Article Text

Abstract
Background: Delirium is a neuropsychiatric disorder characterised by severe cognitive impairment, but the specific neuropsychological profile of this condition has not yet been clearly delineated. Psychiatric symptoms of perceptual disturbance—such as hallucinations, illusions and misperceptions—are common in delirium, suggesting that patients may have deficits in the cognitive systems underlying visual perception.
Methods: Five neuropsychological tests of visual perception were administered to 17 older patients with delirium, as well as to two control groups comprising 14 patients with Alzheimer’s dementia and 18 cognitively normal patients. The Mini Mental State Examination and the Consortium to Establish a Registry for Alzheimer's Disease verbal memory test were also administered to assess the specificity of any perceptual impairments.
Results: Patients with delirium scored significantly lower than cognitively normal patients on all perceptual tasks and significantly lower than patients with dementia on three of these tasks. Mini Mental State Examination scores did not differ between the delirium and dementia groups, and patients with delirium showed significantly better verbal recognition performance than those with dementia.
Conclusions: Patients with delirium have specific visual perceptual deficits that cannot be accounted for by general cognitive impairment. These novel findings provide insights into the neural mechanisms underling delirium and might help to improve clinical detection and management of the disorder. The results also support previous suggestions that cognitive perceptual deficits play a causal role in eliciting psychiatric symptoms of perceptual disturbance.
Statistics from Altmetric.com
Delirium (or ‘acute confusional state’) is a severe neuropsychiatric disorder that is particularly prevalent in older, hospitalised patients.1 The core diagnostic features of delirium are an acute onset and fluctuating deficits in attention and consciousness,2 although several other cognitive and psychiatric symptoms are also associated with the disorder.3 The psychopathology of delirium remains remarkably under-studied.4 In particular, although marked cognitive impairment is known to occur,5–10 detailed characterisation of the neuropsychological profile of delirium is lacking. Increasing our understanding of the particular cognitive domains that are affected in patients with delirium may provide important insights into the underlying pathophysiological mechanisms of this disorder.
One area of cognition that has not yet been examined in delirium is visual perception. This oversight is surprising given that neuropsychiatric symptoms of perceptual disturbance—such as hallucinations, illusions and misperceptions—occur frequently in patients with delirium.3 Most of the knowledge about the content and nature of the perceptual disturbances associated with delirium has come from subjective patient reports and clinical observations.11 No published studies have yet been carried out to assess whether patients with delirium also have specific cognitive deficits of visual perception.
Evidence that psychiatric perceptual disturbances may be associated with cognitive deficits of visual perception has come from other patients who frequently experience hallucinations, such as those with dementia with Lewy bodies12 or Parkinson’s disease dementia (PDD).13 Such patients perform poorly on a range of cognitive tests of visual perception compared with patients with Alzheimer’s dementia (AD) who are matched in terms of overall cognitive impairment but do not experience visual hallucinations.14–17 Furthermore, in various types of dementia, the frequency of hallucinations shows strong positive correlation with the severity of the visual perceptual and attentional impairments and yet does not correlate with the degree of their overall cognitive impairments.18
To account for these patterns, Collerton et al. proposed that disturbed attentional processes and impoverished visual input might cause these hallucinations.18 In their Perception and Attention Deficit (PAD) model, Collerton and colleagues propose that in patients with both perceptual and attentional deficits, sensory inputs activate incorrect and irrelevant neural representations of objects in long-term memory. The patient experiences this erroneous cortical activity as hallucinations or illusory misperceptions.
Given that patients with delirium are known to show gross impairments of attentional functioning3 5 and a high frequency of psychiatric perceptual disturbances,3 19 the PAD model would predict that such patients also have cognitive deficits of visual perception. However this hypothesis has not been formally tested. In this study, we measured the integrity of cognitive visual perceptual processing in patients with delirium by using standard neuropsychological tests. The performance of these patients was compared with that of control groups of patients with AD or with no cognitive impairment. Additional tests of memory function and general cognitive impairment were also administered to all patients in order to ensure that any observed deficits of perceptual function in the patients with delirium could not be better accounted for by their degree of overall cognitive impairment.
METHODS
Participants
Sixty-two hospital patients provided written informed consent to take part in the study, which was approved by the Scotland A Research Ethics Committee. Patients were divided into three groups: (1) patients with current delirium and no known dementia, (2) patients with AD and no current delirium, and (3) cognitively normal (control) patients with no known dementia and no current delirium. Given that both delirium and AD are associated with older age, only patients aged over 70 years were approached to take part in the study. An exclusion criterion for all patients was visual or auditory impairments severe enough to affect the reliability of the cognitive testing.
Patients with delirium were recruited from acute medical and surgical wards of a general hospital. Potential participants were first identified by ward staff, who named eligible patients who had shown evidence of an acute change in cognitive function since being admitted. The presence of delirium was then formally assessed by one of the trained researchers (SM or LM) using the Confusion Assessment Method.20 This diagnostic algorithm records the presence of the four core symptoms of delirium: (1) acute onset or fluctuating course, (2) inattention, (3) disorganised thinking and (4) an altered level of consciousness. A diagnosis of delirium requires that symptoms 1 and 2 and either 3 or 4 are present.
The Confusion Assessment Method criteria were assessed using a validated battery of measures.21 This evaluation comprised the Mini Mental State Examination (MMSE)22 and attentional assessments that required the patient to repeat strings of numbers in a forward or reverse order and to list the days of the week and the months of the year backwards. The Delirium Symptom Interview23 was also administered to most patients. Patients’ medical notes and dialogue with hospital staff provided additional diagnostic information. Five patients were subsequently excluded from the delirium group for showing insufficient symptomatic evidence to meet the full diagnostic criteria for delirium. It is possible that these patients did have delirium but that their symptoms were too subtle to be detected at the time of examination. Alternatively, the clinical symptoms typical of delirium that were observed in these patients might have been attributable to subsyndromal delirium and/or another type of cognitive impairment. One of these five patients also had a visual impairment that may have affected the validity of the perceptual tasks. One further patient was excluded for showing evidence of having had pre-existing dementia, resulting in a final study group of 17 patients with delirium.
Patients with dementia were recruited from a hospital outpatient memory clinic. All dementia patients had been diagnosed by a geriatrician (JMS) as having either AD or mixed AD and vascular dementia according to the criteria of the International Statistical Classification of Diseases and Related Health Problems (10th revision).24 None of the 14 patients recruited into this group was subsequently excluded from the study.
Cognitively normal patients were recruited from the same hospital wards as the patients with delirium. Patients were included if they had no evidence of dementia or delirium, as judged by delirium assessments, their medical history, and their scores on the MMSE (using a cut-off score of 24 out of 30). Seven patients were excluded from this group for not meeting these criteria. The final number of participants in this group was 18.
Procedure
The presence of delirium was first assessed in all participants by using the assessment battery described previously. A second researcher (LM or SM) then administered the cognitive tests, using the same fixed order for each participant.
Visual perception was tested using five tests taken from the Visual Object and Space Perception battery.25 Space perception was measured using the dot counting and position discrimination tasks. In the dot counting task, participants are shown arrays of between five and nine randomly positioned black dots and report how many dots they see each time. In the position discrimination task, participants are shown two squares that each contain one black dot. The participant determines which of the two dots is positioned exactly in the centre of its square. Shape and object perception was tested using the shape detection, incomplete letters and object decision tasks. In the shape detection task, participants determine whether each of 20 random speckled backgrounds contains a superimposed speckled X figure. In the incomplete letters task, participants identify 20 capital letters, each of whose image has been degraded by randomly blanking out 70% of its surface. In the object decision task, participants are shown four silhouette images, one of which is a real object and three are nonsense shapes, and determine which image is of the real object. Participants are not required to name the objects. Previous research has shown that patients with AD are generally unimpaired on all of these tasks.14 15 26
In order to evaluate the specificity of any perceptual deficits in the delirium group, verbal word memory was also assessed in each participant by using the Consortium to Establish a Registry for Alzheimer's Disease word learning test.27 In this test, participants are first shown 10 printed words, one at a time, and are asked to read each word aloud as it is presented. Immediate recall of the words is then tested by asking the participant to recite as many of the 10 words as they can. This procedure is repeated twice more, and the correctly recalled words in each of the three trials are summed to give a total immediate recall score out of 30. Delayed recall of the same words is then tested approximately 5–10 minutes later by again asking the participant to recall as many of the words as possible. This delayed recall score is expressed as a percentage of the participant’s highest score of the three immediate recall trials. Delayed recognition is tested by sequentially showing the participant the 10 target words intermixed with 10 new words and asking them to report whether or not each word is from the original set. Performance on this task is measured by subtracting the number of false positive responses made by the patient from the number of words they correctly recognised to give a ‘recognition discrimination index’. This value can, therefore, range from −10 to 10, with higher scores being indicative of more accurate recognition.
All cognitive and delirium assessments were carried out in outpatient clinic rooms with the dementia patients and on inpatient wards with the delirium and cognitively normal patients. The testing environment of the dementia patients was, therefore, likely to have contained fewer distractions than that of the delirium and control groups. However, as none of the perceptual tasks involved rapid stimulus presentations or required speeded responses, this difference in testing environment is unlikely to have affected the validity of the results. Furthermore, task instructions were repeated and prompts to respond were given whenever necessary during the testing sessions, thereby further minimising the effects of any external distractors.
Statistical analyses
Given that the distributions of most of the cognitive test data were non-normal and that variances were not always homogeneous between groups, non-parametric tests were used to compare cognitive data between groups. First, Kruskal–Wallis tests were used to look for overall differences between the three groups. Mann–Whitney U tests were then used to perform pairwise group comparisons. Statistical significance was taken as a two-sided p value of less than 0.05.
RESULTS
Patient characteristics
Demographic details of the participants in each group are shown in Table 1. The cognitively normal patients were significantly younger than both the delirium patients (t(33) = 2.35, p<0.05) and the dementia patients (t(30) = 2.62, p<0.05). On the other hand, there was no significant difference in age between the delirium and dementia groups (t(29) = 0.08, p = 0.94). The median MMSE score of the cognitively normal patients was higher than that of both the patients with delirium (U = 3.0, p<0.001) and the patients with dementia (U = 15.0, p<0.001). The median MMSE scores of the delirium and dementia patients, however, did not differ significantly (U = 99.5, p = 0.44). Patients with delirium and those with dementia were, therefore, similar in terms of age and overall level of cognitive impairment.
Visual perception
One patient in the delirium group was unable to complete the object decision task. All other perceptual tasks were completed by all participants.
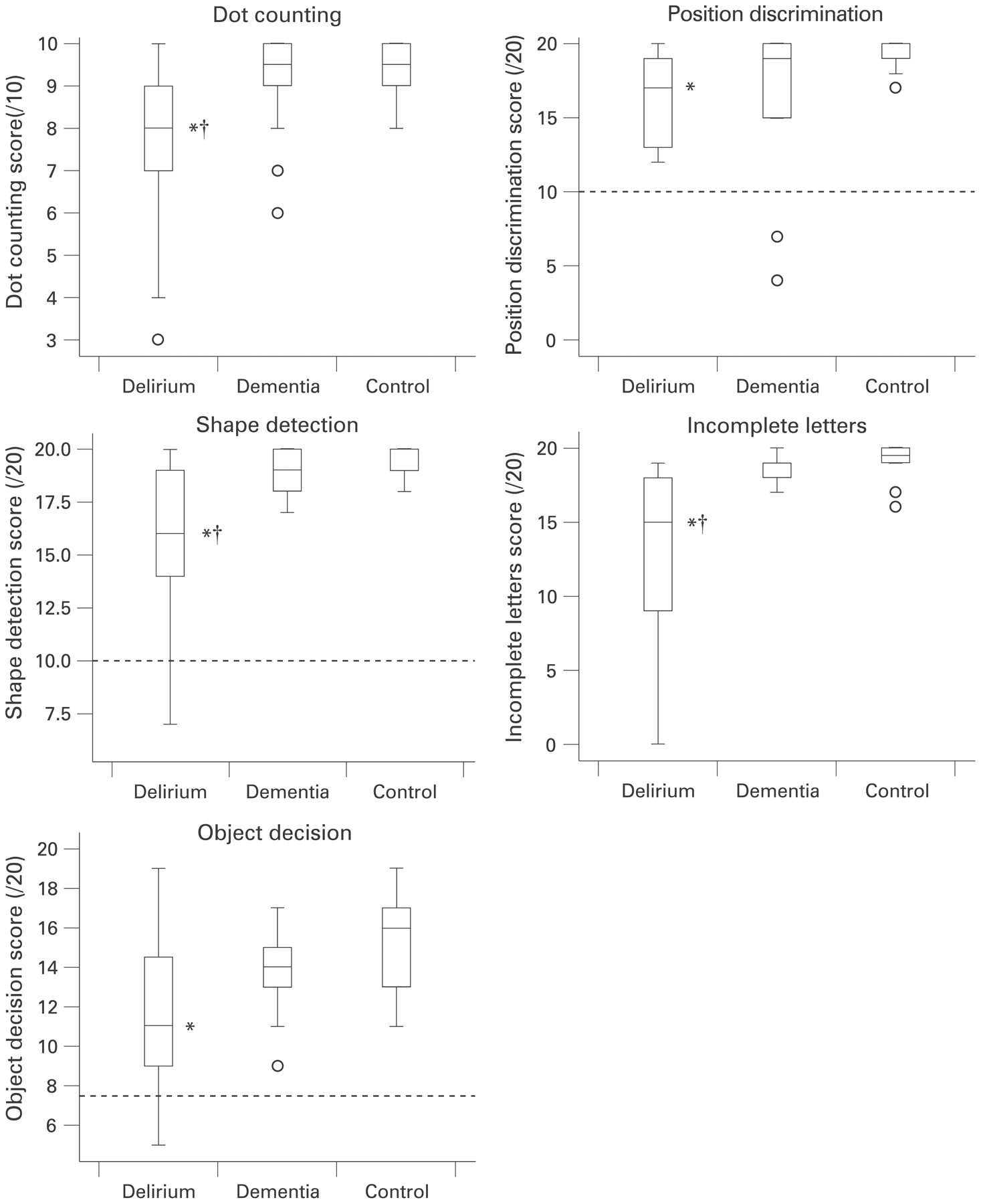
Cognitively normal patients generally scored well in all the visual perceptual tasks (fig 1). At least 50% of these patients scored at, or close to, ceiling level in all tasks except for object decision. Even in this more difficult task, all cognitively normal patients scored above chance level. These patterns of results are consistent with published norms for the tests.25 The performance of the delirium and dementia groups was more variable (fig 1). Even so, very few patients in these groups scored at floor level or at below chance level in any of the tasks, showing that the difficulty level of the tasks was appropriate for the participants. Kruskal–Wallis tests revealed that differences between the three groups on all these tests (dot counting: H = 12.32 (2 degrees of freedom (df)), p<0.01; position discrimination: H = 8.43 (2 df), p<0.05; shape detection: H = 15.72 (2 df), p<0.001; incomplete letters: H = 19.94 (2 df), p<0.001; object decision H = 8.50 (2 df), p<0.05).

Group results for each of the visual perceptual tasks. The interquartile range and median value of each dataset are represented by the height of the inner box and the position of the central horizontal line, respectively. The positions of the upper and lower bars of each plot indicate the maximum and minimum non-outlier values of each dataset. Any outliers are represented by open circles on the plot. The position discrimination, object decision and shape detection tasks were all 2-alternative or 4-alternative forced choice response tasks. Chance-level performance for each of these tasks is indicated on the plots with a dashed horizontal line. Symbols to the right of the median lines indicate group scores that differ significantly from cognitively healthy control patients (*) and patients with dementia (†).
Patients with delirium scored the lowest on all tests of visual perception; their performance was significantly worse than that of cognitively normal patients on all five of these tests (dot counting: median difference = 2.0, U = 56.0, p<0.01; position discrimination: median difference = 3.0, U = 66.0, p<0.01; shape detection: median difference = 4.0, U = 45.5, p<0.001; incomplete letters: median difference = 4.5, U = 34.5, p<0.001; object decision: median difference = 5.0, U = 65.5, p<0.01). Patients with delirium also scored significantly lower than patients with dementia on the dot counting test (median difference = 1.5, U = 68.5, p<0.05), the shape detection task (median difference = 3.0, U = 53.5, p<0.01), and the incomplete letters test (median difference = 4.0, U = 35.0, p<0.001). Their performance did not differ significantly from that of the patients with dementia in the position discrimination test (median difference = 2.0, U = 90.0, p = 0.26) or the object decision task (median difference = 3.0, U = 74.5, p = 0.12). The results of patients with dementia did not differ from those of cognitively normal patients on any of these tasks (dot counting: median difference = 0.5, U = 95.5, p = 0.25; position discrimination: median difference = 2.0, U = 92.0, p = 0.21; shape detection: median difference = 1.0, U = 87.0, p = 0.15; incomplete letters: median difference = 0.5, U = 91.0, p = 0.19; object decision: median difference = 2.0, U = 84.5, p = 0.12).
Memory
There were differences between the study groups in all three measures of memory performance (immediate recall: H = 26.69 (2 df), p<0.001; delayed recall: H = 25.80 (2 df), p<0.001; delayed recognition: H = 21.57 (2 df), p<0.001). Patients with dementia had the lowest scores on all three of these measures (fig 2): their scores on all three measures were significantly lower than those of cognitively normal patients (immediate recall: median difference = 9.5, U = 12.5, p<0.001; delayed recall: median difference = 85.7%, U = 9.0, p<0.001; delayed recognition: median difference = 5.5, U = 14.5, p<0.001). Patients with delirium also scored lower than cognitively normal patients on all three measures of memory (immediate recall: median difference = 6.5, U = 19.0, p<0.001; delayed recall: median difference = 52.4%, U = 43.0, p<0.001; delayed recognition: median difference = 3.5, U = 60.5, p<0.01). The immediate recall scores of the delirium group, however, did not differ significantly from those of the dementia group (median difference = 3.0, U = 102.0, p = 0.52). Patients with delirium also performed better than patients with dementia on the delayed recognition task (median difference = 2.0, U = 67.5, p<0.05), and the results of the delayed recall task showed a trend towards better performance by the patients with delirium (median difference = 33.3%, U = 73.0, p = 0.07).

{kind=link}
{kind=link}
Group results for the immediate recall, delayed recall and delayed recognition measures of the verbal memory tasks. Symbols to the right of the median lines indicate group scores that differ significantly from cognitively healthy control patients (*) and patients with dementia (†). CERAD, Consortium to Establish a Registry for Alzheimer's Disease.
DISCUSSION
The main novel finding in this study is that patients with delirium have impaired visual perception relative to patients with dementia and cognitively normal patients. Importantly, we found that patients with delirium showed a similar level of overall cognitive impairment and better memory performance than patients with dementia, suggesting that the impaired visual perception in patients with delirium is not due to generalised cognitive impairment. These results provide evidence that patients with delirium have specific cognitive deficits of visual perception and contribute to our understanding of the neuropsychological profile of the disorder. These findings parallel those of previous studies that patients who have dementia with Lewy bodies and those with PDD have similar perceptual deficits.14–18 In addition, our results are consistent with the suggestion that cognitive visual perceptual deficits are associated with psychiatric symptoms of perceptual disturbance.
The poor performance of the delirium group on the perceptual tasks suggests that patients with delirium have cognitive deficits in visual perceptual processing. It is not clear, however, which elements of the perceptual system are affected. It may be that delirium is associated with direct impairment of basic visual processes undertaken in the occipital cortex, such as the determination of line orientation or spatial frequency analysis.28 Alternatively, the perceptual deficits could result from impairments in the attentional systems responsible for directing processing resources to visual inputs. Attentional systems in the parietal lobe modulate neural activity in many areas of the occipital cortex that are involved in visual perceptual processing.29 30 Under normal conditions, this relationship increases the sensitivity of perceptual judgements at attended locations.31 Attentional impairments in delirium, however, may result in less-effective directing or focusing of attention to appropriate aspects of visual stimuli during perception, thereby compromising the accuracy of perceptual judgements. Future studies that compare the extent of perceptual processing deficits by using a wider range of visual and non-visual perceptual tasks may be able to uncover the functional mechanisms underlying the errors in patients with delirium.
The results of this study parallel previously published data showing cognitive perceptual deficits in patients who experience psychiatric perceptual disturbances similar to those seen in delirium.14–18 Our findings are also consistent with the PAD model of hallucinations,18 which suggests that disturbed attentional processes and impoverished visual inputs both play a causal role in eliciting hallucinations. In this study, neither the frequency of the patients’ hallucinations nor the magnitude of their attentional impairments was measured, and so it was not possible to determine the association of either of these variables with the measured perceptual deficits. Nevertheless, given that patients with delirium are already known to show attentional impairments,3 5 this new finding of cognitive visual perceptual deficits in delirium is consistent with the causal explanation of the PAD model. Further research is now needed to examine whether independent relationships can be found between the magnitude of cognitive perceptual and attentional deficits and the severity of psychiatric perceptual disturbances.
The findings of this study also have useful implications for the detection and clinical management of patients with delirium. Diagnosing delirium can be difficult due to its considerable symptom overlap with other disorders commonly seen in the elderly population, such as the dementias. The majority of the cognitively normal patients performed without difficulty all but one of the perceptual tasks administered in this study. In addition, patients with AD showed consistently better performance than patients with delirium in some of these tasks, most notably the shape detection and incomplete letters tasks. Incorporating items from these tests into diagnostic tools for delirium may, therefore, be useful in detecting delirium and in discriminating it from other disorders, thus enabling the rapid identification and treatment of patients with delirium. This new evidence for visual perceptual problems in delirium may also help improve clinical care. For instance, the format of visual information given to patients with delirium could be made simpler and clearer or even presented in a different sensory modality, so that patients are less likely to make perceptual errors and thus misunderstand the information.
In summary, these findings suggest that patients with delirium have specific cognitive deficits of visual perception that are not present in patients with AD. These results provide new information on the neuropsychology of delirium and have implications for the assessment and management of this common, serious and poorly understood disorder.
Acknowledgments
This work was funded by a Medical Research Council Clinician Scientist Fellowship to AMJM. The work was undertaken by The University of Edinburgh Centre for Cognitive Ageing and Cognitive Epidemiology, part of the cross council Lifelong Health and Wellbeing Initiative. Funding from the Biotechnology and Biological Sciences Research Council, the Engineering and Physical Sciences Research Council, the Economic and Social Research Council and the Medical Research Council is gratefully acknowledged. We thank the patients and staff of the geriatric medicine and orthopaedics units of the Royal Infirmary of Edinburgh and those at the memory clinic in the Royal Victoria Hospital, Edinburgh.
REFERENCES
Footnotes
Competing interests: None.