Article Text

Abstract
Objectives: To elucidate the factors associated with severity of cardiac sympathetic nerve involvement in idiopathic Parkinson’s disease (PD).
Methods:123I-metaiodobenzylguanidine uptake was examined in 88 patients with PD. The ratio of the uptake in the heart (H) to that in the mediastinum (M) (the H/M ratio) was calculated and correlated with age at onset, age at examination, and disease severity and duration. Twenty five healthy people were also examined as a control.
Results: There was a mild but significant negative correlation between H/M ratio and age at onset (early, r = −0.33, p = 0.002; delayed, r = −0.34, p = 0.001) and between Hoehn and Yahr (H-Y) stage (early, r = −0.30, p = 0.006; delayed, r = −0.32, p = 0.003). There was no significant correlation between disease duration and H/M ratio. When patients with PD were classified into four subgroups on the basis of age at onset (> 62 or < 62 years) and disease severity (H-Y > III or H-Y ⩽ II), the median H/M ratio of the older and more severe group was significantly lower than that of the younger and less severe group (p = 0.005).
Conclusion: This study suggests that late onset, high severity PD is associated with myocardial sympathetic dysfunction.
- 123I-metaiodobenzylguanidine
- Parkinson’s disease
- age
- onset
- H-Y, Hoehn and Yahr
- MIBG, 123I-metaiodobenzylguanidine
- PD, Parkinson’s disease
Statistics from Altmetric.com
123I-metaiodobenzylguanidine (MIBG) is a physiological analogue of noradrenaline that traces the uptake and transport of noradrenaline in presynaptic sympathetic nerve terminals and subsequent vesicular storage.1 Myocardial MIBG scintigraphy has been used to evaluate cardiac sympathetic nerve endings in both cardiac and various neurological diseases.2–5 In idiopathic Parkinson’s disease (PD), myocardial MIBG uptake is significantly reduced even without apparent autonomic failure, which enables early diagnosis of the illness.6–17 Several studies involving small numbers of patients have suggested that duration and severity influence MIBG uptake in PD.12,13,15 However, the factors proposed to be involved differ with the report. Furthermore, no previous study has investigated the effect of age at onset on MIBG cardiac uptake. In the present study, we examined the relations between myocardial MIBG uptake and age at onset, age at examination, disease severity, and disease duration in 88 patients with PD.
PATIENTS AND METHODS
From January 1997 to October 2001, myocardial MIBG scintigraphy was performed in 100 patients with PD according to the criteria of the United Kingdom Brain Bank.18 None of the patients had familial or past histories of heart disease. All patients were examined by routine brain magnetic resonance imaging, and these results were incorporated into the diagnosis. Patients with Parkinson-plus syndrome or drug induced and postencephalitic parkinsonism were excluded. Twelve of the 100 patients with PD onset before reaching 45 years of age were excluded to differentiate autosomal recessive juvenile parkinsonism.19 Thus, 88 patients with PD with the following characteristics were studied: 54 men and 34 women; mean (SD) age of onset 63.5 (9.6) years, range 45–85 years; mean age at examination 68.0 (9.0) years, range 49–87 years; mean disease duration 4.6 (3.6) years, range 1–12 years; and mean L-dopa intake 259 (174) mg. The Hoehn and Yahr (H-Y) scale was used to assess the severity of motor impairment: 10, 27, 40, 9, and 2 subjects were classified into stages I, II, III, IV, and V, respectively, when cardiac MIBG uptake was assessed. As a control group, 25 age matched people with no history of neurological or heart disease (13 men and 12 women, age at examination 66.6 (9.3) years) were enrolled in this study. We obtained informed consent from all subjects.
The 88 patients with PD were subgrouped based on the following cut off values: < 62 years old (younger), > 62 years old (older), H-Y ⩽ II (mild), and H-Y > III (severe). Postural impairment is thought to result from a combined effect of the disease and aging processes, suggesting the widespread involvement of subcortical structures.20 Consequently, patients with PD were classified into four groups: older/severe, older/mild, younger/severe, and younger/mild.
123I-MIBG (111 mBq) was injected intravenously into each subject. The early image of cardiac uptake was taken 15 minutes later and the delayed image three or four hours later. Regions of interest were placed on the whole heart and mediastinum of the front image. The ratio of 123I-MIBG uptake in regions of interest of the heart to that in the mediastinum (H/M ratio) was calculated. The H/M ratios from early and delayed images were evaluated in this study.
The Mann-Whitney U test was used for examining the intentional difference between two groups, the Kruskal-Wallis test was used for examining the intentional difference between three groups, and then Scheffé’s F was used for post hoc testing. The relations between H/M ratio and age at onset, age at examination, and disease duration were analysed using Pearson’s correlation coefficient. The relation between H/M ratio and H-Y scale was analysed using Spearman’s correlation coefficient. Calculations were performed using the statistical software package StatView (Abacus Concepts, Berkeley, California, USA). The level of significance was defined at p < 0.05.
RESULTS
The H/M ratio of all patients with PD was significantly reduced compared with controls in both early (PD, 1.51 (0.32); control, 2.26 (0.19); p < 0.0001) and delayed images (PD, 1.39 (0.33); control, 2.19 (0.20); p < 0.0001).
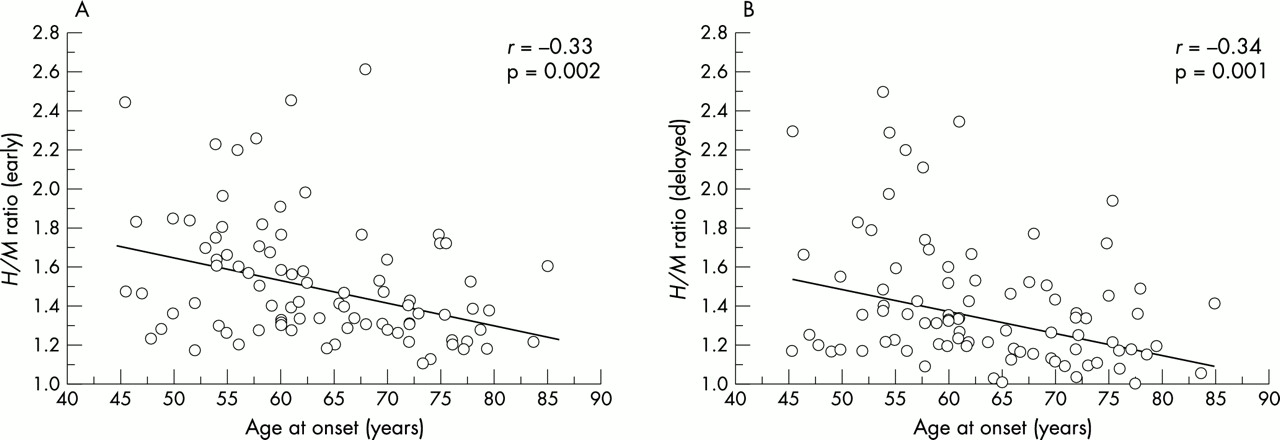
The age at examination was correlated with H/M ratio in patients with PD (early, r = −0.42, p < 0.001; delayed, r = −0.44, p < 0.001; fig 1), while in control subjects this age dependent reduction was not observed (p > 0.5). The age at onset was mildly but significantly negatively correlated with H/M ratio in PD (early, r = −0.33, p = 0.002; delayed, r = −0.34, p = 0.001; fig 2), and the H-Y scale was mildly but significantly correlated with H/M ratio (early, r = −0.30, p = 0.006; delayed, r = −0.32, p = 0.003; fig 3). The disease duration was not, however, significantly correlated with H/M ratio (early, r = −0.15, p = 0.16; delayed, r = −0.20, p = 0.07).
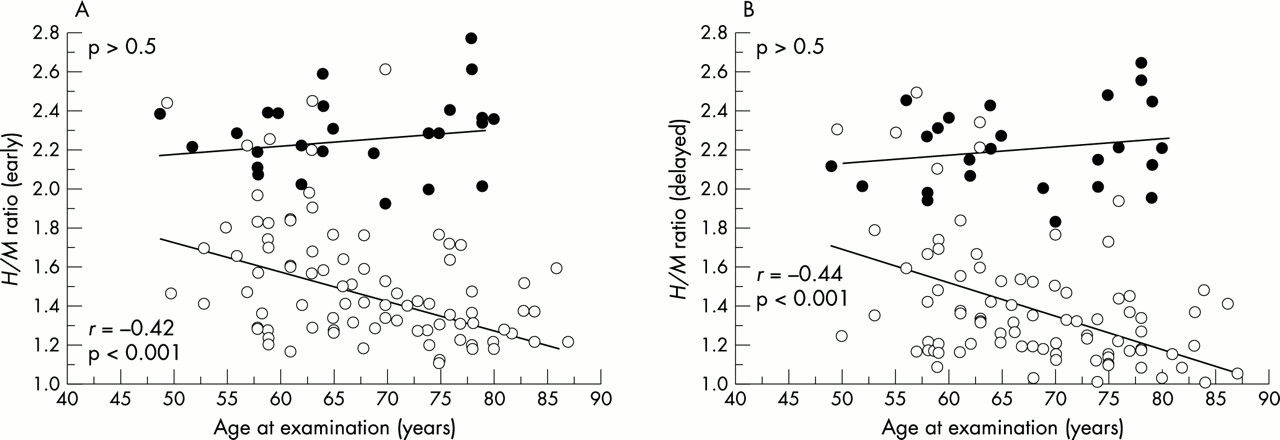
Age at examination had a significant negative correlation with heart to mediastinum (H/M) ratio in Parkinson’s disease (PD) (PD patients: (A) early, r = −0.42, p < 0.001; (B) delayed r = −0.44, p < 0.001) but not in controls (p > 0.5). Open and closed circles represent individual patients with PD and control subjects, respectively.

Age at onset had a slight but significant negative correlation with H/M ratio ((A) early, r = −0.33, p = 0.002; (B) delayed, r = −0.34, p = 0.001). Circles represent individual patients with PD.

{kind=link}
{kind=link}
{kind=link}
Hoehn and Yahr score had a slight but significant negative correlation with H/M ratio ((A) early, r= −0.30, p < 0.01; (B) delayed, r = −0.32, p = 0.005). Circles represent individual patients with PD.
When the patients with PD were classified into the four groups on the basis of age at onset and disease severity, the median H/M ratios of each of these groups were significantly reduced as compared with controls (p < 0.001; table 1). The H/M ratio was lowest in the older/severe group in both early and delayed images of the four groups. The difference in H/M ratio between the older/severe group and younger/mild group was significant (p < 0.005; table 1).
Ratio of 123I-metaiodobenzylguanidine uptake in the heart to that in the mediastinum in four subgroups of patients with Parkinson’s disease and in healthy control subjects
DISCUSSION
Age at onset and H-Y scale are negatively correlated with both early and delayed cardiac MIBG uptake as assessed by the H/M ratio. Furthermore, the combination of higher age at onset and advanced H-Y stage profoundly influenced the reduction of myocardial MIBG uptake in PD. On the other hand, the disease duration was not significantly correlated with either early or delayed MIBG uptake. Both the age at examination and age at onset were negatively correlated with the H/M ratio. The age at examination includes the age at onset and the disease duration, so age at onset has a greater influence on the H/M ratio.
Several possible explanations for the pathophysiology underlying low myocardial MIBG uptake in PD have been proposed. Whether myocardial MIBG uptake reflects sympathetic and systemic autonomic failure has not been verified, and the degree of H/M ratio reduction is not always associated with the presence of orthostatic hypotension conditions.11,15,17 We, however, have previously shown that patients with PD with orthostatic hypotension display supersensitivity to noradrenaline21 and severely decreased MIBG uptake of not only the myocardium but also the lower extremities.7 Recently, Goldstein et al showed that patients with PD with orthostatic hypotension had much lower cardiac uptake of 6-[18F] fluorodopamine than those without the condition.22 Furthermore, they showed that lower 6-[18F] fluorodopamine was seen not only in the myocardium but also in the thyroid and renal cortex in PD with orthostatic hypotension, although we did not measure MIBG uptake in these organs in this study. These findings suggest that the sympathetic nerves are involved more extensively in PD than previously believed. As a possible explanation for the discrepancy between the reduction of myocardial MIBG uptake and orthostatic hypotension in PD, myocardial sympathetic nerve dysfunction would precede generalised sympathetic denervation eliciting orthostatic hypotension. On the other hand, pathological studies have shown that Lewy bodies and Lewy neurites are commonly identified in the cardiac plexus in PD,23 and tyrosine hydroxylase immunoreactive nerve fibres in the heart are greatly decreased in patients with orthostatic hypotension.24 Taken together, the degree of decreased myocardial MIBG uptake is thought to reflect the severity of myocardial sympathetic involvement and to be correlated with systemic sympathetic nerve involvement in PD.
In this study, cardiac MIBG uptake was mildly but significantly correlated with age at onset in PD. In control subjects, however, there were no significant differences in cardiac MIBG uptake in terms of aging. This was in agreement with a previous study by Tsuchimochi et al,25 who reported reduced MIBG uptake in the inferior regions in older patients but no significant decrease in the whole myocardium. They proposed that sympathetic neuronal function in the inferior region may be selectively disturbed with aging. However, we found that sympathetic neuronal function disturbance was more extensively associated with the age at onset of PD. Thus, the negative correlation between age at onset and whole myocardial MIBG uptake was specifically associated with PD, but not with normal aging. Patients with a later onset of PD may have increased motor disability associated with more extensive subcortical involvement.26,27 Furthermore, the degree of dementia caused by the presence of Lewy bodies in cortical areas has been shown to be related to the age at onset.28,29 These reports indicate that a later onset may be associated with widespread multisystem involvement in PD.
We found that cardiac MIBG uptake had a mild but significant negative correlation with H-Y stage. Furthermore, cardiac MIBG uptake was significantly reduced in patients with PD with an H-Y score > III compared with those with an H-Y score ⩽ II. In general, autonomic dysfunction in PD becomes apparent as the disease progresses.30 Our findings indicate that the cardiac sympathetic nerve may be involved in the advancing severity of motor impairment in PD.
Patients with PD often have combinations of motor impairment, cognitive disorder, and autonomic failure during the course of the illness. However, the temporal progression of these three symptoms is heterogeneous among patients. Various factors have been proposed to influence the progression of PD. The present results suggest that patients with PD who have a combination of later onset and more severe clinical stage have increasing cardiac sympathetic nerve impairment in PD. Levy et al31 reported that the increase in risk of dementia in PD was associated primarily with the combined effects of age and the severity of extrapyramidal signs.31 Our findings are similar to those of Levy et al and suggest that later onset PD with high severity comes with an increased risk of early evolution not only to motor and cognitive system involvement but also to myocardial sympathetic involvement.
PD varies between patients in several respects, including age at onset and the rates of progression of both the severity of motor impairment and the involvement of multiple systems. Understanding the progression pattern of PD would provide novel targets for curative treatments on the basis of molecular and environmental studies. However, further prospective studies are needed to determine why age at onset and the severity of motor impairment are associated with reduced myocardial MIBG uptake in PD.