Article Text

Abstract
Objectives Visual-field deficits following temporal lobe surgery have been reported in the literature. In this prospective study, the authors analyse their experience of visual-field deficits in 105 consecutive cases undergoing temporal-lobe surgery performed by a single surgeon, with particular consideration to the laterality of the deficit and its functional implications.
Methods 105 consecutive patients undergoing an anterior temporal lobe resection for epilepsy, between March 1998 and June 2004, were selected. The patient population had a mean age of 35 years (range 19–60 years); 53 had a left-sided resection and 52 a right-sided resection. 91 patients had mesial temporal sclerosis, three gangliogliomas, four dysembryoplastic neuroepithelial tumours (DNETs), two neurocytomas and two cavernomas, and in three cases the histology was inconclusive. Pre- and postoperative visual-field tests were obtained using the Humphrey Esterman binocular functional test for all cases. The test was set to stimulus white III, with a single intensity of 10 DB on the background of 31.5 ASB for all patients. A minimum follow-up period of 12 months postsurgery was employed. Postoperative MRI scans were carried out on all patients. 60 scans were randomly selected, and the extent of temporal lobe resection calculated manually for each.
Results Of the 105 cases, 16 patients had a visual-field deficit postoperatively which was not present preoperatively: 12 following a left and four following a right-sided resection. The OR for incurring a postoperative visual-field defect following left versus right-sided surgery was 3.51 (95% CI 1.05 to 11.73, p=0.04). In four patients, the deficit was severe enough to preclude them from driving in the UK (three left- and one right-sided resection). There was no association between the extent of tissue resection and the incidence of postoperative visual-field deficits.
Conclusions This study suggests left-/right-hemispherical asymmetry in the Geniculocalcarine tracts with field deficits being 3.5 times more likely following left-sided anterior temporal lobe resections compared with right-sided resections. This has significant implications on counselling patients for these procedures. MR tractography may provide an anatomical substrate for these clinical findings, perhaps revealing a more anterior course of the optic radiations within the temporal lobe in one hemisphere versus the other.
- Temporal lobe surgery
- Meyer's loop
- visual-field deficits
- hemispherical asymmetry
- anatomy
- epilepsy, surgery
- vision
Statistics from Altmetric.com
- Temporal lobe surgery
- Meyer's loop
- visual-field deficits
- hemispherical asymmetry
- anatomy
- epilepsy, surgery
- vision
Introduction
Visual-field deficits (VFDs) as a complication of temporal lobe surgery are a well-documented entity, with numerous publications over the decades reporting varying degrees of field deficits occurring in 50–100% of such cases1–15 (see table 1). The deficits are believed to be due to disruption of the proposed pathways of the optic radiations in the temporal lobes, the anterior portion of which is termed the Meyer loop.
Recent literature comparing the incidence of visual-field deficits following temporal lobe resection for epilepsy and the methodology used
It is well established that there is considerable intersubject variability in the anatomy of the Meyer–Flechsig loop.1 16 17 Compounded with different surgical approaches, employing varying degrees of neocortical resection and variations in the methods whereby visual fields are assessed has resulted in a wide discrepancy in the quoted incidence of this complication.
In this report, we carried out a prospective study of 105 patients in our epilepsy programme undergoing an anterior temporal lobe resection between 1998 and 2004. Postoperative visual fields were compared with the preoperative studies and new deficits highlighted. These were correlated with the resection size on postoperative imaging. The incidence and functional implications of the VFDs in our series are presented, and we highlight, for the first time, hemispherical asymmetry with respect to the incidence of postoperative VFDs following temporal lobectomy for epilepsy.
Methods
A prospective study was designed to assess the incidence and functional implications of postoperative VFDs in patients undergoing temporal lobe surgery for epilepsy. The seizure outcome in this population is also documented.
One hundred and five consecutive cases undergoing surgery between March 1998 and June 2004 were selected. The mean age of patients was 35 years (range 19–60 years). Fifty-three had a left-sided resection and 52 a right-sided resection. Ninety-one patients had mesial temporal sclerosis and 14 other lesions which were composed of three gangliogliomas, four DNETs, two neurocytomas and two cavernomas, and in three the neuropathology was inconclusive. All the operations were carried out by a single right-handed surgeon (WH) employing the technique advocated by Spencer.18 The resection is performed in two stages: the lateral neocortical resection is stereotyped with the variation in resection size being primarily along the mesial structures. In all cases, the temporal horn of the lateral ventricle is entered from below at the apex of the collateral sulcus, rather than perpendicular through the middle temporal gyrus. Subpial dissection is used for resection of the superior temporal gyrus, and about 4 cm of the neocortical is resected measured from the temporal tip. The uncus is cleared with the CUSA and the hippocampus dissected out and sent for histology, the length variable on a case-by-case basis. No fixed retraction is used. For the 14 lesional cases, the pathology was all incorporated within the standard resection.
Pre- and postoperative visual-field tests were obtained using the Esterman binocular protocol functional test for all cases carried out on a Humphrey visual field analyser model 611 (Allergan:California). The test was set to stimulus white III, with a single intensity of 10 dB on the background of 31.5 ASB for all patients. The test was chosen because of its use by the UK Driver and Vehicle Licensing Authority in assessing fitness to drive. All the field analyses were carried out by one experienced operator (MG) and reviewed by a neuro-ophthalmologist (GTP). If there was a concern regarding the accuracy of the fields assessed the test was carried out again on up to three different occasions and the best one employed. This is in line with the UK Driving and Vehicle Licensing Agency (DVLA) recommendations.19 In cases with a single point loss in the relevant quadrant, the testing was repeated, and if reproduced, this was categorised as a field deficit for the purposes of this study. A patient's ability to drive was assessed in accordance with the criteria set out by the DVLA.19
The mean time interval between the preop assessment and surgery was 6.4 months, ranging from 3 days to 47 months. The mean time interval between surgery and the postop assessment was 5.4 months, ranging from 1 month to 54 months. Seizure status was assessed at 12 months postoperatively, according to the Engel classification.20
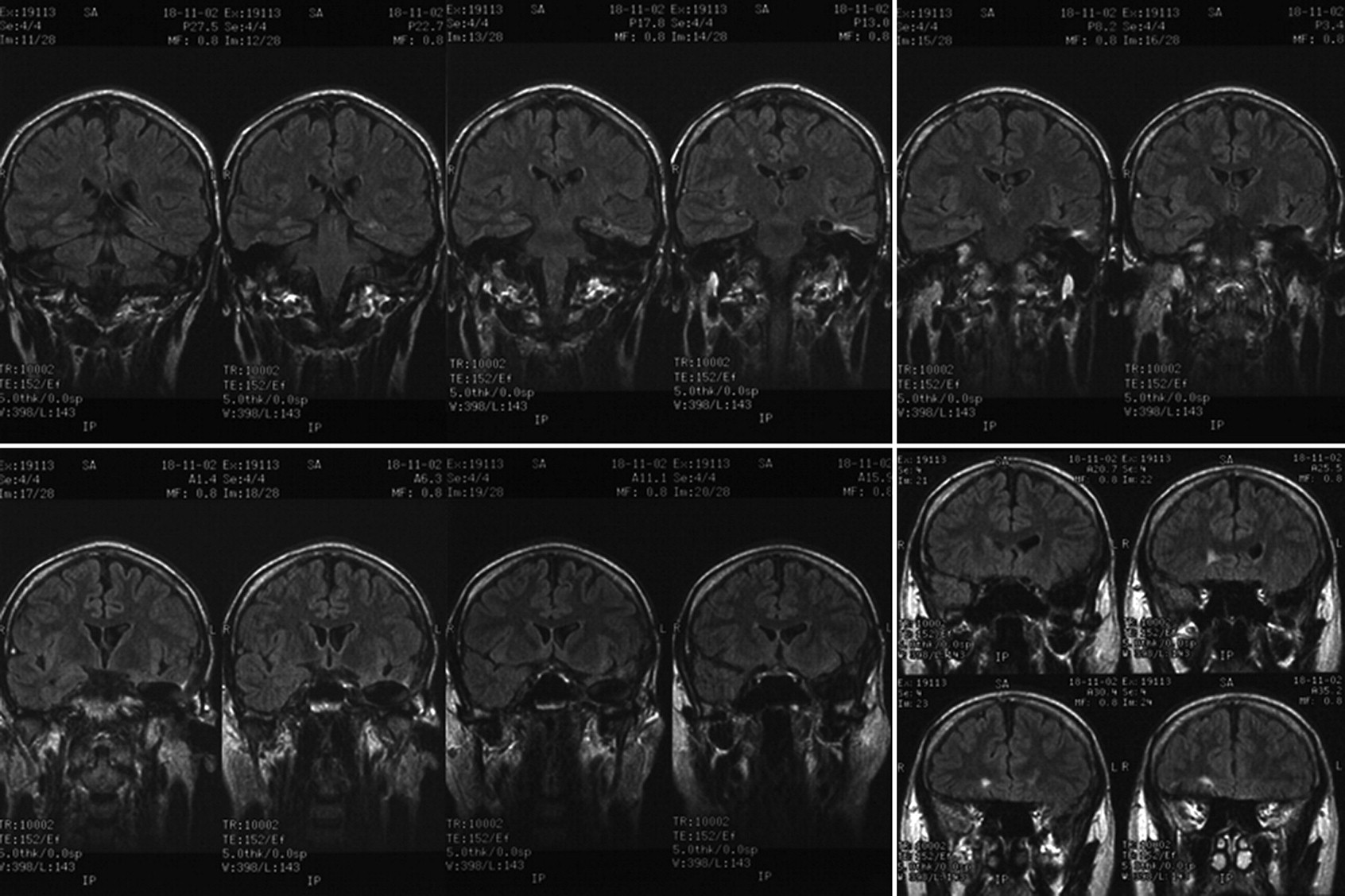
Postoperative MRI scans were obtained on all patients. Of these, the first 60 scans with a diagnosis of hippocampal sclerosis retrieved randomly from the imaging archives were chosen for quantitative statistical analysis. This sample was checked for a chronological bias. There were equal numbers of left- and right-sided resections. The particular acquisitions used were the volumetric Fast spoiled gradient (FSPGR) IR prepped (slice thickness 1.5 mm) acquired in the coronal plane and the fluid attenuated inversion recovery (slice thickness 5 mm) also obtained in the coronal plane (figure 1). The mesial posterior resection limit was categorised utilising its relation to the adjacent pons: as far as the anterior surface of the adjacent pons (four cases), just behind the frontal pons (13 cases), at the midpoint of the pons (12 cases) or up to the posterior margin of the pons (32 cases). In this location, the position of the lateral geniculate body was noted. This method of quantifying resection size offered the best reproducibility and accounted for interpatient variability in terms of head size. Most if not all of the amygdala was excised in these cases with a small residual noted in 20 of the 60 scans analysed. There was also a variable amount of signal change in the brain surrounding the resection. This was interpreted as mechanical damage with gliosis. Its extent was recorded qualitatively as absent (five cases), mild (20 cases), moderate (20 cases) or severe (15 cases). For statistical analysis, the data were recoded in a binomial manner contrasting absent/mild changes with moderate/severe changes.

Postoperative volumetric fast spoiled gradient (case 73) IR prepped (slice thickness 1.5 mm) coronal MRI images used to calculate the extent of resection. In this case the mesial resection was taken as far back as the posterior border of the pons. Most of the amygdala has been excised as well. The signal change at the resection margins was classified as mild.
Statistical analysis
Univariate logistic regression models were used to explore the relationship between postoperative VFDs (dependent variable) and certain key predictor variables that were hypothesised to have an influence on the incidence of such deficits following temporal-lobe surgery for epilepsy. These variables included the side of resection, the presence and severity of postoperative signal change in the vicinity of the resection (as defined above), and the extent of resection in the randomly selected subset of 60 patients with hippocampal sclerosis. Multiple univariate models were constructed in order to assess if there was any relationship between the occurrence of postoperative VFDs and the posterior limit of the hippocampal resection (to the anterior, middle or posterior surfaces of the pons) and whether or not the amygdala was taken. In this exploratory analysis, p<0.05 was used to declare statistical significance. All analyses were undertaken using Stata version 10.0 for Mac (StataCorp, College Station, Texas).
Results
Of the 105 cases, 16 patients (15.3%) had a visual-field deficit postoperatively (figure 2B): 12 following a left temporal lobectomy and four following a right-sided resection (figure 3). While there was no statistical difference between the extent of mesial resection between the left- and right-sided cases (p=0.4), there was a significant association between the laterality of the temporal lobe resection and the odds of manifesting a postoperative VFD (OR 3.51, 95% CI 1.05 to 11.73, p=0.04 for a deficit following a left-sided temporal lobe resection). Preoperatively, a peripheral field loss was present in one patient who was undergoing treatment with Vigabatrin. This remained unchanged after the operation, and she was included in the study. In four patients (3.8%) (figure 4), the deficit was severe enough to preclude them from driving in the UK19 (three left and one right-sided resection). The VFD did not extend to the lower quadrants in any patient.

(A) Preoperative and (B) postoperative visual fields in a patient (case 39) with a characteristic partial upper quadrantinopia ‘ pie in the sky’ defect following a left temporal lobectomy. This patient was able to retain their driving licence.

Bar graph comparing the incidence of visual-field deficits (VFDs) in our patient population segregated by pathology. MTS, mesial temporal sclerosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A, B) Pre- and postoperative visual fields in case 22, in whom the visual-field deficits precluded them from driving based on the Driving and Vehicle Licensing Agency guidelines.
There was no association between the extent of the mesial resection and the incidence of VFDs in this population of patients. We analysed the signal change at the resection margins, and again this was not associated with the incidence of VFDs.
Seventy-eight patients (74.3%) achieved seizure freedom (Engle 1) at 12 months' follow-up. There was no association between the incidence of VFD and seizure outcome in our series. Three of the four patients with VFDs severe enough to preclude them from driving continued to have seizures, resulting in one patient being prevented from driving solely due to their postoperative visual loss.
Analysing the 91 (86.7%) mesial temporal sclerosis cases separately, 67 (73.6%) achieved seizure freedom. Fourteen patients (23.1%) had VFDs, and three (3.3%) were unable to drive. The finding that VFDs were approximately 3.5 times as common in left- versus right-sided resections remained robust (OR=3.52, 95% CI 1.01 to 12.21, p=0.05).
Discussion
Numerous studies (including one from our unit)10 have previously analysed the anatomy of the optic radiations and the functional implications of damage to these during temporal lobe surgery.1 2 4–9 11–17 21 These studies have aimed to identify the anatomy of the optic radiations including the anterior extent of the Meyer loop within the temporal lobe, the relationship of the optic radiation to the temporal horn of the lateral ventricle, the degree of intersubject variability and any relationship between the size of surgical resection or different surgical techniques and the incidence of field deficits (see table 1). The results of these studies have not always been consistent. Potential sources of bias have been a relatively small sample size, retrospective reviews, interobserver and intersurgical variability, and different criteria being used for defining visual-field deficits. In this study, the authors attempted to rectify these biases by designing and conducting a prospective study. A follow-up from our original study, published in 2000,10 our aim here was to collate data on over 100 consecutive patients and perform preoperative visual fields on these patients to ensure that any deficits identified postoperative were temporally related to the surgery. A single surgeon employed the same surgical technique in all the cases, and the same operator carried out all pre- and postoperative visual-field analyses. The Humphrey Esterman binocular functional test was employed, as this is the standard used by the UK DVLA and offers better interobserver reproducibility. In addition to intraoperative measurements, postoperative imaging was obtained in all cases, and resection size was calculated for a random subset. With these measures, we attempted to identify factors that may predispose to the development of postoperative VFDs following a temporal-lobe resection in our study population.
The literature poses considerable variation in the anterior limit of the Meyer loop within the temporal lobe and its implications for postoperative visual-field deficits in temporal lobe surgery. Table 1 lists the recent literature on this subject to highlight the variation in the methodology and the resultant variation in the quoted incidence. In 1954, Penfield stated that a resection within the anterior 60 mm of the temporal tip would not produce a VFD.13 Over the years, this ‘safe zone’ has progressively been getting smaller. Falconer4 put the limit at 40 mm and Bjork2 and his group to a value between 30 and 40 mm. In 1968, Marino and Rasmussen stated that defects occurred at resection sizes down to 40 mm. These studies utilised intraoperative estimation of resection lengths. More recent studies have analysed postoperative MRI to estimate resection sizes and have highlighted significant intersubject variability. Krolak et al,9 using automatic static perimetry and postoperative MRI analyses, put the anteriormost point of the Meyer loop between 20 and 30 mm. Nilsson et al12 compartmentalised the temporal lobe on postoperative MRI and, correlating this with VFDs, concluded that VFDs were present in certain cases when the superior temporal gyrus was involved between 18 and 36 mm from the temporal pole. Another study carried out pathological dissections and put the mean value at 27 mm (SD 3.5) with emphasis on intersubject variability.21 Barton et al1 correlated postoperative MRI findings with VFDs and, employing regression analyses, put the anterior limit at 24 mm for the nasal field and 28 mm for the temporal-field deficits. However, as mentioned, direct comparisons between these studies are problematic, as different methodologies have been employed.
In our study, a maximal resection size of 45 mm was employed in all patients and resulted in a 15.3% incidence of VFDs. This data concurs with the recent literature, suggesting the Meyers loop may be anterior to the 45mm threshold from the temporal pole, in some cases. We, however, did not find any link between the size of resection and the incidence of VFDs. As stated, on postoperative MRI analyses, the resections within the neocortex were stereotyped, ranging between 40 and 45 mm, with variation solely being in the volume of mesial structures resected. As the Meyer loop is a white matter structure, it is not surprising that a correlation between the extent of mesial resection and damage to it was not identified.
A VFD incidence of 15.3% is low compared with earlier series,1 3 6 8–10 12 14 17 including those employing similar assessments of postoperative visual deficits and of resection size. In addition to the above, the other manoeuvres that we feel may be responsible for this finding are the approach used to enter the temporal horn from below and the absence of any fixed retraction, which cannot be proven with the current study design.
Tractography is likely to play a significant role in further elucidating the anatomic substrate for the findings demonstrated in this study. A recent study from our unit22 correlated a postoperative VFD with a disruption of the optic tract on DTI analyses. Nilsson16 analysed the optic tracts in seven healthy volunteers and two patients, and confirmed the wide intersubject variability. More recently, Taoka17 and his group used presurgical tractography in 14 patients undergoing temporal-lobe resection for epilepsy. Their findings are interesting, as they found an association between the incidence of the VFD and the size of disruption of the Meyer loop but not one between the incidence of VFDs and the size of resection from the temporal tip. This study further highlights the difficulties in obtaining postoperative tractography using current paradigms. Though validation of diffusion tensor tractography remains a work in progress, this technique does offers great promise in this field. Further studies are awaited.
Notwithstanding the variance in the reported incidence of VFDs in this patient population, a more pertinent question remains: what is the functional significance of this for any given patient? Egan et al3 documented a VFD incidence of over 80% in their study population but concluded that all of these deficits were asymptomatic. Ability to drive is one of the main reasons put forward by patients choosing to undergo temporal-lobe surgery for epilepsy, and this serves as an objective criterion to answer the above question, at least in the UK. In our series, out of the 16 cases with a VFD following surgery, in four cases (3.8%) the deficit was severe enough to preclude them from obtaining a driving licence in the UK. This figure is considerably less than the 25% incidence quoted in our previous paper10 also using the Humphrey Analyser Esterman protocol, which analyse data between 1986 and 1995 or the 50% incidence quoted by another UK study analysing 14 patients.23 The reduction in incidence of symptomatic VFDs is most likely to be due to the surgical technique as described and the cumulative case load of our epilepsy service. The UK DVLA criteria19 are among the most stringent internationally, and these patients may be able to drive in other countries. Though small, it is imperative that patients be advised about this potential risk before surgery.
The question of hemispherical asymmetry in the anatomy of the optic radiations has been raised previously. In one study from 1976, Jensen and colleagues7 found that larger field defects extending to the lower fields were more likely following a right-sided resection; this was attributed to the larger resections on that side. More recent studies have reported a larger resection size on the right side but with no difference in the incidence of VFD.1 6 14 It is arguable that a difference in the resection size but not VFDs in these studies alludes to a more anterior limit of the Meyer loop on the left side. In a recent study, Yeni and colleagues15 analysed 30 patients with mesial temporal sclerosis for VFDs following temporal lobe surgery. It is interesting to note that although 10 of the 21 patients (47.6%) with left-sided resections developed a VFD compared with just one of the nine patients (11.1%) with right-sided resection, the authors did not find the hemispherical asymmetry statistically significant.
In our series we found we found VFDs to be 3.5 times more likely following left sided resections. The strength of the present study was a large cohort of patients operated on by a single surgeon who carries out similar neocortical resections on both sides. As the subject of a follow-up study, we are currently employing diffusion tensor tractography to analyse this finding further. Why the Meyer's loop would be more anterior on the left side remains to be answered. One hypothesis proposed by the authors is that as the language areas in the left posterior temporal lobes expanded in humans the phylogenetically older optic radiation was pushed more anterior on that side.
Conclusion
Visual-field deficits occur following anterior temporal lobe resections even when the resection size is less than 45 mm. The incidence is low, and in most cases, these deficits do not carry any functional implications. In 4% of cases, the deficits were severe enough to preclude the patient from driving in the UK. Patients need to be adequately counselled for this possibility. We found significant hemispherical asymmetry in the anatomy of the optic radiations, with field deficits being 3.5 times more likely following a left-sided resection. This finding taken in conjunction with the greater functionality of the left lobe in most patients has led to the jocular remark ‘ When it comes to temporal lobectomies, do what is right and think about what is left.’ Further information may come from diffusion tensor imaging (tractography) studies performed prospectively pre- and postoperatively.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.