Article Text

Abstract
Objective: To determine long term functional outcome and length of survival of patients undergoing decompressive craniectomy for space occupying infarction of the middle cerebral artery (MCA), and to identify risk factors associated with death and unfavourable outcomes
Methods: Databases of patients undergoing decompressive craniectomy for space occupying MCA infarction compiled at eight neurosurgical departments (1996–2001) were merged, and 188 patients were evaluated. Mortality was calculated by the Kaplan–Meier method. Clinical outcome was rated using the Glasgow outcome scale (GOS). The prognostic impact of patient related covariates on length of survival and the GOS was analysed multivariately.
Results: The unadjusted 3, 6, and 12 month mortality rates were 7.9%, 37.6%, and 43.8%, respectively (median follow up, 26 weeks). In the “best” multivariate model, age >50 years (p<0.02) and the involvement of two or more additional vascular territories (p<0.01) had an unfavourable impact on length of survival. The adjusted six month mortality was as low as 20.0% (no risk factor) and as high as 59.7% (two risk factors). A GOS score of ⩽3 was significantly associated with age >50 years (p<0.0003): 34.9% of the patients ⩽50 years of age achieved a GOS score of >3, as compared with 12.0% of the elderly subpopulation. The side of the infarct did not have prognostic relevance.
Conclusions: Results of surgical treatment in patients <50 years of age undergoing decompressive craniectomy are encouraging. The effectiveness of decompressive craniectomy for patients >50 years remains questionable and should be analysed in the framework of a prospective randomised study.
- cerebral infarction
- outcome
- hemicraniectomy
Statistics from Altmetric.com
About 10–15% of all patients with cerebral infarction in the territory of the middle cerebral artery (MCA) suffer from progressive clinical deterioration because of increasing brain swelling, raised intracranial pressure, and brain herniation. This patient subpopulation constitutes a particularly difficult challenge for clinicians charged with their care.1–3 It has been claimed, for example, that the introduction of aggressive decompressive craniectomy (in an early or delayed fashion) has improved the overall prognosis for many patients.3,4 However, small sample sizes, poorly defined selection criteria, and no proper control groups hamper the validity of the published datasets so far.3–15 Moreover, an exclusive focus on overall prognosis has hindered subgroup evaluation, identification of pretreatment prognostic factors, and adjustment of treatment effects for the influence of treatment-independent prognostic factors. Thus the identification of appropriate comparison groups for evaluating various treatment strategies appears nearly impossible at present.
The present multi-institutional pooled data analysis was undertaken to define long term outcome and to determine which groupings of prognostic factors predict survival and functional outcome in patients with space occupying MCA territory infarction. Selection criteria and the treatment concepts applied were similar in all the participating departments. Decompressive craniectomy was generally undertaken as second line treatment in the case of clinical deterioration after conservative therapy. Thus identification of prognostic factors and quantitative estimation of their influence becomes possible for a relatively large study cohort. The results obtained may provide a standard against which other management strategies for similar patient subpopulations can be measured, and might be helpful in the stratification of patients for further clinical trials.
METHODS
Databases of eight neurosurgical departments were merged, and 213 consecutively treated patients (1996 to 2001) were included for baseline analysis. We excluded patients with bilateral infarcts (n = 2), infarction caused by vasospasm following subarachnoid haemorrhage (n = 4), and with missing long term follow up after surgical treatment (follow up less than two months; n = 19). Early mortality after decompression was not the reason for exclusion of these 19 patients. Thus 188 patients in all were considered for prognostic evaluation.
The following inclusion criteria were used:
-
infarction of >50% of the MCA territory as defined by computed tomography (CT) and/or standard magnetic resonance imaging (MRI), with an acute onset of corresponding clinical signs and symptoms;
-
neuroradiological evidence of local brain swelling such as compression of the basal cisterns and effacement of sulci.
Patients with any previous disabling neurological disease, coma, terminal illness, or secondary parenchymal haemorrhage were excluded. Early coma at the time of admission was not an exclusion criterion.
Standardised conservative management included normalising the blood volume, hyperosmolar treatment (mannitol, glycerol), mechanical ventilation, and analgesic sedation as described previously.4,16 Intracranial pressure monitoring was not undertaken routinely.
Except for three patients who underwent early surgical treatment (presurgical Glasgow coma scale (GCS) score = 15) decompressive craniectomy was used as second line treatment in case of significant neurological deterioration. “Significant deterioration” was defined as a further decrease in consciousness to somnolence or stupor, and/or the development of anisocoria. Informed consent was obtained from the patients’ relatives. Decompressive craniectomy was done by removing parts of the frontal, parietal, temporal, and occipital squama, resulting in a large bone flap with a diameter of 12–14 cm. The dura was opened and enlarged by the implantation of freeze dried cadaver dura or homologous tissue (temporal fascia or galea-periost flap).4
Patient evaluation
Clinical status was rated on admission and preoperatively using the GCS score.17 Neurological signs and symptoms on admission and preoperatively (hemiparesis, anisocoria of pupils, aphasia), pre-existing medical conditions, and risk factors were recorded and used for prognostic evaluation if possible. For outcome rating we used the Glasgow outcome scale (GOS) at the time of discharge and six months later.18 The Barthel index was also used if available. Complications in the postsurgical clinical course were classified as surgery related or disease related events. Only in the case of an unequivocal relation between the surgical procedure and the observed complication was a surgery related side effect assumed.
Statistical analysis
The reference point for this study was the date of the surgical procedure. The unadjusted overall survival rate was calculated using the Kaplan–Meier method, and adjusted survival rates were obtained from the multivariate proportional hazards model.19,20 The following variables were considered for prognostic evaluation: sex, age, anisocoria, GCS score, extension of infarction (MCA territory only v more than the MCA territory), laterality of the infarction, pre-existing medical conditions or risk factors, and time from infarction to surgery. Univariate analysis was done first. Second, the variables that appeared to be important from step 1 were fitted together. Comparison of alternative models was done by computing the maximised likelihood. The “best” model contained only variables associated with survival (p<0.05) after adjustment for the effects of the other variables in the model. Logistic regression analysis was used to analyse the prognostic impact of pretreatment factors on the GOS. For that purpose the GOS was dichotomised. A GOS of ⩽3 was classified as an unfavourable outcome; otherwise a favourable outcome was assumed. The treating institution was included in each of the multivariate models created to detect or exclude institution related selection bias in the pooled dateset. The Barthel index was not used for prognostic evaluation as it was not available for all the patients.
RESULTS
Patient characteristics
The series comprised 188 patients (105 men and 83 women), with a median age of 57 years (mean (SD), 54.3 (12.3) years; range 17 to 78) and a median postsurgical follow up period of 26 weeks (28.0 (32.4) weeks; range 2 days to 188 weeks). Important clinical data on admission and preoperative course are summarised in table 1. The median time interval between the first clinical symptoms and the first hospital admission was two hours. The median GCS score at the time of admission and before surgical treatment was 11 (range 3 to 15) and 8 (range 3 to 15), respectively.
Clinical and neuroradiological characteristics of patients with space occupying infarction of the middle cerebral artery at the time of admission and before surgery
The frequency of risk factors or pre-existing medical conditions is given in table 2. No risk factor was reported in 10.2% of the patients, one risk factor in 30.7%, two risk factors in 31.8%, and three or more in 27.3%. The infarction was thought to be caused by embolism in 47.9%, by stenosis/dissection/occlusion of the internal carotid artery in 32.6%, and by hypercoagulopathy in 2.2%; in 17.3% of the series the aetiology could not be determined. An additional territory beyond the MCA territory was involved in 28.2% of all patients (MCA + anterior cerebral territory in 19.7%, MCA + posterior cerebral territory in 5.3%, and all three territories in 3.2%). The frequency of right sided and left sided MCA strokes was 66.5% and 33.5%, respectively.
Risk factors and pre-existing medical conditions in patients with space occupying infarction of the middle cerebral artery; 30.7% of the patients had one risk factor, 31.8% had two, and 27.3% had three or more
Treatment
The median duration of conservative management was 24 hours (range 2 to 240) and the median overall time from infarction to surgery was 27 hours (range 2 to 240). Overall, 42.4% of the patients suffered from at least one postoperative complication, with pulmonary problems being the most common cause (39% of all complications); 17.8% of the complications were directly related to surgery (table 3). Surgical revision was necessary in four patients (two with epidural haematomas, one with a space occupying hygroma, one with wound infection).
Postoperative complications of patients with space occupying infarction of the middle cerebral artery undergoing decompressive craniectomy
Survival rates and prognostic factors
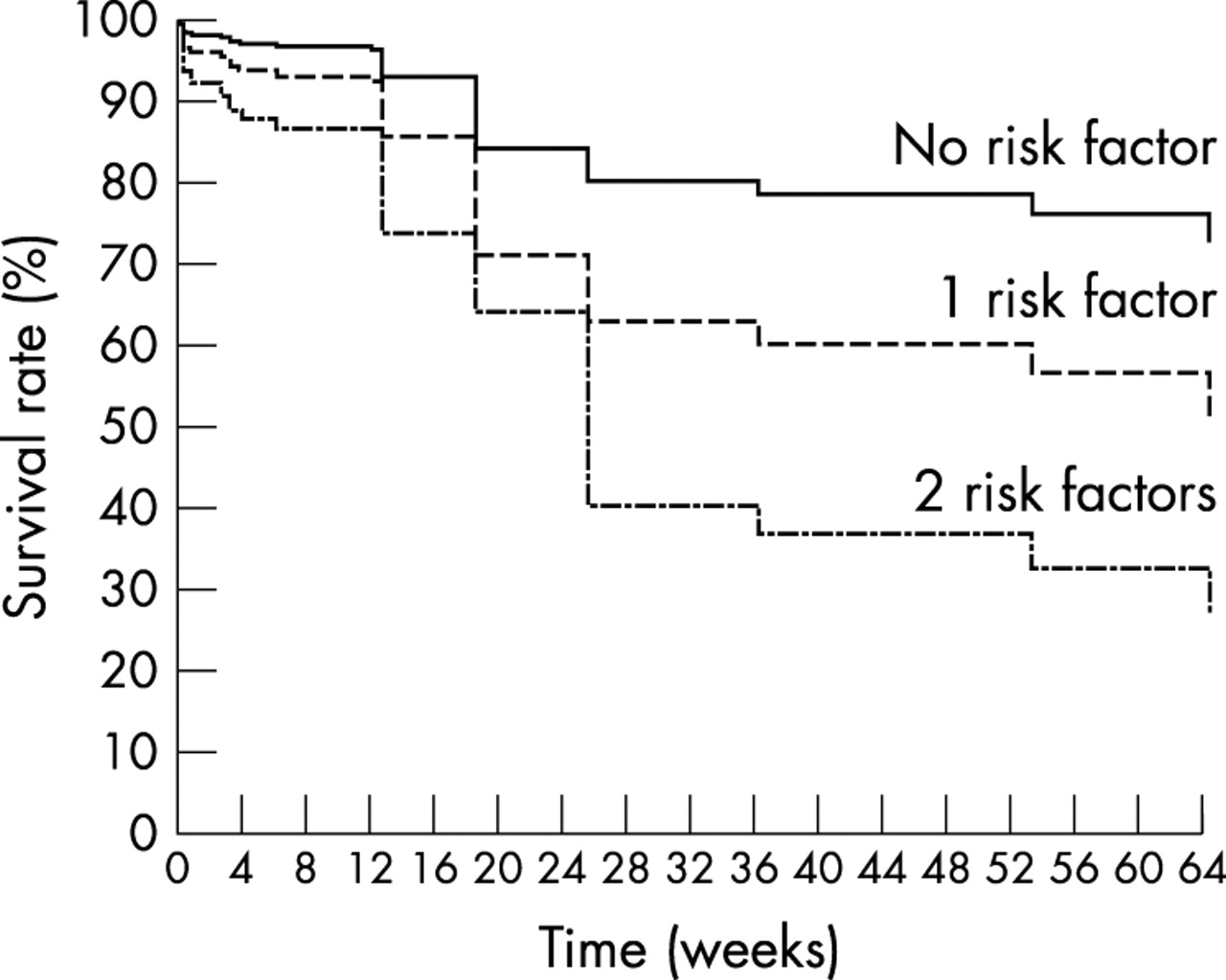
At the time of the last follow up, 58 patients (30.9%) had died. The estimated overall (unadjusted) three, six, and 12 month mortality rates were 7.9%, 37.6%, and 43.8%, respectively (fig 1). Risk factors after univariate analysis were: increasing age (continuously scaled, p<0.02; dichotomised: >50 years, p<0.03); involvement of more than one vascular territory (p<0.01); and an increasing time interval between the onset of clinical symptoms and decompressive surgery (continuously scaled, p<0.03; dichotomised: <39 hours, p<0.03). Though the median GCS score before surgery was not significantly different in the “early” and “delayed” surgery group, the dynamics of deterioration were different in the two groups: patients undergoing early surgery were those with a more rapid decline of the GCS score (0.21 v 0.08 GCS points/h). Non-significant variables were the GCS, sex, number of risk factors, anisocoria, duration of conservative treatment, and the side of the infarct.

Graph showing overall survival of 188 patients after decompressive craniectomy for malignant middle cerebral artery infarction.
In the “best” multivariate model, age >50 years (p<0.02) and the involvement of more than one vascular territory (p<0.01) remained prognostically important (table 4). An alternative model with inclusion of age as a continuously scaled covariate did not achieve a similarly good fit (as expressed by the maximised likelihood). The adjusted six month (one year) mortality rates for patients with 0, 1, and 2 risk factors were 20.0% (21.7%), 40.7% (55.4%), and 59.7% (67.3%), respectively (fig 2). Those three prognostically different classes comprised 41, 116, and 31 patients, respectively. Institution of treatment did not have prognostic relevance in any of the models.
Prognostic factors and survival in patients undergoing decompressive craniectomy for space occupying infarction of the middle cerebral artery.
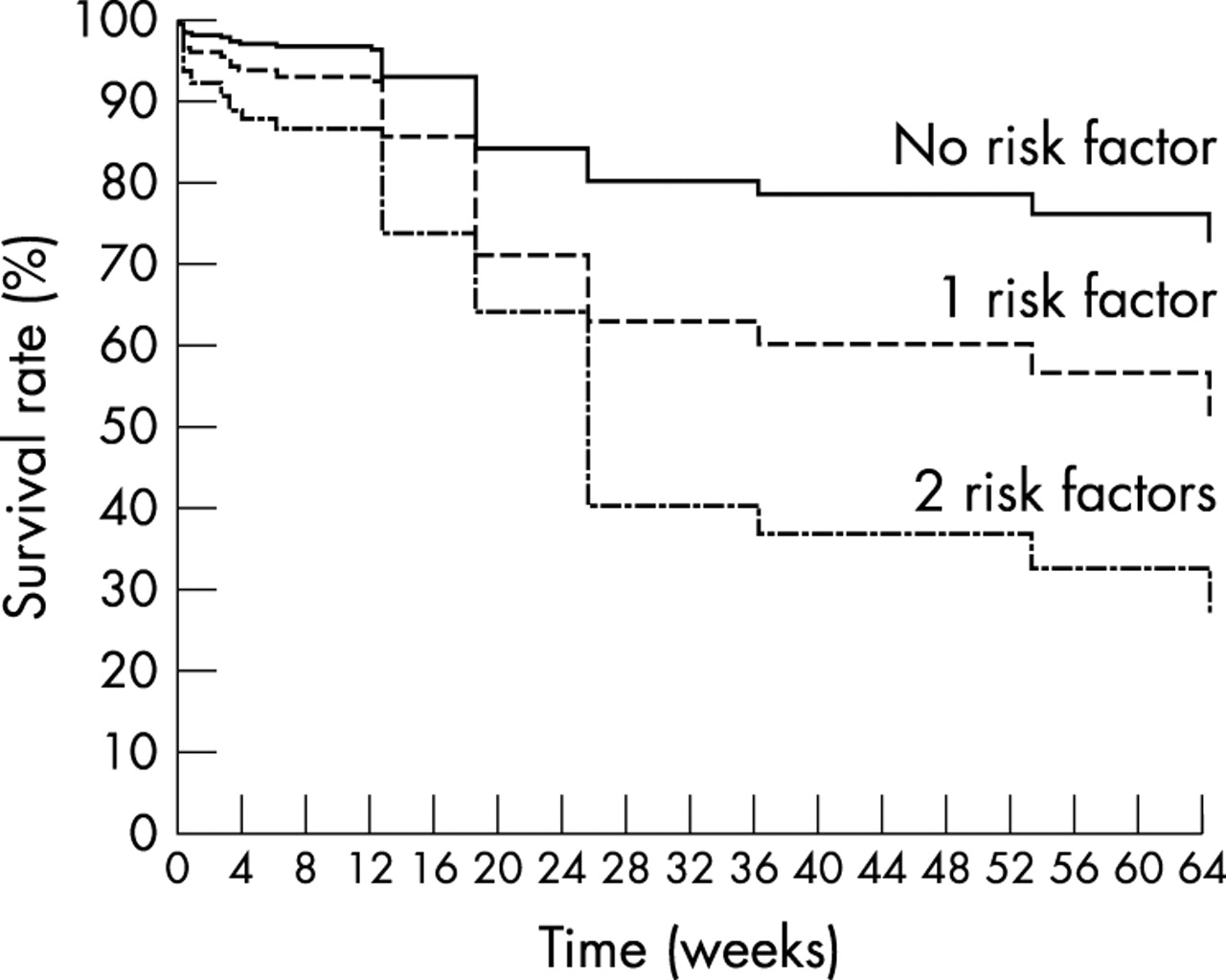
Adjusted survival curves as estimated by the “best” multivariate model; the impact of pretreatment risk factors (age >50 years, involvement of an additional vascular territory) is emphasised.
Functional outcome and prognostic factors
Mean (SD) follow up of the surviving patients (n = 130) was 34.5 (35.3) weeks (median, 26 weeks; range 8 to 188). The median GOS score at discharge and at three, six, and 12 months was 3 at each time. At the last follow up the GOS had improved in 40.9% of the patients and was unchanged in 59.1%. A long term GOS score of 2 was found in three patients (1.6%), 3 in 90 (47.9%), 4 in 34 (18.1%), and 5 in three (1.6%) (median GOS: 3)—that is, favourable results were achieved in 19.7% of all patients (37 of 188). The only variable associated with an unfavourable outcome was increasing age (continuously scaled, p<0.0002; dichotomised >50 years, p<0.0003). Twenty two of 63 patients ⩽50 years of age (34.9%) had a favourable outcome (GOS >3), as compared with 15 of 125 patients (12.0%) in the elderly subpopulation. Institution of treatment did not have prognostic relevance (figs 3 and 4).
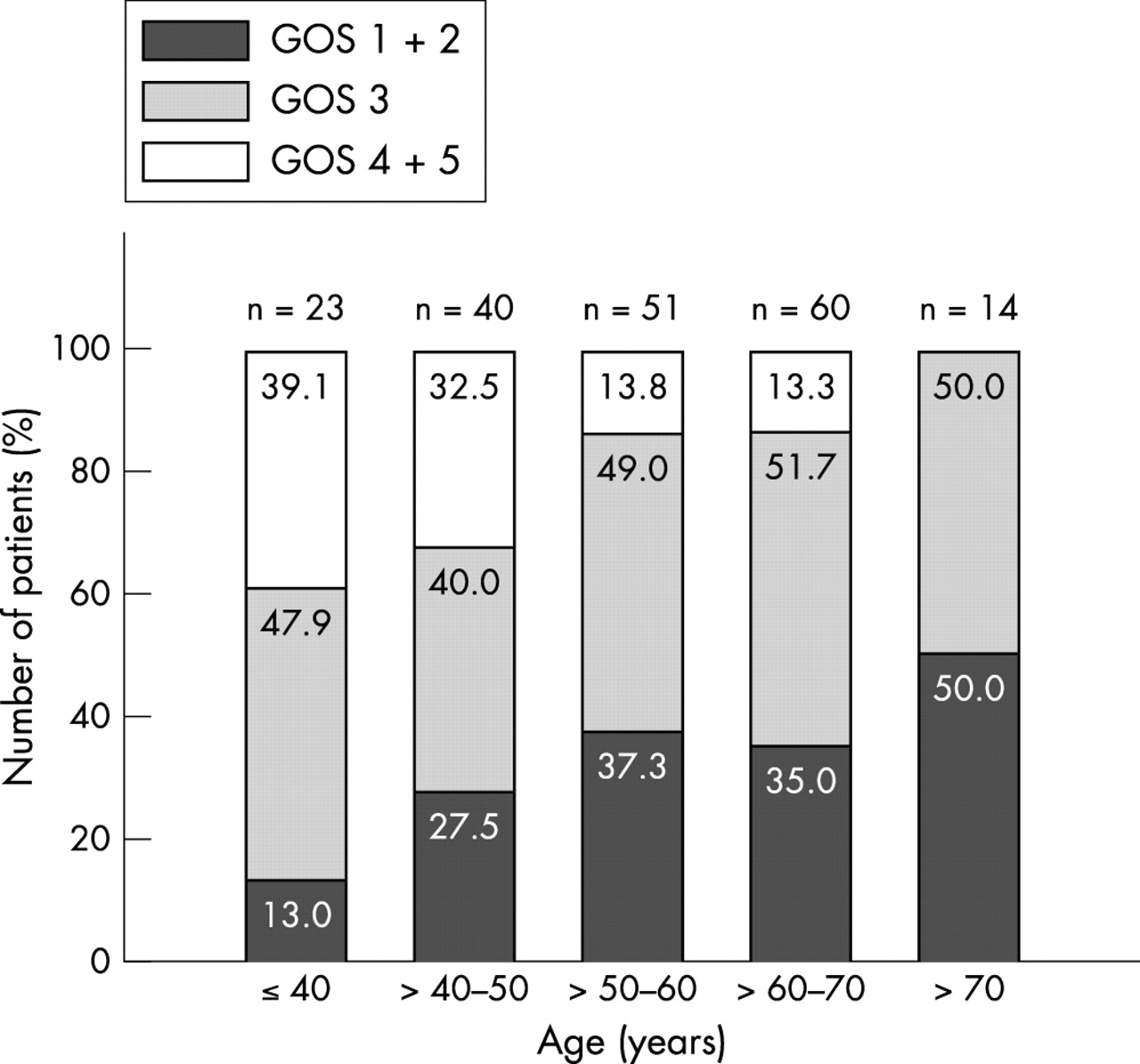
Functional outcome of 188 patients after decompressive craniectomy for malignant middle cerebral artery infarction. The powerful influence of age is demonstrated. GOS, Glasgow outcome scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Functional outcome of 188 patients after decompressive craniectomy for malignant middle cerebral artery infarction. Age is dichotomised (⩽50 years and >50 years). GOS, Glasgow outcome scale.
The Barthel index was available in addition to the GOS in 95 patients at the time of the last follow up. Median follow up in these patients was 26 weeks (mean (SD), 39.4 (37.7) weeks), with a mean Barthel index of 52.8 (28.0) points. Considering a Barthel index of >70 points to be a good outcome, 24.2% of the patients (n = 23) made a good recovery, as compared with 75.8% (n = 72) with an unfavourable outcome (Barthel index ⩽70).
DISCUSSION
The management of patients with space occupying MCA infarction remains a challenge. Small and heterogeneously composed study groups, inadequately defined selection criteria, the absence of long term follow up evaluation, and ongoing uncertainties over the influence of treatment-independent prognostic factors hamper subgroup evaluation and the comparative analysis of various treatment strategies.3–15 Our aim in the current pooled data analysis was not only to calculate mortality rates and functional outcome scores over time for a large number of patients; we also set out to investigate whether there were prognostic factors independent of treatment that could predict survival and functional outcome after decompressive hemicraniectomy for malignant MCA infarction (which was used as second line treatment). Conservative management and the indications for, timing of, and technique of surgical treatment were comparable in all the study centres, and institution related factors did not have prognostic impact in any of the models created. Thus the results obtained should not have been biased by institution related factors, and provide a standard against which other management strategies for similar subpopulations can be measured.
Survival and prognostic factors
The risk of death remains substantial beyond 30 days after decompressive surgery (because of non-neurological complications), and this has not yet been fully acknowledged. Accordingly, reported mortality rates should be interpreted with due consideration to the follow up time. In the current series the overall three, six, and 12 month mortality rates were 7.9%, 37.6%, and 43.8%, respectively. The estimated three month mortality was in the upper range of that previously reported.3,10,14,15 In particular, Schwab et al, who have undertaken so called “early surgery” in 31 patients, did not observe better results (three month mortality, 16%).4
The remarkable finding of the current study was that pretreatment variables have a profound impact on survival, even in this homogeneously treated highly selected patient population with space occupying infarcts in the MCA territory. Unfavourable predictors were older age (>50 years) and the involvement of more than one vascular territory, which divided the overall group into subsets with estimated six month mortality rates from as low as 20% to as high as 60%. The pretreatment clinical score was of minor prognostic importance. Though patients undergoing early decompressive surgery because of rapid clinical deterioration had a worse prognosis in the one variable model, the prognostic impact of this covariate (rapid clinical deterioration) was lost after multivariate analysis. Taking into account that the protagonists of early surgical treatment did not adjust outcome data for the effects of pretreatment prognostic factors and did not carry out a proper control group investigation,4 no definite conclusions can be drawn at present as to the optimal timing of surgical treatment.
Functional outcome and prognostic factors
In accordance with preliminary published data, 19.7% of all patients experienced a favourable functional outcome score (GOS score >3), with 1.6% achieving complete independence.3,10 The GOS score was significantly influenced by the patient’s age. Whereas only 12.0% of patients older than 50 years had a favourable outcome, this was the case in 34.9% of the younger patient subpopulation. Pretreatment clinical scores, involvement of two or more vascular territories, and laterality of the infarction did not have prognostic relevance. The latter is in line with the results of Schwab et al,4 and should be regarded with caution. A selection bias in favour of right sided infarction (right/left ratio in this series, 125/63) could not be excluded, as there might have been a tendency for physicians to deny surgery to patients with left sided strokes. Additional prospective data, appropriate outcome scores, and quality of life data are necessary for further clarification of this ongoing debate.
Limitations of the study and future perspectives
The different estimates of survival rates and functional outcome scores for prognostic subgroups of this series should be regarded cautiously. Model selection was based on a retrospective dataset and did not consider all aspects of the disease. In particular, the possible impact of CT/MRI related variables was not tested (which was explained by the large number of missing values in image related variables in the pooled dataset). Notwithstanding these limitations, the powerful prognostic impact of age was demonstrated for the first time with regard to both survival and functional outcome. There is continued uncertainty, however, about the overall effectiveness of surgical treatment and whether the risk factors identified for poor outcome are associated with hemicraniectomy or just with large MCA strokes, independent of how they are treated. Evaluation of a corresponding medically managed patient cohort appears essential in this situation for further clarification. Taking into account the high mortality, the poor functional outcome scores, and the high frequency of side effects of treatment in the elderly subpopulation, the effectiveness of decompressive surgery remains questionable in this subpopulation. Otherwise outcome data for the younger patients were encouraging. It remains a controversial issue whether future prospective randomised trials should focus on the overall effects of surgical v non-surgical treatment concepts in patients with large MCA strokes, or whether risk cohorts should be studied separately. The relatively favourable results after surgical treatment of younger patients (as demonstrated in this series) and the lack of corresponding data after non-surgical management strategies in previous reports (for comparative analysis) may raise the question of whether a prospective randomised study should include the younger patient subpopulation.
Conclusions
The current analysis shows that patients undergoing decompressive craniectomy for malignant cerebral infarction represent a rather heterogeneous population with a varying prognosis. Age must be considered the most important pretreatment prognostic factor, and surgical treatment results in younger patients are encouraging. Whether surgery should be done early or delayed remains unknown. The benefit of surgery for patients over 50 years of age is questionable and should be analysed in a prospective randomised study.
REFERENCES
Footnotes
-
See Editorial Commentary, p 179
-
Competing interests: none declared