A L Jones, R Gentry, H Barton (University of Wales School of Medicine, Cardiff); D Craufurd, J Snowdon, J Thompson (University of Manchester); D J Brooks, N Pavese, P Piccini (MRC Cyclotron Unit, Hammersmith Hospital, London).
REFERENCES
Footnotes
-
Competing interests: none declared.
-
See Editorial Commentary page 612
Linked Articles
- Editorial commentary
- Editorial commentary