Article Text

Abstract
Background The clinical diagnosis of dementia with Lewy bodies (DLB) is made on the basis of consensus criteria; however, the sensitivity of the criteria is relatively low. There are no generally accepted biomarkers to distinguish DLB from other dementias. Here the utility of quantification of α-synuclein, β-amyloid42 (Aβ42) and tau in the CSF of patients with DLB, Alzheimer's disease (AD) and other dementias was examined.
Methods 86 patients were divided into three age and sex matched groups: DLB (n=34), AD (n=31) and other dementias (n=21). Two patients with α-synuclein gene (SNCA) duplication were also examined. Aβ and tau were quantified using an ELISA kit. A modified sandwich ELISA was developed which enables the sensitive quantification of CSF α-synuclein.
Results Total and phosphorylated tau levels as well as Aβ40/42 and tau/Aβ42 ratios were significantly higher in AD patients than in patients with DLB (p<0.01) and other dementias (p<0.01). CSF α-synuclein levels in DLB patients were significantly lower than those in patients with AD (p<0.05) and other dementias (p<0.01). CSF α-synuclein level correlated with the Aβ42 level in DLB patients (p=0.01, r=0.43). Two patients with SNCA duplication exhibited relatively low levels of CSF α-synuclein.
Conclusions The study suggests that reduced levels of CSF α-synuclein in DLB may reflect the accumulation of α-synuclein with Lewy pathology in the brain and that quantification of CSF α-synuclein helps in the differentiation of DLB from AD and other dementias in combination with Aβ42 and tau analysis.
Statistics from Altmetric.com
Introduction
Dementia with Lewy bodies (DLB) is clinically characterised by fluctuating cognitive decline, visual hallucinations, delusions and parkinsonism. A key pathological feature of DLB is the accumulation of α-synuclein, a major filamentous component of Lewy bodies and neurites. DLB is considered to be the second most common form of neurodegenerative dementia after Alzheimer's disease (AD).1 Consensus criteria for the clinical diagnosis of DLB were proposed2; however, the problem in diagnosis is the relatively low sensitivity of the criteria despite the high specificity.1 3 There is considerable overlap of clinical manifestations as well as neuropathology between DLB and AD patients, which could lead to an inaccurate antemortem diagnosis.3
Diagnostic biomarkers in CSF have been explored to determine the aetiology of dementia in patients. The decrease in amyloid-β (Aβ) 42 level and increases in total and phosphorylated tau levels in the CSF of AD patients have been widely demonstrated.4 Several research groups attempted to quantify CSF α-synuclein as a possible biomarker of neurodegenerative disorders; however, contradictory results were reported. Low levels of CSF α-synuclein were reported in patients with Parkinson's disease (PD) and DLB.5 6 In contrast, Öhfelt et al reported that α-synuclein levels in PD and DLB patients are comparable with those in controls.7
Here we attempted to establish the utility of quantification of α-synuclein in CSF by a modified sandwich ELISA in combination with quantifications of Aβ42 and tau for differentiating patients with DLB from those with AD and other dementias.
Methods
Participants
A total of 86 patients divided into three age and sex matched groups (DLB (n=34), AD (n=31) and other dementias (n=21)) were recruited from Niigata University Hospital and affiliated hospitals. Patient characteristics and demographics are shown in table 1. Patients were diagnosed as having DLB and AD when they fulfilled the ‘probable’ diagnostic consensus criteria for these dementias.2 8 Each subject in this study underwent neurological examination, neuroimaging (CT and/or MRI) and laboratory tests to exclude alternative causes of their cognitive impairment. All patients with DLB had progressive dementia, concomitant parkinsonism, visual hallucinations or fluctuating cognition. Two patients with the DLB/PD dementia (PDD) phenotype and α-synuclein gene (SNCA) duplication were also included.9 AD patients with any parkinsonian feature or visual hallucination were not included. The group of other dementias consisted of 21 patients with frontotemporal lobar degeneration (n=12), progressive supranuclear palsy (n=2), normal pressure hydrocephalus (n=2), vascular dementia (n=2) and unclassified dementia (n=3). This study was approved by the ethics committee of Niigata University.
Clinical characteristics of the patients and levels of CSF markers
CSF collection and assay
CSF was collected by lumbar puncture after informed consent was obtained. Samples of CSF were centrifuged at 4000 g for 10 min and the supernatant was immediately frozen in polypropylene tubes and stored at −80°C until assay. Aβ40 and Aβ42 levels were determined using an ELISA kit (Wako, Japan). Total tau and phosphorylated tau (ptau181) were quantified using a commercially available enzyme immunoassay kit (Innogenetics, Belgium).
We developed a modified sandwich ELISA to quantify α-synuclein in CSF. ELISA was performed using a monoclonal Syn-1 antibody (BD Bioscience, California, USA) as the capturing antibody and a polyclonal FL-140 antibody (Santa Cruz Biotechnology, California, USA) as the reporter antibody. This assay enables the direct measurement of α-synuclein using neat CSF samples (100 μl). The standard curve for the ELISA was constructed using recombinant human α-synuclein. All the samples were analysed in duplicate.
Statistical analysis
All statistical analyses were performed using commercially available software, SPSS 12.0J (SPSS Japan, Japan). Results are shown as mean±SD. Comparisons between groups were performed using analysis of variance (ANOVA), followed by Tukey's post hoc test. An exploratory correlation was examined using Pearson correlation coefficient. Receiver operating characteristic curve (ROC) analysis was used to determine the best cut-off values for the measured biomarkers.
Results
Quantification of Aβ42 and tau in CSF
Table 1 shows the clinical characteristics and results of CSF biomarkers in patients with DLB, AD and other dementias. There was no statistically significant difference in age at examination, age at onset or gender among the three groups. We quantified tau, Aβ40 and Aβ42 in the CSF of the patients (table 1). The total and phosphorylated tau levels in AD patients were significantly higher than those in patients with DLB (p<0.01) and other dementias (p<0.01). In addition, the Aβ42 level in the AD patients was significantly lower than that in patients with other dementias (p<0.01). Patients with DLB showed a higher Aβ42 level than AD patients and a lower Aβ42 level than patients with other dementias; however, the differences were not statistically significant. The Aβ40/42 and tau/Aβ42 ratios were significantly higher in patients with AD than in patients with DLB (p<0.01) and other dementias (p<0.01).
Optimising sandwich ELISA for α-synuclein quantification in CSF
We attempted to optimise sandwich ELISA to achieve a high sensitivity quantification of CSF α-synuclein. We found that the use of the combination of the Syn-1 and FL140 antibodies yielded the highest sensitivity. This ELISA system enables the detection of only α-synuclein without cross reactivity to human β- and γ-synucleins (see supplementary figure 1A available online). Immunoprecipitation assay using the combination of FL-140 and Syn-1 antibodies detected a single band migrating at ∼17 kDa corresponding to full length α-synuclein in CSF (see supplementary figure 1B available online). We therefore chose to utilise the ELISA system to quantify the CSF α-synuclein.
Quantification of CSF α-synuclein and its correlation with clinical variables
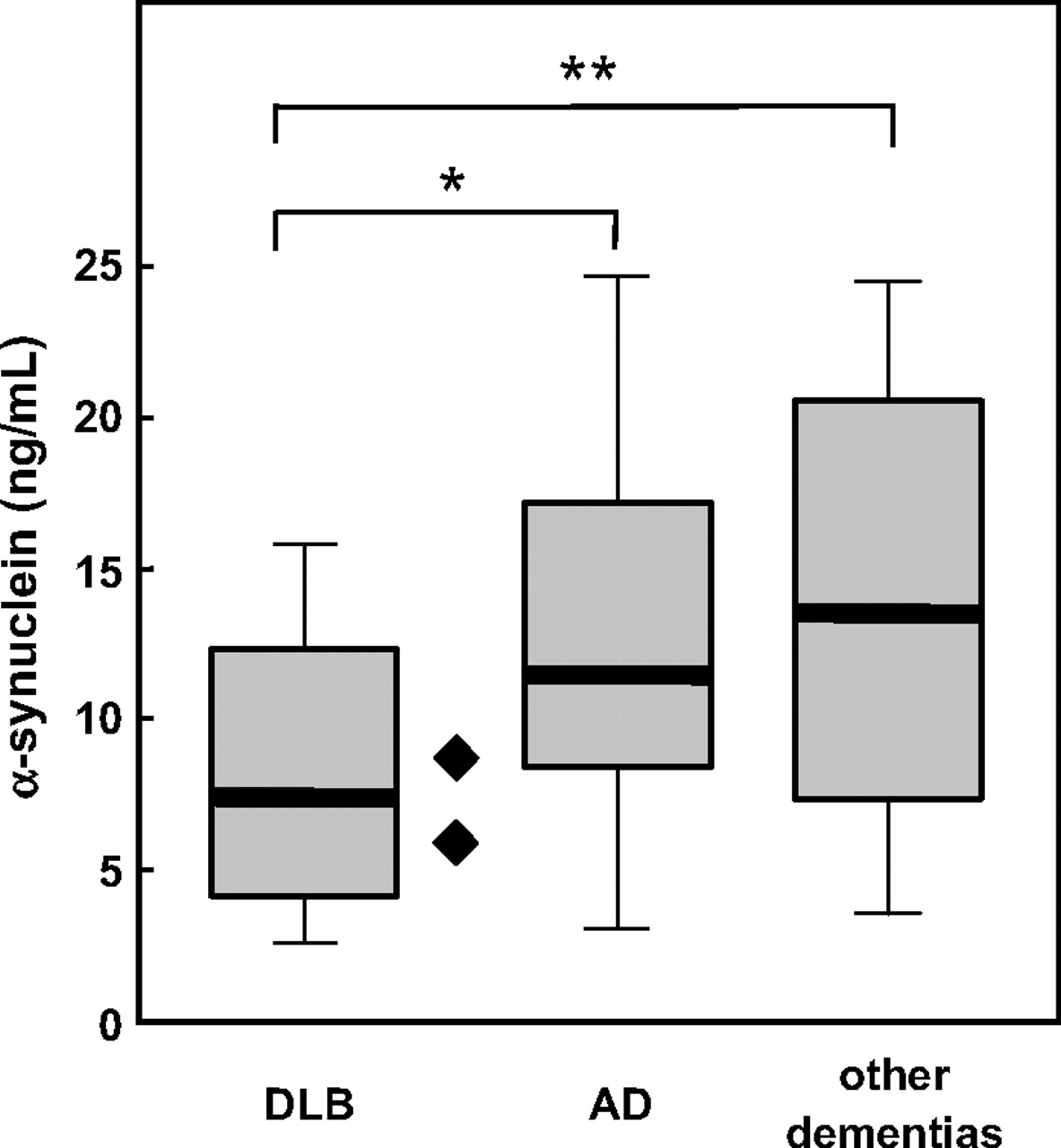
The results of the quantification of α-synuclein in the DLB, AD and other dementia groups are shown in figure 1. The CSF α-synuclein level in DLB patients was 8.2±4.2 ng/ml which was significantly lower than that in AD patients (12.2±5.8; p<0.05) and patients with other dementias (13.9±7.5; p<0.01). We also examined the CSF of two patients with SNCA duplication and the DLB/PDD phenotype.9 The α-synuclein levels were 5.2 ng/ml (examined at the age of 74 years) and 9.7 ng/ml (examined at the age of 54 years), which are comparable with those of DLB patients and lower than the average values in patients with AD and other dementias.

{kind=link}
Box plots of CSF α-synuclein (ng/ml) in the patient groups dementia with Lewy bodies (DLB (n=34), Alzheimer's disease (AD) (n=31) and other dementias (n=21). Two patients with SNCA duplication are indicated (filled diamonds). The box plots show the median values (thick lines), and the 25th and 75th percentiles. Statistically significant difference was calculated using ANOVA, followed by Tukey's post hoc test. *p<0.05, **p<0.01.
We found no significant association of CSF α-synuclein level with MMSE score, sex, age at examination or duration of the disease in the DLB or AD group. In the DLB group, the CSF α-synuclein level correlated with the Aβ42 level (p=0.01) (see supplementary figure 2A available online). This correlation was not found in the AD group (see supplementary figure 2B available online).
Receiver operating characteristic analysis
The sensitivity and specificity of the CSF biomarkers, including α-synuclein, tau and Aβ42, were determined by receiver operating characteristic (ROC) analysis (see supplementary table available online). Results of ROC analyses of CSF α-synuclein levels in the DLB and AD groups showed a sensitivity of 72.4% and a specificity of 61.8% at a cut-off value of 9.0, and those in the DLB group and the group with other dementias showed a sensitivity of 66.7% and a specificity of 73.5% at a cut-off value of 11.6. Total and phosphorylated tau levels and tau/Aβ42 ratio differentiated the AD group from the DLB group and the group with other dementias, with sensitivities and specificities in the range 86–95%.
Discussion
Measurement of CSF proteins, particularly those deposited in the affected brain, is becoming an important diagnostic tool in the differential diagnosis of neurodegenerative dementia. In this study, we demonstrated that CSF α-synuclein levels in DLB patients were lower than those in patients with AD and other dementias. This finding seems to support the hypothesis that low α-synuclein levels reflect neuropathological processes implicated in α-synuclein pathology, such as Lewy bodies and neurites in DLB. We also showed that levels of total and phosphorylated tau as well as Aβ40/42 and tau/Aβ42 ratios in AD patients were different from those in patients with DLB and other dementias. Taken together, quantification of α-synuclein in combination with Aβ42 and tau in CSF would be useful in differentiating DLB from AD and other dementias.
Studies on the quantification of CSF α-synuclein by ELISA showed contradictory results. Our results are in agreement with an earlier study showing lower CSF α-synuclein levels in DLB patients than in AD patients, although a relatively small number of AD patients (n=13) was examined.6 In contrast, other studies showed no significant difference in CSF α-synuclein level between DLB and AD patients.7 10 11 These conflicting results might be explained by heterogeneous inclusion criteria of patients, methodological difference in α-synuclein quantification, or both. For instance, we used the combination of Syn-1 and FL-140 antibodies for our modified sandwich ELISA whereas other groups used different antibodies such as monoclonal 211, Syn3d, Syn5d or polyclonal mSA-2 antibody.5–7 11
The question regarding the reduced level of CSF α-synuclein in DLB patients remains unanswered. Our finding that CSF α-synuclein level is decreased in DLB patients may have parallels with the evidence of a reduced CSF Aβ42 level in AD patients.12 Our finding that α-synuclein level correlated with Aβ42 level in CSF might be related to the pathological finding that Aβ deposition is associated with extensive α-synuclein lesions and a high level of insoluble α-synuclein in the brain of DLB patients.13
We previously reported on DLB/PDD patients who carry SNCA duplication.9 14 In the brain of patients with SNCA duplication, Lewy bodies are abundantly distributed throughout.14 Overexpression of SNCA appears to be relevant to the development of α-synuclein pathology in the brain because patients with SCNA multiplication have high SNCA mRNA expression levels.15 Unexpectedly, our study revealed that patients with SNCA duplication showed relatively low levels of CSF α-synuclein. This result suggests that the increased expression level of SNCA does not simply lead to an increased CSF α-synuclein level, and that CSF α-synuclein level likely reflects the abnormal accumulation of α-synuclein in the brain.
Although our study has potential clinical implications, it also has several limitations. Firstly, the diagnosis of patients was based on clinical criteria, not on autopsy verification. An important question is whether alteration of CSF α-synuclein level relates to the pathological change of α-synuclein accumulation in the brain. Secondly, we were unable to examine healthy subjects because such samples were not available. Lastly, most of the DLB patients received medication such as L-dopa and dopamine agonists which may affect the CSF α-synuclein level. Despite these limitations, our study finding warrants further study in which CSF α-synuclein levels are determined in additional patient groups with synucleinopathies, including Parkinson's disease and multiple system atrophy.
Acknowledgments
The authors wish to thank the participants for their cooperation.
References
Supplementary materials
Web Only Data jnnp.2009.197483
Files in this Data Supplement:
Footnotes
Linked articles 206391.
Funding This study was supported by a Grant-in-Aid for Scientific Research (21200041) from the MEXT, Japan and the Mochida Memorial Foundation for Medical and Pharmaceutical Research.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the ethics committee of Niigata University School of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary