Article Text

Abstract
Objective: To evaluate the incidence and the prevalence of neutralising antibodies (NABs) to three interferon beta (IFNβ) products in patients with multiple sclerosis (MS).
Methods: Sera were tested from 125 patients with relapsing-remitting MS. Patients were treated with IFNβ-1b (Betaferon, n = 29) 8 MIU subcutaneously every other day, IFNβ-1a (Avonex, n = 44) 30 μg intramuscularly once weekly, or IFNβ-1a (Rebif, n = 36) 22 μg subcutaneously three times weekly for 6 to 18 months. An additional 16 patients were treated with Rebif 22 μg intramuscularly once or twice weekly. NABs were assessed using the cytopathic effect assay before treatment and every three months during treatment. Patients with two or more consecutive positive samples were considered to be persistent NAB positive (NAB+).
Results: At baseline, no patients were NAB+. NABs developed during the first three months of treatment and continued to develop until month 18. Over 18 months of treatment, the risk of being persistent NAB+ was 31% for Betaferon, 15% for Rebif, and 2% for Avonex (Betaferon versus Avonex, p = 0.001; Betaferon versus Rebif, p = 0.19; Rebif versus Avonex, p = 0.04). In all patients with one or more NAB+ samples, the risk of becoming NAB+ was 38% for Betaferon, 18% for Rebif, and 7% for Avonex (Betaferon versus Avonex, p = 0.0007; Betaferon versus Rebif, p = 0.10; Rebif versus Avonex, p = 0.07). At month 18, the prevalence of persistent NAB+ patients was 31.6% for Betaferon, 18.7% for Rebif, and 4% for Avonex. Numbers of NAB+ patients observed were similar with intramuscular Rebif and with subcutaneous Rebif.
Conclusion: The three IFNβ preparations have different degrees of immunogenicity, with Betaferon producing the highest incidence of NABs and Avonex the lowest. These differences should be considered by neurologists when selecting treatment for their patients with MS because NABs can reduce both bioavailability and clinical efficacy of IFNβ.
- interferon beta
- multiple sclerosis
- neutralising antibodies
- CPE, cytopathic effect
- EDSS, expanded disability status scale
- IFNβ, interferon beta
- LU, laboratory units
- MS, multiple sclerosis
- NAB, neutralising antibody
- PRISMS, prevention of relapses and disability by interferon β-1a subcutaneously in multiple sclerosis
- WHO, World Health Organization
Statistics from Altmetric.com
- CPE, cytopathic effect
- EDSS, expanded disability status scale
- IFNβ, interferon beta
- LU, laboratory units
- MS, multiple sclerosis
- NAB, neutralising antibody
- PRISMS, prevention of relapses and disability by interferon β-1a subcutaneously in multiple sclerosis
- WHO, World Health Organization
Patients with multiple sclerosis (MS) can develop neutralising antibodies (NABs) during treatment with interferon beta (IFNβ) products: IFNβ-1b (Betaferon; Schering AG, Berlin, Germany),1,2 IFNβ-1a (Avonex; Biogen, Inc, Cambridge, UK),3,4 and IFNβ-1a (Rebif; Ares-Serono, Basel, Switzerland).5 The presence and concentration of NABs may be clinically important in the management of patients treated with IFNβs because NAB-positive (NAB+) patients have low or undetectable serum concentrations of IFNβ.6 Furthermore, NABs reduce or abolish IFNβ bioavailability7–10 and NABs have been shown to reduce the therapeutic efficacy of IFNβs.1,2,5,9,11–16
The reported percentages of NAB+ patients observed in studies of individual IFNβs vary considerably.1–3,5,9,17–21 However, a direct comparison of the percentages of NAB+ patients reported in these studies is not possible because of differences in assay methods in different laboratories, including differences in the following parameters: type of assay used to detect NABs; methods used to represent neutralisation potency; criteria for determining NAB positivity; three month versus six month time points for measurement; and treatment duration.
The present study was conducted to determine the incidence and prevalence of NABs in serum samples from patients with MS who were treated with Betaferon, Avonex, or Rebif for 6 to 18 months. NABs were quantified every 3 months using the cytopathic effect (CPE) assay in a single laboratory in our MS centre. Hence, NABs were directly compared for the three IFNβ products under controlled conditions in a single laboratory using the same assay procedure.
METHODS
Patients
Patients with clinically definite MS22 were enrolled in the study from May 1995 to July 2000. Patients were included in the study if they were between 17 and 65 years of age, had a relapsing-remitting or secondary progressive course of MS,23 and had an expanded disability status scale (EDSS)24 score of ≤ 5.5. Patients were excluded from the study if they had received prior treatment with an IFNβ product, immunosuppressive treatment during the 12 months before the study, or corticosteroids four weeks before the initiation of the study. Patients who were pregnant or breastfeeding, had other neurological or autoimmune diseases, or had infectious conditions were excluded from the study. Before enrolment, all aspects of the study protocol were reviewed with each patient and informed consent was obtained.
Procedure
Eligible patients were screened for the presence of NABs before (baseline) and every 3 months during IFNβ treatment for up to 18 months. Patients were treated with one of the three commercially available IFNβ preparations: Betaferon 8 MIU subcutaneously three times weekly, Avonex 30 μg intramuscularly once weekly, or Rebif 22 μg subcutaneously three times weekly. An additional subgroup of patients was treated with Rebif 22 μg intramuscularly once or twice weekly. Patients were not randomly assigned to treatment because the three IFNβs became available in Italy at different times: Betaferon in February 1995, Avonex in August 1997, and Rebif 22 μg in December 1998. Moreover, all the patients treated with Avonex had an EDSS score ≤ 3.5 because the Avonex phase III study included patients in this score range.3 Blood samples were collected every 3 months at least 36 hours after IFNβ injection, then serum was inactivated for 30 minutes at 56°C before being stored at −80°C until assayed.
Two categories of NAB positive (NAB+) patients were identified. The first category consisted of all patients who had one or more positive sample. The second category, a subset of the first category, consisted of patients who had two or more consecutive NAB+ samples, referred to as “persistent” NAB+.
Cytopathic effect assay
The CPE assay was used to detect NABs because it has been recommended by the World Health Organization (WHO).25 A549 cells (human lung carcinoma cell line) were plated in a monolayer on to 96 well tissue culture plates at a mean concentration of 70 000 cells/100 μl and incubated overnight. Serum samples were diluted, mixed with one of the three IFNβ preparations at a final concentration of 10 IU/ml, and incubated for one hour. One hundred microlitres of the serum-IFNβ mixture was incubated with A549 cells for 24 hours. Cells were then infected with encephalomyocarditis murine virus and viable cells were quantified 24 hours later by staining with crystal violet in 20% ethanol. The dye taken up by the cells was eluted with 33% acetic acid and its absorbance was measured in a densitometer at 620 nm.18 Controls for viral activity, cellular viability, and titration of the IFNβ preparation were performed in each set of CPE assays for NAB detection.
According to WHO recommendations, data from the neutralisation assay are reported as the reciprocal of the highest dilution of serum inducing 50% neutralisation (that is, neutralising 10 U/ml of IFN activity to an apparent 1 U/ml of activity). The neutralisation titre of a serum sample was calculated according to Kawade's formula26 and expressed in laboratory units (LU). A concentration of ≥ 20 LU/ml is generally considered the threshold for positivity. However, the present study used thresholds of both ≥ 5 and ≥ 20 LU/ml because the lower limit of detection for our CPE assay was 2.5 LU/ml. The IFNβs used as reference or calibration standards in the CPE assay were the commercially available preparations of Betaferon, Avonex, and Rebif intended for clinical use.
Statistical analysis
The percentage of patients who developed NABs during each three month period was calculated to determine the incidence of NAB+ patients in each treatment group. The risk of becoming NAB+ was assessed from the incidence of NAB+ patients over sequential three month intervals using Kaplan-Meier analysis, in which patients are included in the analysis until they become NAB+ or drop out of the study. Differences in survival curves between the treatment groups were analysed using the log rank test. Prevalence was computed from the number of patients presenting as NAB+ in cumulative three month periods during the study. Prevalence was calculated from baseline to 3, 6, 12, 15, and 18 months of treatment. Differences in the prevalence of NAB+ samples between the treatment groups were analysed using Fisher's exact test. All statistical analyses were performed with GraphPad Prism software, version 3.0 (GraphPad Software Inc, San Diego, California, USA). All reported p values are based on two tailed statistical tests, with a significance level of 0.05.
RESULTS
Patients
One hundred twenty five patients were enrolled in the study. Twenty nine patients received Betaferon, 44 patients received Avonex, and 36 patients received Rebif. A subgroup of 16 patients received Rebif intramuscularly once (6 patients) or twice (10 patients) weekly. Follow up was comparable among the treatment groups. All patients (n = 125) completed six months of treatment and were included in the analyses of baseline, month 3, and month 6. Sixty patients (48%) completed 18 months of treatment: 19 of 29 patients (65%) in the Betaferon group, 25 of 44 patients (57%) in the Avonex group, and 16 of 36 patients (44%) in the Rebif subcutaneously group. The mean treatment duration for all groups was 15 months, and 675 serum samples were available for analysis (77 samples were not available). Sixty five of 125 patients (52%) did not have a complete follow up; 50 patients were still receiving treatment when the study ended; 15 of 125 (12%) discontinued the treatment because of disease progression (five patients), side effects (five patients), pregnancy (one patient), and personal choice (four patients). All the dropout patients were NAB negative.
Table 1 shows the baseline demographic and clinical characteristics of patients. There were no significant differences between groups in demographic or clinical characteristics at baseline with the exception of a lower EDSS score of patients treated with Avonex. The majority of patients (71%) were women and the mean age of all patients was 36.6 years. No patients tested positive for NABs at baseline.
Patient demographic and clinical characteristics
NAB titre ≥ 20 LU/ml
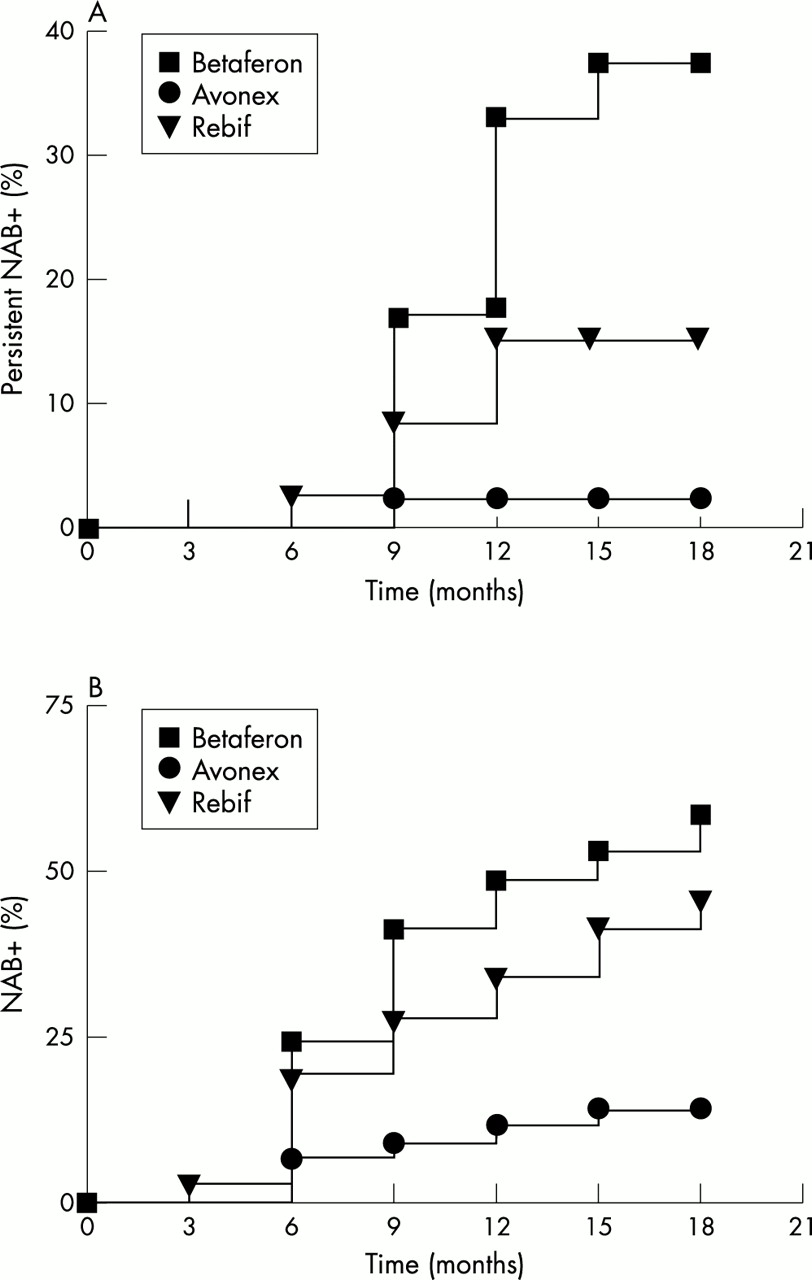
Table 2 presents the incidences of all NAB+ patients and persistent NAB+ patients with an antibody titre ≥ 20 LU/ml for each treatment group. NABs were first detected during the first 3 months of treatment and continued to appear throughout the 18 months of treatment. Of 21 patients who developed NABs during the 18 month study, 19 (90%) developed NABs during the first year of treatment, 16 (84%) of these during the first nine months of treatment. The risk of becoming persistent NAB+ during 18 months of IFNβ treatment was 31% with Betaferon, 15% with Rebif, and 2% with Avonex (fig 1A). The risk of becoming persistent NAB+ was significantly lower for Avonex than for either Betaferon (p = 0.001) or Rebif (p = 0.04). There was no difference in the risk of developing NABs between Betaferon and Rebif (p = 0.19). In an analysis that included patients with one isolated NAB+ sample (fig 1B), the risk of becoming NAB+ increased for all groups and was 38% with Betaferon, 18% with Rebif, and 7% with Avonex (Betaferon versus Avonex, p = 0.0007; Betaferon versus Rebif, p = 0.10; Rebif versus Avonex p = 0.07).
Incidence (Inc) and prevalence (Prev) of neutralising antibodies (NABs) (titre ≥1:20) in patients with multiple sclerosis treated with interferon beta

Kaplan-Meier curves for risk of having (A) two or more consecutive samples positive for neutralising antibodies (persistent NAB+) and (B) one or more positive samples (NAB+) using a titre ≥20 LU/ml as the threshold for positivity.
The prevalence of NABs was significantly higher in Betaferon treated patients than in Avonex treated patients at all cumulative time points after month 3 for all NAB+ patients and for persistent NAB+ patients (p = 0.0002 to p = 0.03; table 2). At month 18, the cumulative prevalence of persistent NAB+ patients was 31.6% in the Betaferon group compared with 4% in the Avonex group. Patients treated with Rebif had a cumulative prevalence of 25% and 18.7% after 18 months for all NAB+and persistent NAB+, respectively. There was no significant difference between Rebif and either Betaferon or Avonex.
NAB titre ≥ 5 LU/ml
Table 3 shows the incidence of NAB+ patients with the threshold for positivity defined as a NAB titre ≥ 5 LU/ml (table 3, fig 2A). The data obtained were consistent with those of NAB titre ≥20 LU/ml. A significantly lower risk of becoming persistent NAB+ was observed in the Avonex group than in either the Betaferon group (p = 0.0002) or the Rebif group (p = 0.047); the difference between Betaferon and Rebif approached significance (p = 0.068). In an analysis of the risk for having one or more NAB+ samples, a significantly lower risk of developing NABs was observed in the Avonex group than in either the Betaferon or the Rebif group (p = 0.0001 and p = 0.003, respectively). Similar to the data for titre ≥ 20 LU/ml, there was no significant difference in the risk of NAB development between Betaferon and Rebif treatments (fig 2B).
Incidence (Inc) and prevalence (Prev) of NABs (titre ≥1:5) in patients with multiple sclerosis treated with interferon beta

{kind=link}
{kind=link}
Kaplan-Meier curves for risk of becoming (A) persistent NAB+ and (B) NAB+ using a titre ≥5 LU/ml as the threshold for positivity.
The prevalence of NABs was also evaluated for all NAB+ patients and the subgroup of persistent NAB+ patients having an antibody titre ≥ 5 LU/ml (table 3). As expected from this lowered detection threshold, the prevalence of NAB+ patients was higher across all treatment groups at each interval for both categories of patients (table 3). The prevalence of NAB+ patients and persistent NAB+ patients was significantly greater in the Betaferon group than in the Avonex group (p < 0.0001 to p = 0.03). In the Rebif group, the prevalence of NABs in all patients and persistent NAB+ patients was 50% and 18.7%, respectively, but there was no significant difference between the Rebif group and either the Avonex or the Betaferon group.
NABs in patients treated with intramuscular Rebif
A subgroup of 16 patients were treated with Rebif 22 μg intramuscularly once or twice weekly. The route of administration of Rebif did not affect the development of NABs. The incidence of persistent NAB+ patients in this subgroup was 18.7%, which was similar to the incidence observed in patients who received Rebif 22 μg subcutaneously three times weekly (19.7%). Two of the three NAB+ patients were treated with Rebif 22 μg intramuscularly once weekly, whereas the third patient received Rebif 22 μg intramuscularly twice weekly.
DISCUSSION
The present study directly compared the incidence and prevalence of NABs with the three types of IFNβs available in Europe for the treatment of relapsing MS. Results showed that the three IFNβ preparations differ in their ability to induce NABs in patients with MS. A significantly lower incidence of NAB+ patients was observed with Avonex than with either Betaferon or Rebif for both definitions of NAB positivity (one or more positive samples and two ore more positive samples). The cumulative risk of becoming persistent NAB+ with Betaferon was double that of Rebif (31% v 15%) and over 10-fold greater than that for Avonex (31% v 2%). The cumulative risk of becoming persistent NAB+ with Rebif was approximately 7-fold greater than that for Avonex (15% v 2%). Hence, Betaferon was more immunogenic than Rebif and Rebif was more immunogenic than Avonex. As expected, lowering the threshold criteria for NAB positivity from a detection limit of ≥ 20 LU/ml to ≥ 5 LU/ml increased the incidence of NABs in each treatment group; however, patients treated with Avonex still had a significantly lower risk of developing NABs than did patients treated with Betaferon or Rebif.
The presence of NABs is important in the evaluation of IFNβ efficacy in the treatment of MS. All double blind, placebo controlled, randomised, multicentre trials that established the beneficial effects of IFNβs for the treatment of relapsing MS reported the incidence of NABs.1–5 In these clinical studies of individual IFNβs, the percentage of NAB+ patients ranged from 27.8% to 45% with Betaferon,1,2,27 from 15.9% to 23.8% with Rebif,5,18 and from 2% to 22% with Avonex.3,4 The findings of the present study are generally consistent with the results of these studies, with the exception that the percentage of NAB+ patients observed in the phase III trial of Avonex was substantially higher (14–22%).3 In the open label safety extension of the phase III Avonex trial,9 the percentage of NAB+ patients decreased to 5%; the decrease in NABs from the phase III study was attributed to a modifications of the manufacturing process to reduce the amount of IFNβ-1a aggregates by changing the excipients in the final product.9 The low incidences of NAB+ patients found in our study and in a recent study of Avonex in monosymptomatic patients (2% NAB+ patients)4 are consistent with the idea that the available Avonex preparation is less immunogenic than that used in the phase III trial.9
The apparent rank order of immunogenicity of the three IFNβ preparations in the present study is consistent with a study by Ross et al,21 which compared the immunogenicity of all three IFNβs in one laboratory using an antiviral neutralisation bioassay. This study found that Betaferon was more immunogenic than IFNβ-1a, and among IFNβ-1a products, Rebif was more immunogenic than Avonex. In another study by Kivisäkk et al,20 similar NAB+ threshold criteria were applied to compare NAB development with Betaferon and Avonex using a CPE assay in an independent laboratory. In this study, the percentage of NABs was 44% with Betaferon and 5% with Avonex in patients treated from 7 to 24 months.20
The CPE assay is internationally recognised for quantification of the neutralising activity of IFNβs.25 A titre ≥ 20 LU/ml is generally considered to be the threshold for NAB positivity and has been used in most studies.1,2,5,8,18,20,28–30 Another approach to establishing a threshold for an upper limit of normal is to assess the lowest value detectable in IFNβ treated patients but not in healthy controls or in untreated patients with MS. The test used in the present study has a lower limit of sensitivity of 2.5 LU/ml, and none of the patients had a concentration higher than 5 LU/ml before IFNβ treatment. Consequently, our data were stratified and analysed based on two thresholds, ≥ 5 and ≥ 20 LU/ml. Decreasing the threshold for positivity or using a method with a higher sensitivity increases the number of patients detected as positive. For example, Ross et al21 used a sensitive method (to 3 LU/ml) and found that most patients treated with IFNβ produced IFNβ antibodies, with 40% to 75% of patients NAB+. To date, it is not known whether the threshold for NAB positivity in the CPE assay should be 5 LU/ml or 20 LU/ml because the lowest NAB titre that interferes with the therapeutic efficacy of IFNβ has not been identified. However, it is noteworthy that a titre between 5 and 20 LU/ml decreases IFNβ bioavailability and a titre > 20 LU/ml abolishes bioavailability.8
Fluctuation of NAB positivity is possible and the disappearance of NABs after some years of treatment has been described.16 Our study lasted 18 months, too short a follow up period to analyse NABs seroconversion. However, in the group of 14 persistent NAB+ patients (with titre > 20 LU/ml), all the samples were positive during the follow up, apart from two samples from the same patient in which positive determinations always showed a titre < 38 LU/ml.
There are several potential reasons for the differences observed between the three IFNβs in their ability to induce NABs. IFNβ-1b differs from IFNβ-1a in several respects, such as biochemical structure, dose, dosing frequency, route of administration, and vehicle.6,19,20 One or more of these factors may be responsible for the increased immunogenic properties of Betaferon compared with IFNβ-1a (Rebif or Avonex). However, since IFNβ-1a is identical to natural IFNβ, whereas IFNβ-1b has been modified biochemically,31 it is likely that biochemical structure is an important aspect in determining the high immunogenicity observed with Betaferon. The risk of developing NABs was also higher with Rebif than with Avonex; however, these two IFNβ products have the same biochemical structure. It can be hypothesised that differences in dose or route of administration affect immunogenicity. However, data from the present study do not support this hypothesis because the incidence of NABs did not differ between groups of patients treated with Rebif 22 or 44 μg intramuscularly weekly and those treated with Rebif 66 μg subcutaneously weekly. Hence, differences in immunogenicity between Avonex and Rebif may depend on differences in drug excipients. The relation between excipients and immunogenicity of IFNβ has not been studied, but Rudick et al9 suggest that a modification of the Avonex excipient caused a reduction in NAB+ patients.
In contrast with the study of Antonelli et al,18 in our study the degree of disability did not seem to be a factor influencing the capacity to produce NABs, although the Avonex treated patients presented with a lower baseline EDSS score. In fact, NAB negative patients and persistent NAB+ patients did not differ in baseline EDSS score, regardless of whether Avonex treated patients were included in the analysis. Moreover, NAB negative and persistent NAB+ patients had comparable disease durations.
As the majority of NABs appear during the first year of treatment, their clinical effects are more evident if the follow up is longer than two years. This concept is clearly shown by the PRISMS (prevention of relapses and disability by interferon β-1a subcutaneously in multiple sclerosis) study, which showed no significant impact of NABs during the first two years of the study, but a significant impact on both clinical and magnetic resonance imaging measures when the follow up was four years.5,32 It should be noted that NABs have a relevant impact on MS in terms of both the number of patients involved and the magnitude of clinical effects. The PRISMS-4 study clearly showed that NAB+ patients treated with Rebif 44 μg three times weekly had a mean relapse rate of 0.81 and a 17% increase in burden of disease on magnetic resonance imaging, whereas NAB negative patients had 0.50 relapse rate and 8% decrease in burden of disease. This clinical effect was observed in one of seven patients treated with Rebif 44 μg and in less than one of five patients (23%) treated with Rebif 22 μg.
In conclusion, this study compared the relative risk for developing NABs in patients with MS treated with one of three different IFNβ preparations using a single, sensitive assay under controlled conditions in one central laboratory. The rank of relative risk was found to be Betaferon ≥ Rebif > Avonex. NABs can appear early during the course of MS treatment, persist for several years before disappearing,16 decrease IFNβ bioavailability,8,9 and reduce or abolish the clinical efficacy of IFNβs.1,2,5,16 Hence, the relative risk of developing NABs should be considered when selecting the appropriate IFNβ treatment, both for newly diagnosed MS and for those already receiving treatment for MS.
Acknowledgments
We thank Prof G Antonelli for teaching us the CPE method; we are indebted to Rita Guerrieri and Angela Zaccaria for their expert nursing assistance. This work was supported by Piedmont Health Service, AISM (Associazione Italiana Sclerosi Multipla), ARB (Associazione Ricerca Biomedica), and Fondazione Cavalieri Ottolenghi.
REFERENCES
Footnotes
-
Competing interests: AB, SM, GO, PBC, MC, and EM have been reimbursed by Farmades, Serono, and Dompé Biotech for attending several conferences; AB received fees for speaking from Serono, Dompé Biotech, and Biogen; and AB received funds for research and for members of the staff from Serono and Dompé Biotech. Farmades is the Italian distributor of Betaferon; Serono is the manufacturer of Rebif, Biogen is the manufacturer of Avonex, and Dompé Biotech is the Italian distributor of Avonex.