Article Text

Abstract
Objective Despite refined criteria for behavioural variant frontotemporal dementia (bvFTD), its differentiation from Alzheimer's dementia (AD) remains difficult at early clinical presentation. Apraxia is not considered as a supportive feature for the diagnosis of bvFTD, but for AD. However, only few studies have quantified praxis disturbances in mild disease stages and their specificity for AD compared with bvFTD remains indistinct. We explore apraxia in bvFTD and investigate the differential validity of apraxia screening tests to distinguish between AD, bvFTD and healthy controls (HC).
Methods We compared composite apraxia scores assessed with standardised neuropsychological screening tests as well as performance in praxis subdomains in patients who fulfil current clinical criteria for AD (N=20), bvFTD (N=20), and in HC (N=20).
Results Composite scores of apraxia screening tests provided high diagnostic accuracy for detecting mild stages of both neurodegenerative disorders compared with HC (sensitivity: 75–95%; specificity: 70–90%). Both patient groups showed pronounced impairments in limb praxis, especially in imitation of hand and finger postures (bvFTD: 71.7%; AD: 55.5%; HC: 86.7%) and pantomime of object use (bvFTD: 88.6%; AD: 81.4%; HC: 97.5%). Beyond that, patients with bvFTD displayed a unique profile of deficits for imitating face postures (bvFTD: 69%; AD: 88%; HC: 95.5%).
Conclusions Praxis disturbances are important but under-represented diagnostic features in mild stages of AD and bvFTD. Apraxia screening tests are easily applicable diagnostic tools, which may support clinical diagnoses of both neurodegenerative diseases. The analysis of individual apraxia profiles can effectively facilitate differential diagnosis of AD and bvFTD.
- ALZHEIMER'S DISEASE
- APRAXIA
- NEUROPSYCHOLOGY
- DEMENTIA
- BEHAVIOURAL DISORDER
Statistics from Altmetric.com
Introduction
Apraxia refers to a disability to correctly perform or imitate movements on command despite widely intact elemental sensorimotor functions, intellectual abilities and comprehension.1 Definitions and taxonomies of apraxia and its subcomponents are diverse and competing cognitive models disagree in the definition of domains that essentially constitute the syndrome.2 ,3 However, dysfunctions in imitation and pantomime on command have been proposed as the core features of the syndrome.4 This descriptive division of praxis domains and subdomains (figure 1) has overcome a range of definitional and practical issues in apraxia research and has thus been adopted by modern apraxia screening tests for patients with stroke.2 ,3

Apraxia subcomponents. Division of domains and subcomponents of apraxia tested in this study corresponding to the distinctions made by Goldenberg, 2009.4 Please note that according to this taxonomy, apraxia can also affect actual use of objects and tools but that this domain is not investigated here. We use the term ‘pantomime of emblems’ instead of ‘emblematic gestures’ here in order to emphasise its commonality to ‘pantomime of object-use’.
Despite its reference as a supportive feature for the diagnosis of Alzheimer's dementia (AD) in international clinical guidelines,5 only few studies investigated apraxia in early disease stages.6 Apraxia in AD is assumed to result from atrophy of left parietal and/or temporal cortices.7 However, the strict dependency on parietal lobe function for praxis tasks has recently been challenged.4 Praxis subdomains have been linked to areas in the frontal lobes in healthy controls (HC)8 and accordingly in disorders characterised by frontal lobe dysfunctions such as primary progressive aphasia,9 corticobasal degeneration10 and schizophrenia.11 Yet, apraxia has not been evaluated in behavioural variant frontotemporal dementia (bvFTD), a neurodegenerative disease that is characterised by early and progressive atrophy of the medial frontal cortex.12 Alongside insidious changes in social conduct, patients with bvFTD display deficits in social perspective taking and mentalising abilities13 ,14 but also in planning and organisation of complex action due to frontal-executive dysfunction.15
We explored the incidence and nature of praxis disturbances in bvFTD. In particular, we were interested in the applicability and diagnostic accuracy of standardised and objective apraxia screening tests for the diagnosis of AD and bvFTD. Moreover, we investigated whether a detailed analysis of praxis subdomains may facilitate differential diagnoses between the two neurodegenerative disorders in mild disease stages.
Methods
Participants
Patients were recruited from the memory clinic at the Department of Neurology of the University Hospital Münster, Germany, between January and October 2013. Initial diagnoses were based on current clinical criteria for AD and bvFTD, respectively.16 ,17 Patients with AD presented with early progressive memory impairment, whereas patients with bvFTD showed early and proceeding deterioration in personality, behaviour and social conduct confirmed by follow-up examinations. Diagnoses were substantiated by a neurological examination including history taking, a detailed neuropsychological assessment, MRI of the brain at 3.0 Tesla, and—in case of bvFTD—an 18-fluorodeoxyglucose positron emission tomography (PET) when MRI was not fully informative or ambiguous on regional atrophy focus. Analysis of cerebrospinal fluid (CSF) biomarker profile, including τ-protein and amyloid-β peptide levels was included in the diagnostic workup. Patients suggestive of vascular dementia, psychiatric, malignant, infectious or inflammatory diseases as well as multifactorial aetiologies were excluded. Patients with clinically predominant aphasia, visual agnosia, depression or movement disorders (eg, Parkinsonism or alien-limb syndrome) were likewise excluded. HC consisted of relatives of patients. All control participants were screened for psychiatric disorders using a semistructured interview and had a comprehensive neurological examination before referral to the study. Patients with AD with a Mini-Mental State Examination (MMSE18) <19 and controls with an MMSE <28 were excluded. To quantify severity of behavioural disturbances, the frontal behavioural inventory (FBI19) was administered to caregivers of patients. Disease duration was estimated by relatives and verified by clinical records. A total of 104 patients were reviewed and tested for the aforementioned inclusion and exclusion criteria. After this procedure we arrived at the desired sample size of N=20 for the bvFTD and AD groups. Out of the 20 patients with bvFTD, 16 fulfilled all criteria for ‘probable bvFTD’.17 Four patients with bvFTD were considered ‘possible bvFTD’ due to less marked frontal and/or anterior temporal atrophy or a conflicting CSF biomarker profile at the time of inclusion despite an unambiguous clinical presentation.17 Within the AD group, all patients fulfilled the criteria for probable AD with varying levels of evidence of the AD pathophysiological process (please refer to online supplementary table S1 for biomarker profiles of all included patients). The study was approved by the local ethics committee (2012-365-f-S). All participants in this study gave written informed consent.
Apraxia assessment
We conducted three screening tests for apraxia during routine follow-up examinations within 6 months after initial diagnosis. The Cologne Apraxia Screening (CAS) and Ideomotor Apraxia Test (IAT) were administered in accordance with their published manuals.20 ,21 The CAS consists of a total of 20 items involving the praxis subdomains pantomime of object use (10 items), imitation of hand and finger postures (5 items) and imitation of face postures (5 items). The IAT incorporates only imitation of hand and finger postures (10 items) but unlike the CAS, it has already been validated in patients with AD. Both tests provide an objective, standardised quantitative scoring system based on time and accuracy for each performed gesture. Notably, inter-rater reliability is high for both tests (IAT: Cohen's κ=0.83−1; CAS: Spearman's r=0.91).20 ,21 To cover all subdomains of apraxia depicted in figure 1, we conducted a third screening test comprising items from routine clinical apraxia assessment: The Münster Apraxia Items (MI) consist of commonly used pantomimes of emblems (4 items) requested verbally (eg, ‘show me how to wave goodbye’) and imitation of hand and finger postures (8 items) depicted on photographs. A detailed description of items and the scoring system can be found in the appendix (see online supplementary figure S1). Scoring of all apraxia assessments was based on video analysis and carried out by an experienced clinical neuropsychologist (AJ). To test for inter-rater reliability of the MI, 15 videos were rated by a second rater blinded for the patient's diagnosis. We found a good concordance between ratings (mean Cohen's κ=0.77; range 0.61–1.0 depending on the item). Scores for praxis subdomains shown in figure 1 were calculated by summing up raw values of the respective items across all three apraxia screening tests. For comparisons between subjects and domains, praxis subdomain scores were then converted to percentage.
Statistics
Data analysis was carried out using SPSS V.21. Before analysis, data were screened for outliers by visual inspection of boxplots. However, no participants showed consistently abnormal results compared with their group mean across variables. MMSE scores were compared using a univariate analysis of variance (ANOVA) and post-hoc Games-Howell tests. Disease duration and scores on the FBI were contrasted between patient groups using independent sample Student's t-tests. We used a multivariate ANOVA (MANOVA) with Games-Howell post-hoc tests to compare apraxia composite scores and scores on apraxia subdomains across groups. To account for multiple post-hoc pairwise comparisons, Bonferroni correction procedure for the number of apraxia variables was applied—thus only p values <0.0056 were considered statistically significant. Receiver operating characteristic curves were computed to calculate sensitivity and specificity of the apraxia screening tests for each patient group compared with HC. To further explore differences between patient groups at the level of praxis subdomains, we conducted three follow-up mixed-design ANOVAs in order to directly investigate possible diagnosis x subdomain interaction effects.
Results
Demographic data and disease severity scores
Clinical and demographic characteristics of the participants are summarised in table 1. Age and education of the participants were compared using ANOVA and did not differ between patients with bvFTD and AD. There was a significantly higher percentage of women among patients with AD compared with patients with bvFTD, χ2 (2, N=20)=14.14, p<0.01. Both patient groups scored significantly lower on the MMSE compared with HC. Patients with AD presented with lower MMSE scores than patients with bvFTD (bvFTD: 25.4, AD: 22.4, p=0.009). Owing to its disproportionately high weighting of memory, verbal and visuoperceptual functions, the MMSE has been shown to be insensitive for the core behavioural and cognitive deficits in bvFTD especially in mild disease stages when apathy and mutism are less pronounced.22 ,23 Disease duration was longer for patients with bvFTD compared with patients with AD in our sample, t(32)=2.58, p<0.05. Behavioural disturbances as measured by the FBI were mild-to-moderate but expectedly more pronounced in bvFTD compared with patients with AD, t(32)=7.04, p<0.01.
Demographics, clinical characteristics and apraxia scores
Apraxia screening tests—composite scores and diagnostic properties
Table 1 summarises results and between-group comparisons of composite apraxia scores and scores of praxis subdomains. MANOVA revealed that composite apraxia scores and scores of subdomains differed significantly across groups, F(12, 104)=5.96, p<0.0001; Wilk's Λ=0.351, partial η2=0.41. Composite scores of the three conducted apraxia screenings are depicted separately for each group in figure 2A. Patients with AD and bvFTD scored significantly lower compared with HC in each of the three apraxia screening tests. However, using these composite scores, performance of patients with AD and bvFTD did not differ significantly (table 1). All three apraxia screening tests showed a high predictive validity for the differentiation between both AD versus HC (figure 2B; table 2) and bvFTD versus HC (figure 2C; table 2). Diagnostic properties of the three apraxia screening tests can be found in table 2. The CAS showed the greatest area under curve of the three apraxia tests for both comparisons (AD vs HC and bvFTD vs HC).
Diagnostic properties of apraxia screening tests
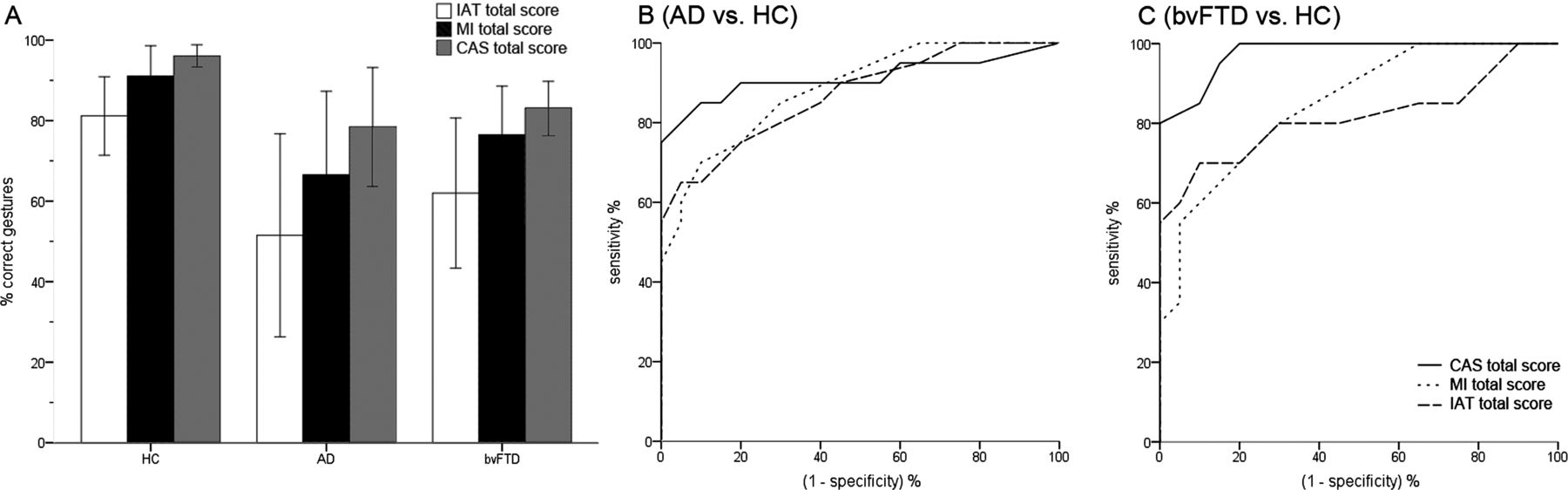
Diagnostic properties of apraxia composite scores. (A) Mean group performances on apraxia screening tests (composite scores). (B and C) ROC curves of the three apraxia screening tests for the comparisons AD versus HC and bvFTD versus HC (bvFTD, behavioural variant frontotemporal dementia; CAS, Cologne Apraxia Screening; HC, healthy controls; IAT, Ideomotor Apraxia Test; MI, Münster Apraxia Items; ROC, receiver operating characteristic).
Apraxia screening tests—subdomain scores and differential diagnosis
At the level of praxis subdomains, both patient groups showed significantly reduced scores compared with HC in pantomime of object use, imitation of hand and finger postures as well as in the superordinate domains pantomime (all) and imitation (all). However, patients with bvFTD and AD did not differ from each other on any of these scores in direct comparison. We found no significant between-group differences in pantomime of emblems. In contrast, patients with bvFTD uniquely revealed significantly diminished scores in the praxis subdomain imitation of face postures when compared with HC (Games-Howell p<0.000) but also in direct comparison to patients with AD (Games-Howell p=0.005; table 1; please refer to online supplementary video 1 for a sample video of a patient with bvFTD).
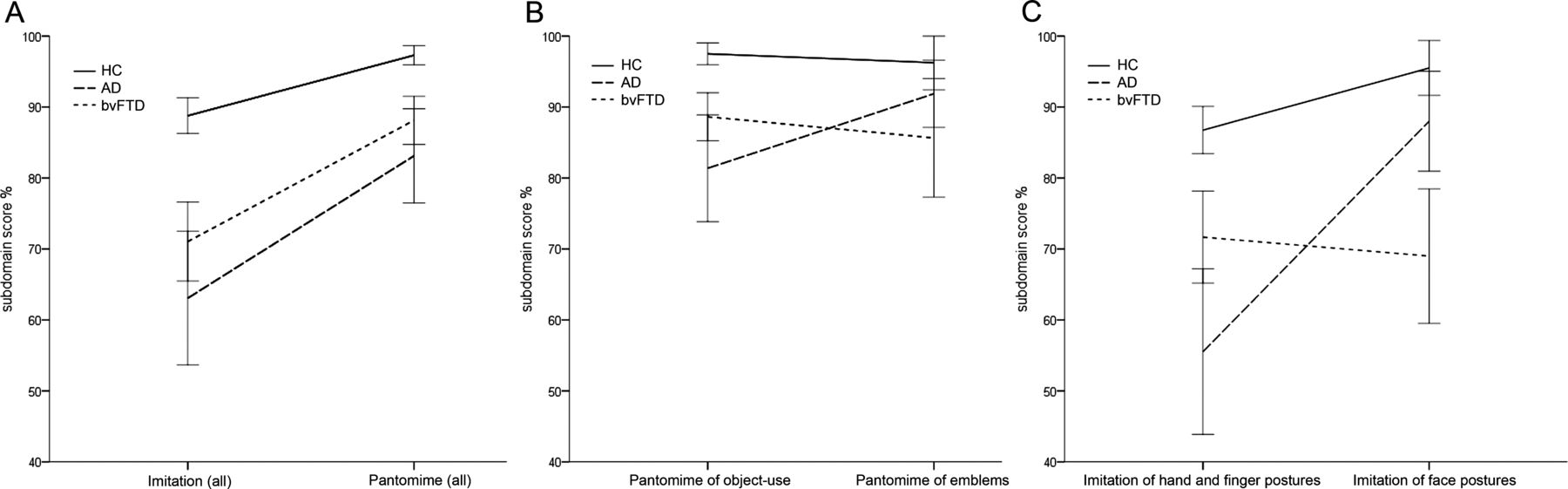
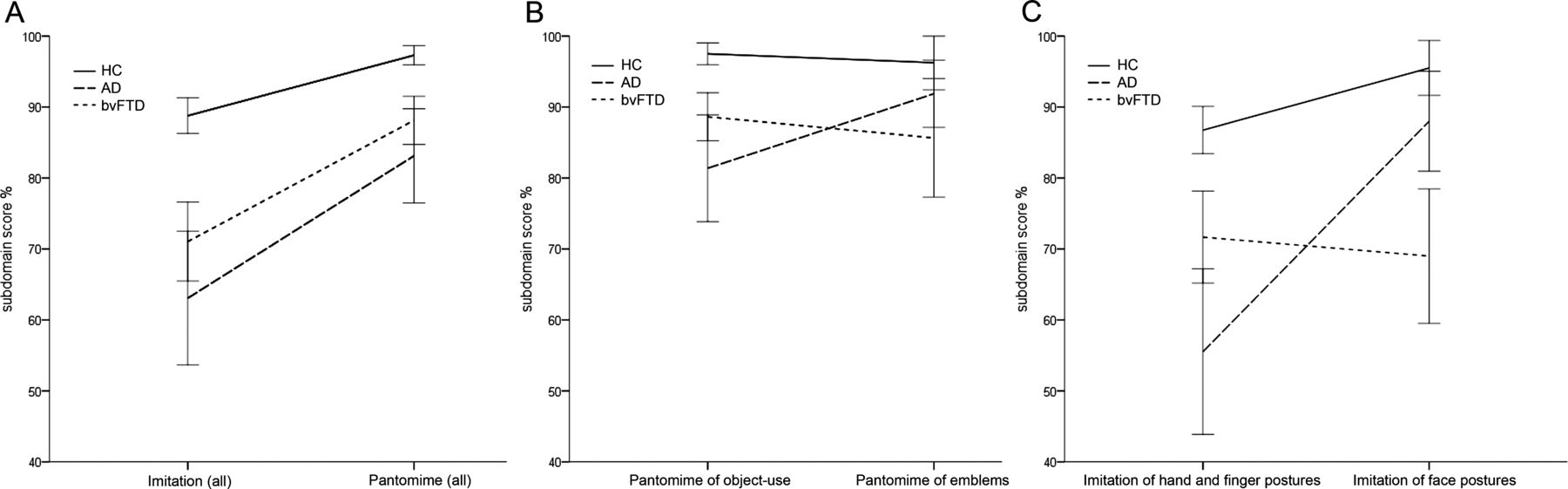
In order to substantiate these results and to further explore differences in apraxia profiles between patients with AD and bvFTD, we next directly contrasted corresponding subdomain pairs (figure 1) using three follow-up mixed-design 2×3 ANOVAs with subdomain as within-subject and group as between-subject factor. This enabled us to investigate possible differences between patient groups regarding the pattern of impairments, by looking at several apraxia subdomains at the same time. There was a significant group x subdomain interaction for the comparison imitation (all) versus pantomime (all), F(2, 57)=4.34, p=0.018. Inspection of the interaction plot suggests that patients with AD and bvFTD showed a similar but slightly disproportionate decline from pantomime to imitation when compared with HC (figure 3A). Comparison of pantomime of object use and pantomime of emblems revealed a highly significant interaction with group, F(2, 57)=5.14, p=0.009. Figure 3B shows that this interaction is mainly due to differences in performance between patients with AD and bvFTD which run counter to each other: patients with AD showed larger deficits in pantomime of object use compared with pantomime of emblems, whereas patients with bvFTD exhibited an opposite relationship. Concurrent comparison of imitation of hand and finger postures and imitation of face postures similarly indicated significantly diverging apraxia profiles between bvFTD, AD and HC, F(2, 57)=13.8, p=<0.001. Patients with AD displayed a disproportionately large imitational deficit for hand and finger postures compared with HC. Diametrically opposed to both other groups, patients with bvFTD displayed a unique profile of larger deficits for imitation of face postures compared with imitation of hand and finger postures (figure 3C), suggesting a specific profile of praxis deficits in both diseases.
{kind=link}
{kind=link}
{kind=link}
Group differences of apraxia subdomain scores. (A–C) ANOVA interaction plots for apraxia subdomain (within-subject) × group (between-subject) interactions (ANOVA, analysis of variance; AD, Alzheimer's dementia; bvFTD, behavioural variant frontotemporal dementia; HC, healthy controls).
Discussion
This study investigated apraxia in bvFTD and explored whether the profile of disturbances in praxis subdomains differed between AD and bvFTD in mild disease stages.
Diagnostic properties of composite apraxia scores
We found strong evidence for globally reduced performance in praxis tasks in patients with AD even at an early clinical stage in line with previous studies.24–26 However, these studies employed elaborate experimental tasks to quantify the level of apraxia, most of which are difficult to apply in clinical practice due to time constraints. We were able to replicate these findings using time-efficient, off-the-shelf clinical screening tests for apraxia.20 ,21 In particular the CAS, a newly developed test optimised to quantify subtle praxis disturbances in patients with stroke, showed a high sensitivity and specificity in distinguishing mild AD from HC. Performance of patients with bvFTD in standardised apraxia screenings was likewise significantly reduced compared with age-matched HC. The degree of impairment on composite apraxia scores was similar in patients with bvFTD and mild AD, suggesting that apraxia may be a common diagnostic marker for both neurodegenerative diseases. In view of the continuing challenge to diagnose bvFTD in mild clinical stages by employing highly standardised neuropsychological tests, our result is novel and promising: in terms of sensitivity and specificity estimates for differentiating bvFTD from a sample of neurologically healthy age-matched controls, composite apraxia scores in our study proved effective.
Apraxia profiles of patients with AD and bvFTD
Subsequent analyses of apraxia subdomains revealed significant differences between the two patient groups. We found patients with mild AD to be impaired in imitation as well as pantomime. The deficit was most pronounced for imitation of hand and finger postures. This result corroborates previous findings that imitating meaningless gestures may be among the earliest and most evident praxis deficits in AD.26 ,27 Accurate imitation of meaningless (ie, non-symbolic) hand and finger gestures places high demands on visuoperceptual analysis and requires a representation of relationships between body parts.28 Such impaired ‘body-part coding’ has previously been discussed as a cognitive mechanism for the imitational deficits seen in patients with left-brain stroke.4 There is vast neuroanatomic evidence that imitation of unknown gestures critically depends on (inferior) parietal lobe integrity.4 ,29 Owing to early atrophy in these areas, patients with AD may be particularly prone to impairments in this domain of apraxia. In contrast to imitation of meaningless gestures, pantomimes convey a familiar symbolic meaning. These gestures are usually well trained and thus may be guided by semantic memory.30 It has previously been shown that patients with AD can also be impaired on these more conceptual tasks of apraxia even in early disease stages.25 Nevertheless, accuracy in tasks on pantomimes of object use is positively influenced by semantic knowledge about objects and tool use.31 Impairments of semantic memory and conceptual knowledge become more evident in later stages of AD, possibly due to spreading of the pathology into areas of the anterior temporal lobe.32 This may explain our finding of relatively better performance of pantomime compared with imitation tasks in our sample of patients with mild AD.
Despite previously reported relative sparing of parietal atrophy in patients with bvFTD,12 we nevertheless found patients with bvFTD in our sample to be also impaired in both domains of apraxia, imitation and pantomime of gestures. At large, this finding adds to the growing evidence for a possible contribution of frontal brain areas to praxis tasks.4 ,8–11 ,29 Importantly, subsequent analyses showed differential profiles of praxis impairments in patients with bvFTD and AD. In contrast to patients with AD, the profile of patients with bvFTD was characterised by unique deficits in imitation of facial postures and to a lesser degree, by relatively more impairment in pantomimes of emblems. Imitation of gestures has been related to aspects of social cognition, including the ability to comprehend others’ actions but also others’ emotional and cognitive states via internal simulation processes.33 ,34 At a neural level, these processes are subserved by large scale functional networks, referred to as mentalising and mirror neuron system.35 These networks crucially involve areas in the frontal lobe, in particular medial prefrontal and orbitofrontal cortex,36 which are among the earliest target areas of neurodegeneration in bvFTD.12 Consequently, impairments in social cognition including facial emotion recognition37 have been reported to be sensitive markers for bvFTD, correlating with the degree of atrophy in these areas but also with clinical aspects of social conduct disturbances.13 ,38 Relating these findings to ours, intransitive communicative gestures (like the verbally requested pantomimes of emblems) and especially imitation of face postures may constitute social stimuli which are disproportionately affected by deficits in social cognition in patients with bvFTD. In this sense, the production deficits for face postures in bvFTD may be associated to an encoding deficit, as previously shown in these patients.37 Moreover, face apraxia has previously been reported in the language variants of frontotemporal lobar degeneration alongside with apraxia of speech.10 ,39 These studies showed associations between face apraxia and volume loss in left frontal brain areas, particularly the middle frontal gyrus, premotor cortex and frontal operculum, but most importantly not with parietal cortices. Furthermore, lesion studies in patients with damaged brain have consistently reported brain structures in the frontal lobe (eg, anterior insula) as symptom sites of face apraxia.40
Clinical implications
Since both patient groups showed pronounced impairments in standardised praxis tasks, it appears surprising that apraxia is not explicitly considered in current clinical diagnostic guidelines of either neurocognitive disorder.16 ,17 As apraxia is commonly investigated in the context of aphasia and stroke, it is generally under-represented as a potential cognitive dysfunction in neurodegenerative diseases.6 Previous evidence from studies on apraxia in dementia is scattered and results are hardly comparable, likely due to dissimilar and sometimes elusive definitions of apraxia, differing methods of assessment and usually small and clinically heterogeneous samples.6 Such methodological and conceptual issues may have concealed the clinical value of routine apraxia assessment as a supportive element for diagnosing dementia. Operational and more descriptive definitions of apraxia and praxis subdomains as established by modern screening tests appear well founded to overcome these issues.
Additionally, our result of disease-specific apraxia profiles regarding patterns of deficits in subdomains may prospectively be clinically relevant for differentiating AD and bvFTD in mild disease stages at single-case level. Whereas more research is needed to establish off-the-shelf apraxia tests specifically designed for this challenging task, our results appear promising and provide evidence that a separate examination of manifestations of apraxia can be fruitful for differential diagnoses (see also online supplementary table S2).
Limitations
In the current study, apraxia was defined and quantified by impaired behavioural performance in the domains of pantomime and imitation pertaining to different body parts, and therefore our conclusions on the incidence of apraxia in bvFTD only hold for these phenomena. It is currently unclear whether and to what extent other cognitive dysfunctions may account for some of the deficits in praxis tasks seen in patients with bvFTD. Since patients with bvFTD and AD may also differ in several other neuropsychological domains (eg, verbal comprehension, memory, visuospatial abilities) that may influence performance in praxis tasks, future studies are needed to evaluate these potential influences on apraxia in both diseases. However, whether or not apraxia in bvFTD is considered a distinct deficit or only as deduced from other neuropsychological dysfunctions, our results point to a specific apraxia profile in mild stages of the disease.
As MRI data on cerebral atrophy was not analysed quantitatively (eg, using voxel-based morphometry), we cannot be certain that for example, face apraxia is linked to frontal atrophy in patients with bvFTD. Related to this, future studies should also take into account variants of AD that display atypical ‘frontal’ atrophy patterns and assess apraxia within these syndromes to disentangle brain atrophy from the underlying neurodegenerative disease.
Furthermore, although we are not aware of an effect of gender on praxis performance, the unequal proportion of male and female patients within the bvFTD group could be a confounding factor and may limit a generalisation of our results.
Conclusions
Our study provides evidence of an impairment of patients with bvFTD in standardised apraxia screening tests. Composite scores of these easily applicable tests showed a high validity to distinguish AD and bvFTD from HC in mild stages of the diseases, and therefore should be considered in diagnostic workup. Moreover, apraxia profiles of bvFTD and AD differed significantly in performance on imitation of face postures with bvFTD presenting unique symptoms of face apraxia (refer to online supplementary video 1 for a sample video). Given that the differential diagnosis in mild stages of both diseases is still difficult, apraxia screening tests and particularly an analysis of subdomains could contribute to the diagnostic process and may prospectively aid to distinguish both diseases in mild stages. Future studies will be committed to explore the relation between different manifestations of apraxia with other neuropsychological and behavioural deficits in bvFTD (eg, with tasks for social cognition and emotion recognition). Additionally, the neural basis of our finding of praxis impairments in bvFTD requires to be investigated by relating apraxia scores and subdomains to specific structural cerebral changes on MRI and to hypometabolism on PET.
Acknowledgments
The authors would like to thank Sabine Bruchmann for assistance and help in patient acquisition; and Dr Pienie Zwitserlood for support and helpful comments on the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
- Data supplement 4 - Online video
Footnotes
AJ, TD and HL contributed equally to this study.
Contributors AJ contributed in the study concept and design, drafting of the manuscript, analysis and interpretation of the data, statistical analyses, acquisition of the data and study coordination. AT and AK were involved in the revising of the manuscript for content and acquisition of the data. HW was involved in the medical writing for content and study supervision. GL was involved in the medical writing for content. TD participated in the study conceptualisation, revising of the manuscript and study supervision. HL contributed in the study conceptualisation, interpretation of the data, revising of the manuscript and study supervision.
Funding This study was supported by the Stiftung Neuromedizin, Münster, Germany.
Competing interests AJ, GL and HL received honoraria for lecturing and travel expenses for attending meetings from Novartis Pharma GmbH. HW received speaker honoraria, consultation fees and grant support from Bayer-Schering, Biogen Idec, Merck-Serono, Novartis, Sanofi-Aventis, TEVA Pharma and Novo Nordisk. TD received honoraria and travel expenses from Genzyme, Shire, Bristol-Myers Squibb, Boehringer-Ingelheim Pharma, Sanofi Aventis, Wisai, Novartis, Bayer Vital, Merz Pharma, Actelion and Lundbeck for serving as a speaker and consultant. He received research support from Genzyme, Shire and Actelion. For conducting dementia studies TD received grants from Novartis and Merz Pharma.
Patient consent Obtained.
Ethics approval Local Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.