Article Text

Abstract
Objective Although a concern exists that 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) might increase the risk of intracerebral haemorrhage (ICH), the contribution of these agents to the relationship between serum cholesterol and disease occurrence has been poorly investigated.
Methods We compared consecutive patients having ICH with age and sex-matched stroke-free control subjects in a case–control analysis, as part of the Multicenter Study on Cerebral Haemorrhage in Italy (MUCH-Italy), and tested the presence of interaction effects between total serum cholesterol levels and statins on the risk of ICH.
Results A total of 3492 cases (mean age, 73.0±12.7 years; males, 56.6%) and 3492 control subjects were enrolled. Increasing total serum cholesterol levels were confirmed to be inversely associated with ICH. We observed a statistical interaction between total serum cholesterol levels and statin use for the risk of haemorrhage (Interaction OR (IOR), 1.09; 95% CI 1.05 to 1.12). Increasing levels of total serum cholesterol were associated with a decreased risk of ICH within statin strata (average OR, 0.87; 95% CI 0.86 to 0.88 for every increase of 0.26 mmol/l of total serum cholesterol concentrations), while statin use was associated with an increased risk (OR, 1.54; 95% CI 1.31 to 1.81 of the average level of total serum cholesterol). The protective effect of serum cholesterol against ICH was reduced by statins in strictly lobar brain regions more than in non-lobar ones.
Conclusions Statin therapy and total serum cholesterol levels exhibit interaction effects towards the risk of ICH. The magnitude of such effects appears higher in lobar brain regions.
Statistics from Altmetric.com
Introduction
Increasing evidence has suggested that serum cholesterol is inversely associated with the risk of intracerebral haemorrhage (ICH).1 In recent years, 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, or statins, have emerged as the most important class of cholesterol-lowering agents and among the most commonly prescribed drugs worldwide.2 In spite of the proven benefits of statins in reducing the risk of cardiovascular and cerebrovascular disease, the results of several studies have raised concerns about the risk of haemorrhagic stroke, mainly ICH, in people treated with these agents,3 ,4 which is presumed to be the consequence of decreased serum cholesterol concentrations. Some of the pleiotropic effects of statins, including decreased platelet aggregation and decreased thrombogenesis, could further increase the risk of cerebral bleeding.5 Although this potential risk, if any, is likely to be overshadowed by the large benefits in terms of reduction of individual susceptibility to cardiovascular disease, the clinical implications could be relevant, and clinicians should be asked to carefully consider this relation when prescribing statin therapy targeting low cholesterol goals. So far, the contribution of these agents to the link between serum cholesterol and ICH has been poorly investigated and the existing reports conflict with one another. Therefore, in the present study, we aimed at elucidating whether (1) there is a relationship between statin therapy and serum cholesterol, or vice versa, towards the risk of intracerebral bleeding and (2) such a relationship might vary according to the presumed mechanism of cerebral haemorrhage, in a cohort of Italian patients with ICH.
Material and methods
Study group and design
The Multicenter Study on Cerebral Haemorrhage in Italy (MUCH-Italy) is a countrywide network of neurological centres designed to investigate epidemiology, risk factors and consequences of ICH in the setting of a hospital-based, multicentre, prospectively-recruiting, observational study, coordinated by the University of Brescia.6 The MUCH-Italy study consists also of a biostatistical core (University of Pavia) and 19 Italian clinical recruiting centres. The institutional review board at each participating study centre provided approval for the study. Written informed consent was obtained from all participants (or next of kin). For the purpose of the present analysis, we screened data sets from patients with acute ICH consecutively admitted from 1 January 2002 to 31 July 2014.
Cases
Criteria for patient selection, risk factor definition, diagnostic procedures and assessment of haematoma location have been previously described.6 Briefly, eligibility for study participation required neuroimaging (CT or MRI) confirmation of haemorrhagic stroke. Exclusion criteria included the presence of trauma, brain tumour, haemorrhagic transformation of a cerebral infarction, vascular malformation or any other perceived cause of secondary ICH. ICH location was assigned based on admission CT scan by stroke neurologists at each participating centre. ICH isolated to the cortex (with or without involvement of subcortical white matter) and cerebellar haematomas were defined as lobar ICH, while ICH selectively involving the thalamus, basal ganglia or brainstem was defined as deep (non-lobar) ICH. Multiple concurrent bleeds involving deep and lobar territories were defined as mixed ICH and represented an exclusion criterion.
Control subjects
Control subjects were enrolled from the Moli-Sani project, an Italian population-based study recruiting citizens of the Molise region, an area between the Central and Southern regions, aimed at investigating the equilibrium between genetics and environment in the pathogenesis of cardiovascular, cerebrovascular and cancer disease.7 Individuals included were matched with cases by sex and age (±5 years), and were confirmed to have no medical history of stroke through interview and review of medical records.
Risk factor definition
A history of vascular risk factors was defined as the presence of these predisposing conditions, either in the personal medical history for both cases and control subjects or when identified during admission for patients with ICH. In particular, smoking was defined as currently smoking one or more cigarettes per day on a regular basis. Hypertension was defined as systolic blood pressure, BP >140 mm Hg and/or diastolic BP >90 mm Hg of the acute phase, or using pharmacological treatment for hypertension. Diabetes was defined as fasting glucose levels >6.9 mmol/L of the acute phase or current treatment with antidiabetic drugs. Based on daily alcohol consumption, participants were dichotomised into excessive drinkers (>45 g of alcohol) and light-moderate drinkers or non-drinkers. We also collected information on atrial fibrillation (medical history or electrocardiographic findings at admission), atherosclerotic peripheral arterial disease (medical history), coronary artery disease (medical history of angina, myocardial infarction, coronary artery bypass graft or percutaneous transluminal coronary angioplasty), history of previous stroke or transient ischaemic attack (based on clinical history) and pre-ICH medications (warfarin, aspirin or other antiplatelet agents, antihypertensive agents, oral hypoglycaemic agents or insulin and statins).
Measurement of serum lipid levels
Fasting lipids measurements were carried out on venous blood samples in each participating centre, using comparable enzymatic procedures. Admission total serum cholesterol levels were used for interaction analysis, while hypercholesterolaemia was defined as total serum cholesterol levels >6.2 mmol/L of the acute phase or using pharmacological treatment to lower blood lipids. Statin use included any of the following: atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin or simvastatin, or a combination of medications that included a statin. Current use of these cholesterol-lowering medications was defined as filling a prescription for such medications in the 6 months prior to the index date. Participants were classified as non-hypercholesterolaemic, hypercholesterolaemic under treatment with statins, or hypercholesterolemic not under treatment with statins. Data were obtained from interviews with patients, next of kin and/or attending physicians or general practitioners.
Statistical analyses
We compared the characteristics of patients with ICH and control subjects, using the χ2 test for categorical variables, and the independent-samples t test for continuous variables. Despite the matching criteria adopted for the selection of control individuals, this group was, on average, 3 years younger than cases. All multivariable analyses were, therefore, adjusted for age. We performed unconditional logistic regression models to examine the effect of selected risk factors in the prediction of disease status (case/control) in each of the three study subgroups (overall ICH, deep ICH and lobar ICH). In particular, we adjusted for those variables that might potentially influence the risk of cerebral bleeding, including age, hypertension (yes/no), diabetes mellitus (yes/no), hypercholesterolaemia (yes/no), current smoking (yes/no), daily alcohol intake (heavy drinkers/light-moderate drinkers or non-drinkers) and antithrombotic medications use (yes/no). As statin treatment might modify the association between total serum cholesterol levels and ICH, we investigated whether this relationship differed across strata of statin use, and tested the presence of interaction or modification effects. The modelling strategy assumed disease status (case/control) as outcome variable (Y), and total serum cholesterol concentrations (X) and statin use (Z) as predictors. In particular, we tested all the possible total serum cholesterol-statin use interaction logistic regression models (see online supplementary figure S1). The assessment of interaction models was performed without and with adjustment for the following covariates: age, systolic BP values, serum glucose levels, smoking habit, daily alcohol intake and use of antiplatelet agents and oral anticoagulants. To compare these competing models, we computed the Akaike' Information Criterion (AIC=−2×model log-likelihood+2×number of model parameters) and the Bayesian Information Criterion (BIC=−2×model log-likelihood+log(n)×number of model parameters). The selected model was the one minimising either AIC or BIC.8 The regression parameter estimates were re-expressed as ORs and Interaction ORs (IOR=OR(group1)/OR(group2)), and 95% CIs. For visualising main effects and interaction of total serum cholesterol levels (X) and statin use (Z) with covariates, we considered the ‘covariate contribution’ (CC=the sum of the covariates, excluding X and Z, multiplied by their corresponding logit coefficient), as suggested by Mitchell and Chen.9 This reflects the aggregate contribution of covariates when the predicted probabilities of outcome (Y) in the logistic model are represented in a two-dimensional plot. In particular, the probability plot displays the outcome probability Y as a function of the continuous variable X and the binary variable Z for low (20th centile) and high (80th entile) of CC. The threshold of statistical significance was set at p<0.05 for all analyses. Data were analysed using SPSS for Windows V.16.0 (SPSS Inc, Chicago, Illinois, USA) package (http://www.spss.com) and our codes in R.10
Supplemental material
Results
A total of 3492 patients with ICH (mean age, 73.0±12.7 years; males, 56.6%) and 3492 control subjects (mean age, 70.6±10.5 years; males, 56.6%) were eligible for inclusion in the present study. All participants were Caucasian. Based on the location of the haematoma, 1604 (45.9%) patients were categorised as lobar ICH cases, while 1888 (54.1%) were considered deep (non-lobar) ICH cases. Demographic and baseline clinical characteristics of the study group are summarised in table 1, stratified by haematoma location. Compared to control subjects, cases were more likely to have a pre-ICH history of coronary artery disease, hypertension and diabetes, and to be prescribed antithrombotic medications. Their mean serum glucose levels, as well as systolic and diastolic BP values at the time of presentation were also higher. Conversely, they were less likely to have a history of hypercholesterolaemia and their mean serum total cholesterol concentration was lower.
Baseline demographics and clinical characteristics of the MUCH-Italy study group according to haemorrhage location
Table 2 summarises the associations between selected predisposing factors and the risk of ICH. The effect of hypertension, diabetes mellitus and heavy alcohol consumption in increasing the risk of cerebral bleeding was prominent in non-lobar regions, whereas the use of antithrombotic medications was more strongly associated with lobar location of the haematoma. In contrast, we did not detect any association between current smoking and ICH, regardless of haemorrhage location. Of note, the protective effect of hypercholesterolaemia was apparently attenuated by statin use, especially in the subgroup of patients with lobar ICH.
Multivariable ORs for intracerebral haemorrhage by location
The AIC index and BIC index signed the ‘total serum cholesterol-statin use complete interaction model’ (see online supplementary figure S1, model 8) as the best in predicting the effect of statins and total serum cholesterol levels on ICH risk (see online supplementary table S1 and S2). Effects estimates for the interaction between statin use and total serum cholesterol levels, re-expressed as ORs, are displayed in table 3. The interaction between total serum cholesterol levels and statin use for the risk of haemorrhage was statistically significant (IOR, 1.09; 95% CI 1.05 to 1.12 for ICH regardless of haemorrhage location; IOR, 1.13; 95% CI 1.08 to 1.19 for strictly lobar ICH; IOR, 1.07; 95% CI 1.01 to 1.13 for deep ICH). Therefore, the effects of cholesterol and statins were not conditionally independent, but average effects. Overall, increasing levels of total serum cholesterol were associated with a decreased risk of ICH within statin strata (average OR, 0.87; 95% CI 0.86 to 0.88 for every increase of 0.26 mmol/L of total serum cholesterol concentrations), an average effect that did not change substantially according to the location of cerebral haematoma (OR, 0.86; 95% CI 0.84 to 0.88 for strictly lobar ICH; OR, 0.88; 95% CI 0.86 to 0.90 for deep ICH). Conversely, statin use was associated with an increased risk of ICH at the average level of total serum cholesterol (5.7 mmol/L: OR, 1.54; 95% CI 1.31 to 1.81 for ICH regardless of haemorrhage location; OR, 1.58; 95% CI 1.28 to 1.96 for strictly lobar ICH; OR, 1.44; 95% CI 1.14 to 1.82 for deep ICH). These findings were not substantially affected by adjustment for covariates, except for the effect of statins on the risk of ICH, which was strongly attenuated and became non-significant in the multivariable model. Statin use resulted in a less dramatic change in the risk of cerebral bleeding across cholesterol values compared to non-statin use.
Interaction analysis of serum total cholesterol levels and statin therapy on the risk of intracerebral bleeding stratified by haemorrhage location
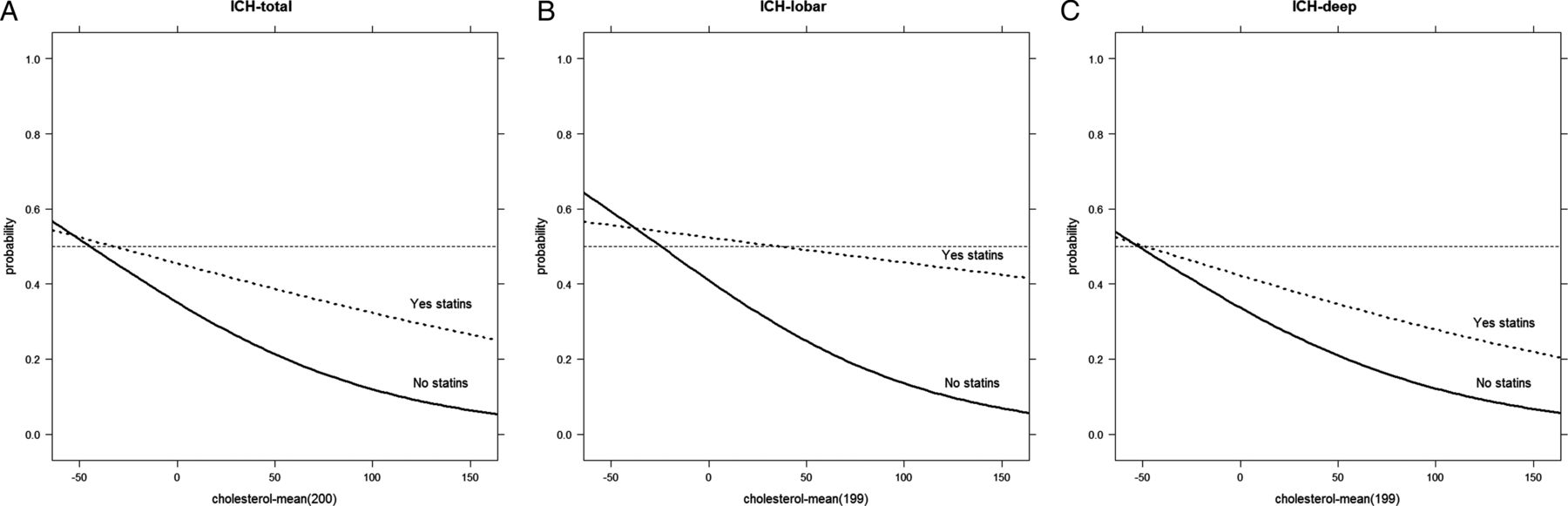
Statin use, in particular, turned out to reduce the protective effect of total serum cholesterol against ICH, especially in strictly lobar brain regions more than in non-lobar ones (figure 1 and see online supplementary figure S2). We observed a direct, linear, slightly increased predicted probability of ICH with increasing serum concentrations of total cholesterol in the subgroup of patients under treatment with statins, an effect that was prominent in the subgroup of patients with haemorrhage located in lobar brain regions compared to the whole cohort or to the subgroup of patients with non-lobar ICH.

{kind=link}
Predicted probability (risk) of overall ICH (A), lobar ICH (B) and deep ICH (C), for total cholesterol and statin use. ICH, intracerebral haemorrhage.
Discussion
The question of whether cholesterol-lowering drugs might be involved in the relationship between serum lipids, including cholesterol and ICH, has been a matter of long debate. In particular, it is still unclear whether statin use may confer an increased risk of cerebral bleeding. The results of our study provide, therefore, further information on this theme and novel insights into the role of serum lipids in the aetiology of ICH.
In line with a number of prior reports,1 as well as with the results of in vitro and animal studies,11–13 we confirmed that total serum cholesterol concentrations are inversely associated with the risk of ICH. Owing to the observational nature of our analysis, however, the extent to which serum cholesterol can be judged causal in the occurrence of ICH is difficult to assess, and it could be that low cholesterol levels might simply be an epiphenomenon of the individual propensity to cerebral haemorrhage. Although we cannot definitively rule out this alternative interpretation, the dose-dependent relationship we found (approximately 12% decreased risk of ICH for every increase of 0.26 mmol/L in total serum cholesterol concentration) might be considered, however, an argument in favour of the hypothesis of a pathogenic link between serum cholesterol and cerebral haemorrhage.
Our findings also suggest that statin use before the index event might be related to intracerebral bleeding. A number of previous studies have highlighted the fact that statins, besides their effects as cholesterol-lowering agents, exhibit a wide range of antithrombotic properties, as a consequence of their modulatory effects on profibrinolytic mechanisms, blood coagulation cascade and platelet functions.5 ,11 ,14 These effects could theoretically account for an increased risk of bleeding complications. Based on our data, the contribution of statins to the risk of cerebral bleeding might occur, at least in part, through their effect on serum total cholesterol levels. In particular, the use of statins seems to reduce the strength of the inverse association between cholesterol and ICH, so that any protective influence of hypercholesterolaemia might be attenuated by the cholesterol-lowering effect of these agents. These findings, indirectly, reinforce the assumption that total cholesterol might be related to the occurrence of brain haemorrhage, and make the influence of confounders, such as general medical or nutritional status, unlikely.15 On the other hand, however, they are at odds with the results of previous meta-analyses of statin therapy, which found no increased risk of haemorrhagic stroke in participants taking these medications.16–19 In particular, the inconsistency between the results from randomised clinical trials18 ,19 and our findings is substantial, and calls for further investigation on how exactly cholesterol and statins affect stroke risk in order to explain this striking discrepancy. It should be noted, in this regard, that most of the previous studies on this topic were based on conventional regression models that allow quantification of the strength of the independent association of each factor (ie, statins use or cholesterol level) with disease risk but do not allow evaluation of the interaction’s effects among these factors. What distinguishes our study from others is the application of a regression model that is able to explore and quantify the cholesterol-statin interactions and illustrate how these interactions influence outcome.
Another finding from our data is the differential patterns of association, the strongest effect of statins being detected in the subgroup of patients with strictly lobar haemorrhage, likely related to cerebral amyloid angiopathy.20 In agreement with our findings, statin therapy has been associated with an increased prevalence and severity of cerebral microbleeds in cortical-subcortical brain regions,21 ,22 as well as with a higher propensity for lobar ICH in a recent epidemiological study with the same case–control design as ours.23 This supports the hypothesis of a different susceptibility of cerebral small vessels to the effect of serum lipids and statins.
The MUCH-Italy collaborative study differs from previous epidemiological analyses on this topic in several ways that increase its reliability and precision: it is large, involving more than twice the number of participants included in previous observational studies with the same design; it is based on rigorous case–control matching and racial homogeneity; fasting total serum cholesterol levels are available for most of the participants, which implicates the ability to perform adequate interaction analyses; and it has the advantages of hospital-based recruitment, including detailed and standardised data collection with little missing information, and complete radiological data allowing exploration of the effect of confounders on the cholesterol–statins–ICH relationship. Nevertheless, we are aware of several limitations. We did not control for statin dosing, duration of treatment or compliance, because these data were not collected. The same is true for the lack of cholesterol fractions, such as high-density lipoprotein and low-density lipoprotein concentrations, as well as for the absence of repeated measures of cholesterol, which does not allow the ruling out of intraindividual fluctuations in serum levels over time. Another caveat is the possibility that vascular disease can itself directly or indirectly affect blood cholesterol concentration because of the influence that the acute phase reaction to ICH might have had on admission levels in the group of cases. Although these drawbacks are noteworthy, we believe they do not alter the obvious clinical implication of our findings.
Conclusions
Although we cannot dispute the fact that the potential risk of ICH associated with statin use, if any, is unlikely to overshadow the large benefits conferred by lipid-lowering medications in reducing cardiovascular events, including ischaemic stroke,2 clinicians should carefully consider bleeding susceptibility when prescribing statin therapy targeting reduced cardiovascular risk. Identification of those statin users who are more prone to develop this complication will be the goal of future research.
References
Footnotes
Contributors APe and MG were responsible for study concept and design, interpretation of data, data analysis and Statistical analysis. APe was responsible for drafting of the manuscript, administrative, technical and material support. APe and APa were responsible for supervision of the study. All the authors were responsible for acquisition of data and critical revision of the manuscript for important intellectual content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.