Article Text

Abstract
Objective To electrophysiologically classify an Italian Guillain–Barré syndrome (GBS) population into demyelinating and axonal subtypes, to investigate how serial recordings changed the classification and to underline the pitfalls in electrodiagnosis of GBS subtypes.
Methods The authors applied two current electrodiagnostic criteria sets for demyelinating and axonal GBS subtypes in 55 patients who had at least two serial recordings in three motor and sensory nerves.
Results At first test, the electrodiagnosis was almost identical with both criteria: 65–67% of patients were classifiable as acute inflammatory demyelinating polyradiculoneuropathy (AIDP), 18% were classifiable as axonal GBS, and 14–16% were equivocal. At follow-up, 24% of patients changed classification: AIDP decreased to 58%, axonal GBS increased to 38%, and equivocal patients decreased to 4%. The majority of shifts were from AIDP and equivocal groups to axonal GBS, and the main reason was the recognition by serial recordings of the reversible conduction failure and of the length-dependent compound muscle action potential amplitude reduction patterns as expression of axonal pathology.
Conclusions Axonal GBS is pathophysiologically characterised not only by axonal degeneration but also by reversible conduction failure at the axolemma of the Ranvier node. The lack of distinction among demyelinating conduction block, reversible conduction failure and length-dependent compound muscle action potential amplitude reduction may fallaciously classify patients with axonal GBS as having AIDP. Serial electrophysiological studies are mandatory for proper diagnosis of GBS subtypes and the identification of pathophysiological mechanisms of muscle weakness. More reliable electrodiagnostic criteria taking into consideration the reversible conduction failure pattern should be devised.
- Guillain-Barré Syndrome
- clinical neurophysiology
- neurophysiology
- clinical
Statistics from Altmetric.com
Introduction
Guillain–Barré syndrome (GBS) is divided into three major subtypes: acute inflammatory demyelinating polyradiculoneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor and sensory axonal neuropathy (AMSAN). AIDP is most frequent in Western countries, whereas AMAN is common in China and Japan.1–5 AMAN and AMSAN have been associated with antecedent Campylobacter jejuni (C jejuni) infection and autoantibodies to gangliosides, especially to GM1 and GD1a.2–7 In AMAN and AMSAN, the pathology is consistent with an antibody-mediated primary axonal damage at the Ranvier node.8–11
AIDP, AMAN and AMSAN are difficult to distinguish on clinical grounds, and electrophysiology plays a determinant role in GBS diagnosis and classification, and in establishing the prognosis. AMAN is currently diagnosed by an absence of demyelinating features and decrease in distal compound muscle action potential amplitude.3 4 However, some GBS patients with IgG to gangliosides showed besides axonal features rapid resolution of conduction block (CB) and conduction slowing without development of temporal dispersion or restoration of F-waves without increased latency.12–15 These findings were thought to be incompatible with demyelination and remyelination, and indicated that AMAN is characterised not only by axonal degeneration but also by ‘reversible conduction failure,’ possibly induced by anti-ganglioside antibodies at the axolemma of the Ranvier node.12 15
The aim of this study was to electrophysiologically classify an Italian GBS population according to the current criteria, to investigate how serial recordings changed the initial classification and to underline the possible pitfalls in electrodiagnosis of GBS subtypes.
Methods
Patients
We reviewed the clinical and electrophysiological records of patients discharged with the diagnosis of GBS from the University Hospital of Chieti between January 1995 and June 2009, and selected patients with progressive weakness of more than one limb with or without sensory symptoms or signs, who had at least two electrophysiological recordings in at least three motor and three sensory nerves. Fifty-five patients fulfilled these requirements. All patients signed an informed consent for utilisation of personal data, storage and assay of biological materials for research purposes.
Electrophysiology
Motor conduction studies were performed by a Nicolet Viking IV machine (Nicolet, USA). Amplitude and duration of negative peak of compound muscle action potential (CMAP) from distal (dCMAP) and proximal (pCMAP) stimulation, conduction velocity (CV), distal motor latency (DML) and minimal F-wave latency were measured. Sensory studies were performed antidromically in median and ulnar nerves, orthodromically in sural nerve. Amplitudes of sensory nerve action potentials (SNAPs) were measured baseline to negative peak. For DML, CV and F wave latency we defined the upper and lower limit of normal as the mean±2.5 SD of control values of our laboratory. For CMAP and SNAP amplitude the lower limit of normal was calculated as the mean±2.5 SD of the logarithmically transformed amplitudes of the controls. Electrophysiological findings in patients were expressed as percentages of upper and lower limits of controls. In serial recordings of the same patients dCMAP amplitude was considered significantly increased when higher than 50% of the value found at the first study. Electrophysiology was performed in each patient at least twice in the same motor and sensory nerves. The total number of tests was 170. The first test was performed within 15 days from onset of symptom (mean 9 days; range 2–15 days) and the results employed for the electrodiagnosis at first study. When a patient had more than one follow-up test the recording which we considered most informative was utilised for the final electrodiagnosis. The mean interval between disease onset and the most informative test was 28 days (range 7–70 days). EMG of biceps brachialis, first dorsalis interosseous, quadriceps femoralis and tibialis anterior was performed in at least one follow-up test and spontaneous activity was graded semiquantitatively as absent, mild, moderate and abundant.
Electrodiagnostic criteria
Box 1 lists the electrodiagnostic criteria sets used in the initial test. In Ho's criteria, evidence of ‘unequivocal temporal dispersion’ is found among the parameters to assess demyelination.3 Since how much temporal dispersion of CMAP should be considered ‘unequivocal’ was not defined, we used an increased duration of negative peak of pCMAP ≥30% compared with dCMAP.16 Hadden and colleagues replaced unequivocal temporal dispersion with CB defined as a pCMAP/dCMAP amplitude ratio less than 0.5.4 AMSAN was diagnosed by an absence of demyelinating features, as in Ho's criteria, and reduction in sensory nerve action potential amplitude <50% of lower limit of normal in at least two nerves.8 17 Patients not fulfilling the criteria for AIDP, AMAN and AMSAN were classified as equivocal. The reasons for classification changes at follow-up are reported in the Results.
Box 1 Criteria for electrophysiological classification
Acute inflammatory demyelinating polyradiculoneuropathy
(a) Ho et al3
Patients must have one of the following in two or more nerves during the first 2 weeks of illness:
Motor conduction velocity <90% lower limit of normal (LLN) (<85% if amplitude of compound muscle action potential after distal stimulation (dCMAP) is <50% LLN)
Distal motor latency >110% upper limit of normal (ULN) (>120% if dCMAP is <100% LLN)
Evidence of unequivocal temporal dispersion
F-response latency >120%
(b) Hadden et al4
At least one of the following in each of at least two nerves, or at least two of the following in one nerve if all others inexcitable and dCMAP≥10% LLN:
Motor conduction velocity<90% LLN (<85% if dCMAP is <50% LLN)
Distal motor latency >110 % ULN (>120% if dCMAP is <100% LLN)
amplitude of compound muscle action potential after proximal stimulation/dCMAP ratio <0.5 and dCMAP ≥20% LLN
F-response latency >120%
Acute motor axonal neuropathy
(c) Ho et al3
No evidence of demyelination as defined in (a)
dCMAP <80% LLN
(d) Hadden et al4
None of the features of demyelination in any nerve as defined in (b) (except one demyelinating feature allowed in one nerve if dCMAP is <10% LLN)
dCMAP <80% LLN in at least two nerves
Acute motor and sensory axonal neuropathy
(e) Feasby et al,8 Rees et al17
No evidence of demyelination as defined in (a)
dCMAP <80% LLN in at least two nerves
Sensory nerve action potential <50% LLN in at least two nerves
C jejuni serology and definition of antecedent C jejuni infection
Sera from 51 of 55 patients were tested for the presence of IgA and IgG against C jejuni by enzyme-linked immunosorbent assay (ELISA).18 Subjects were considered to have had an antecedent C jejuni infection if they had a positive stool culture for C jejuni or a high optical density for both IgA and IgG classes at dilution of 1:200 and 1:2000 and a definite history of a diarrhoeal illness within the previous 3 weeks before disease onset.
Antiganglioside antibody testing
Serum IgG and IgM to gangliosides GM1, GD1a and GD1b were tested in acute phase sera by ELISA.18 Serum was considered positive when showing an antibody of IgM and IgG or only IgG class with titre ≥1:400.
Statistical analysis
Patients were grouped according to final electrodiagnosis, presence or not of antecedent C jejuni infection, and presence or not of antiganglioside antibodies. Comparative analyses were made with the Fisher exact test. Results were considered significant if p<0.05.
Results
Electrodiagnosis at first test
In the first neurophysiological test, 37 of 55 patients (67%) fulfilled Hadden's criteria for AIDP, 10 patients (nine AMAN, one AMSAN; 18%) for axonal GBS and eight (14%) were classified as equivocal. According to Ho's criteria, 36 patients (65%) were classified as AIDP, 10 as axonal GBS (nine AMAN, one AMSAN; 18%) and nine (16%) equivocal (figure 1).

Electrodiagnosis of Guillain–Barré syndrome (GBS) patients in the first study and after serial recordings. The arrows indicate the directions of changes from a subtype to another, and the numbers indicate the subjects changing group. AIDP, acute inflammatory demyelinating polyradiculoneuropathy.
Follow-up and reasons for changes of electrodiagnosis
Thirty patients initially classified as AIDP according to both criteria did not change classification at follow-up. Two patients, initially classified according to both criteria as equivocal, developed definite demyelinating features and were reclassified as AIDP. Fourteen of 32 patients (23%) with a final diagnosis of AIDP developed mild to moderate spontaneous activity in at least one muscle. The 10 patients initially classified as axonal GBS showed at follow-up dCMAP amplitudes substantially unchanged or further reduced, with some nerves becoming unexcitable, without the development of any demyelinating features and confirming a motor axonal degeneration pattern (figures 2A, 3A). All 10 patients developed moderate to abundant spontaneous activity at EMG. Therefore, none of these subjects changed the initial electrodiagnosis. Two patients according to Hadden's criteria and three patients according to Ho's criteria classified at the first study as equivocal developed amplitude reduction in dCMAPs and in one patient of SNAPs and were finally diagnosed as axonal subtypes. All three patients showed moderate to abundant spontaneous activity at EMG.

Patterns of motor conduction abnormalities. Superimposed compound muscle action potentials (CMAPs) recorded from the abductor digiti minimi after ulnar nerve stimulation at the wrist, below-elbow and above-elbow and from the abductor pollicis brevis after median nerve stimulation at the wrist and elbow. (A) Acute motor axonal degeneration pattern: ulnar nerve. Distal CMAP amplitude was already decreased (4 mV) on day 4 and further decreased (2 mV) on day 11. The patient had IgG anti-GM1 and anti-GD1a. (B) Length-dependent CMAP amplitude reduction pattern: ulnar nerve. On day 2, there was a mild reduction (28%) of CMAP amplitude from below-elbow stimulation compared with wrist stimulation and an abnormal amplitude reduction in CMAP (65%) from above-elbow compared with below-elbow stimulation. At day 11, all CMAP amplitudes were reduced, and there was an abnormal amplitude reduction (64%) of CMAP from below-elbow stimulation compared with wrist, whereas the CMAP amplitude drop across the elbow was decreased (29%). At day 26, distal CMAP amplitude was further decreased, but amplitude reductions in CMAPs from proximal stimulation sites were no longer evident. The patient had IgG anti-GM1 and anti-GD1a. (C) Reversible distal conduction failure pattern: median nerve. On day 6, distal and proximal CMAP amplitudes were reduced (2.6 mV). On day 12, distal CMAP was increased 142%, returning within the normal range. There was no excessive temporal dispersion of proximal or distal CMAP in all recordings from day 6 to day 25. The patient had IgG anti-GD1b. (D) Reversible conduction failure pattern in intermediate nerve segments. Ulnar nerve. On day 10, there was a partial CB across the elbow which improved on day 20 and resolved at day 27 without the development of excessive temporal dispersion. The patient had IgG anti-GM1, anti-GD1a and anti-GD1b. (E) Acute inflammatory demyelinating neuropathy pattern: ulnar nerve. On day 2, all conduction parameters were normal. On day 14, all CMAPs were dispersed, distal CMAP amplitude was greatly reduced (1 mV), distal motor latency was increased (5.7 ms), the CMAP amplitude ratio between below-elbow and wrist stimulation was 0.2, and conduction velocities were reduced (20 m/s in the below-elbow wrist segment and 26 m/s across the elbow). On day 40, the CMAP amplitude ratio between below-elbow and wrist stimulation was 0.5 but all CMAPs were still reduced in amplitude and dispersed, DML was further increased (7.2 ms) and conduction velocities reduced (19 m/s in the below-elbow wrist segment and 16 m/s across the elbow). The patient did not have antiganglioside antibodies.
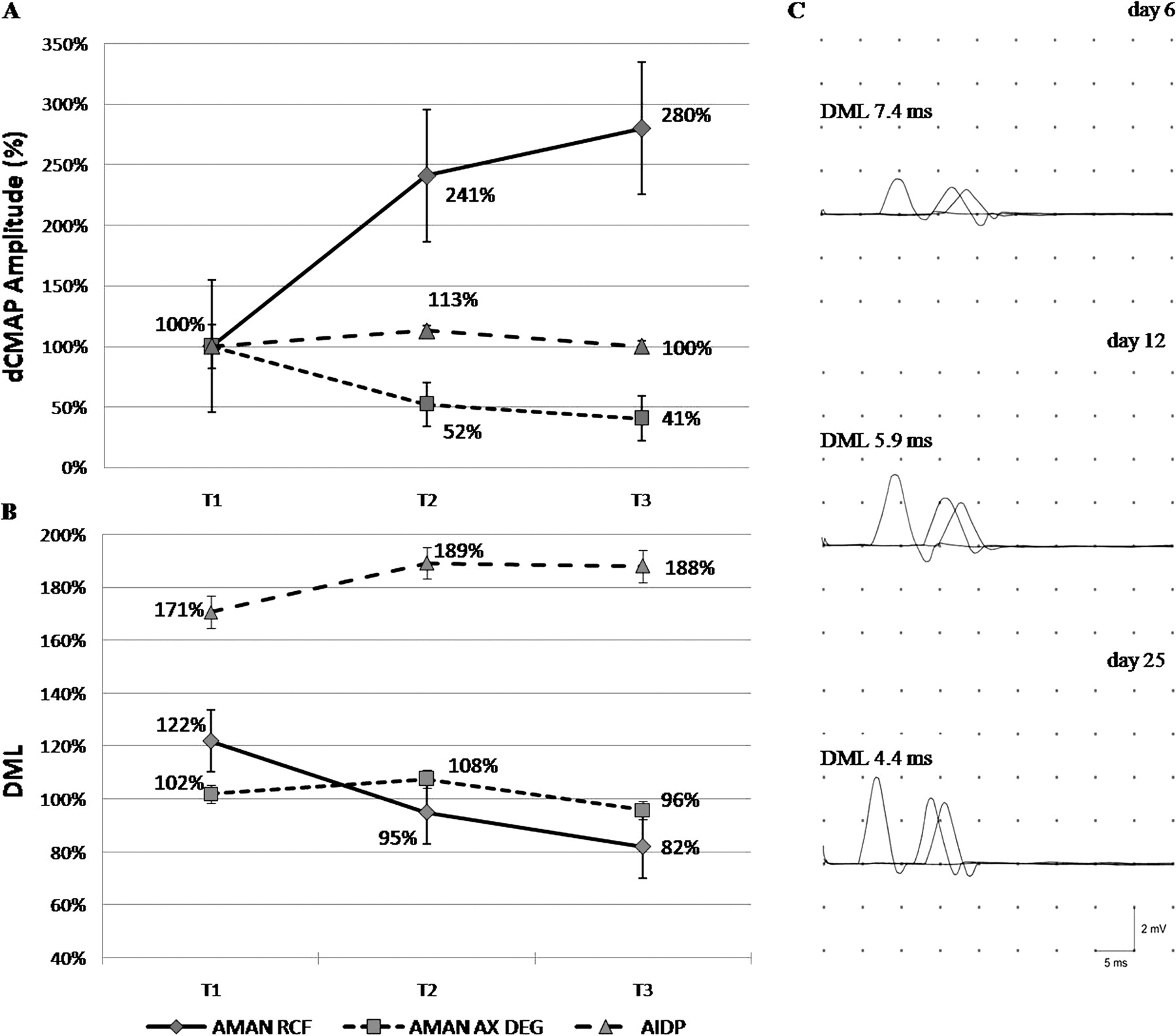
Serial electrophysiological findings in patients with axonal Guillain–Barré syndrome and acute inflammatory demyelinating polyradiculoneuropathy (AIDP). The abscissae contain three time intervals of recordings after disease onset: T1=1–10 days, T2=11–20 days, T3=21–30 days. Ordinates: (A) distal compound muscle action potential (dCMAP) amplitudes expressed as percentages of values at first recordings considered 100%. Linear graphs of 18 nerves of patients with AIDP without antiganglioside antibodies, 17 nerves of patients with acute motor axonal neuropathy (AMAN) and reversible distal conduction failure (AMAN RCF) and antiganglioside antibodies and 10 nerves of patients with AMAN and axonal degeneration (AMAN AX DEG). Ordinates: (B) distal motor latencies (DMLs) expressed as percentages of upper limits of controls. Linear graphs 18 nerves of patients with AIDP without antiganglioside antibodies, 11 nerves of patients with AMAN RCF prolonged distal motor latencies (DMLs) and antiganglioside antibodies and 10 nerves of patients with AMAN AX DEG and antiganglioside antibodies. Vertical bars are standard errors. (C) Compound muscle action potentials recorded from the extensor digitorum brevis muscle after stimulation of peroneal nerve at ankle, below-fibular head and above-fibular head in a patient with antibodies to GD1b. On day 6, DML is prolonged and dCMAP amplitude reduced (1.6 mV). On day 12, DML is slightly prolonged, and dCMAP amplitude is increased 106%. On day 25, DML is in the normal range, and the dCMAP amplitude is 150% increased compared with day 6.
In the first study, three patients showed a progressive CMAP amplitude reduction along the nerve length (figure 2B) fulfilling in some segments the criterion for CB in at least one nerve. According to Hadden's criteria, two patients were classified as AIDP, whereas the other was classified as equivocal. According to Ho's criteria, one patient was classified as AIDP, and the other two were equivocal. Serial recordings showed that dCMAP amplitudes decreased, becoming comparable with the pCMAPs with the disappearance of CB without development of excessive temporal dispersion or other features of demyelination (figure 2B). All three patients showed abundant spontaneous activity at EMG. We interpreted this length-dependent CMAP amplitude reduction as being due to progressive loss of excitability in fibres undergoing axonal degeneration, and these patients were finally classified as axonal GBS.19–21
Partial motor CB was found in intermediate nerve segments in at least two nerves in four patients and in one nerve in other two patients. CB was localised in six ulnar nerves of four patients in the segment across the elbow with slow CV (range 24–38 m/s) (figures 2D, 4). In five of these six patients, DMLs were prolonged in 11 nerves (mean 122% of ULN, range 110–147%) reaching the cut-off for demyelination (figure 3B). Four of these six patients were classified on the basis of the first study according to both criteria as AIDP and two patients as equivocal. At serial recordings, partial CB resolved rapidly without development of excessive temporal dispersion of dCMAPs or pCMAPs in all nerves (figures 2D, 4), and CV improved, returning to normal values in parallel with resolution of CB (figure 4). In 17 nerves, dCMAP amplitude promptly increased with a mean of 141% (range 67–350%) within a mean interval between the first study and follow-up of 9 days (range 6–17 days) (figures 2C, 3A). DMLs, when prolonged, returned to normal values within 3 weeks (figure 3B). The time course of electrophysiological abnormalities in the nerves of these six patients was clearly different from what found in nerves of patients with AIDP and AMAN with axonal degeneration (figures 2, 3). Only two of six patients developed mild spontaneous activity at EMG. These six patients were finally classified as axonal GBS with reversible conduction failure.12–15

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serial electrophysiological findings in ulnar nerves of two patients with acute motor axonal neuropathy (AMAN) and reversible conduction failure. The ordinates are: (A) ratios between amplitudes of proximal (above elbow) and distal (below elbow) compound muscle action potential (P/D CMAP); (B) P/D CMAP duration ratios; (C) conduction velocity (CV) in the segment above–below elbow (continuous line) and below–elbow wrist (dashed lines). The abscissae show the days. Time 0 is the time of the first recordings which were done between day 2 and day 7 after the disease onset. CVs improved in the above–below elbow segment in parallel with the resolution of conduction block without development of excessive temporal dispersion of proximal CMAPs. These patients had antiganglioside antibodies.
Final electrophysiological classification
Because of the better definition of electrophysiological abnormalities at follow-up, the recognition of the reversible physiological conduction failure and of the length-dependent CMAP reduction patterns as expressions of axonal pathology, 13 subjects (24%) changed classification (figure 1). Overall 32 patients (58%) were finally classified as AIDP, 21 (38%) were finally classified as axonal GBS (18 AMAN, three AMSAN), and two (4%) remained equivocal (figure 1). In the AIDP subtype, 56% of patients had pain, 73% had paraesthesias, and 64% had sensory loss. In the AMAN subtype, 38% of patients had pain, 16% had paraesthesias, and none had sensory loss. All three AMSAN patients had paraesthesias and sensory loss; pain was present in one patient.
Relations between final electrodiagnosis, antecedent C jejuni infection and antiganglioside antibodies
Twenty-one of 51 (41%) GBS patients had antecedent C jeuni infection. Sixteen of 19 patients (84%) with axonal GBS and five of 30 patients (17%) with AIDP had antecedent C jeuni infection. The difference was highly significant (p=0.000004).
The two patients who remained equivocal at follow-up did not have antecedent C jeuni infection.
Antibody to GM1 was present in eight AIDP and 12 axonal GBS (two with reversible conduction failure). Antibody to GD1a was present in five AIDP, and 13 axonal GBS (three with reversible conduction failure). Antibody to GD1b was present in six AIDP and eight axonal GBS (three with reversible conduction failure). Overall, at least one antibody to gangliosides GM1, GD1a or GD1b was present in 28 of 55 (51%) GBS patients, in 19 of 21 (90%) axonal GBS and in nine of 32 (28%) AIDP patients. The difference was highly significant (p=0.000007). Eight of 10 patients who were classified as axonal GBS at first test and did not change classification at follow-up had antibodies to gangliosides. The three patients with the length-dependent CMAP amplidute reduction pattern and the six patients with the reversible conduction failure pattern had antibodies to gangliosides. The two patients who remained equivocal at follow-up did not have antiganglioside antibodies.
Fifteen of 19 (79%) patients with axonal GBS had antecedent C jejuni infection and at least one antiganglioside antibody. However, only four (13%) of 30 AIDP patients had antecedent C jeuni infection and at least one of the tested antibodies to gangliosides. The difference was highly significant (p=0.000002).
Discussion
The percentages of patients with demyelinating and axonal GBS vary substantially in different series.3 4 22 23 This may be due to genetic susceptibility, different triggering factors, electrophysiological criteria used and whether the electrodiagnosis was based on a single or serial studies. Ho and colleagues in 129 Chinese patients, classified by a single test, found 65% AMAN, 24% AIDP and 11% unclassifiable patients.3 Hadden and colleagues applied their criteria to 369 GBS patients from 11 Western countries examining the results of two electrophysiological tests performed approximately 4 weeks apart.4 In the first test, 69% of patients met the criteria for AIDP, and 3% met the criteria for AMAN, the remaining patients being equivocal or showing unexcitable nerves. In the second test, although the final proportions of AIDP and AMAN were similar, many subjects changed classification. More recently, in 51 Indian patients applying Ho's criteria to the results of a single test, 86% of patients had AIDP and 14% axonal GBS, whereas in 41 patients from Israel, using the results of two studies performed within 4 weeks from onset, the percentage of AIDP was 63% and of axonal GBS 37%.22 23 In the GBS series, we report that electrodiagnosis was almost identical at the first test with both criteria, but at follow-up, 24% patients changed classification. The main shifts were from AIDP and equivocal groups to axonal group, which at follow-up resulted twice as much in number. The principal reason was the individuation of CBs rapidly resolving without the development of dispersed CMAPs due to remyelinating, slow conducting, desynchronised components which are characteristic of the evolution of CB due to segmental demyelination.24–26 This feature, denominated reversible conduction failure, has been described in some Japanese AMAN patients and in a GBS subtype named acute motor conduction block neuropathy (AMCBN) and ascribed to an antibody-mediated impaired physiological conduction at the axolemma of nodes of Ranvier.12–15 27–30 The pathophysiology of AMAN with axonal degeneration, AMAN with reversible conduction failure and AMCBN can be explained by the experimental model of axonal GBS. In the rabbit, the immunopathological cascade starts with IgG deposit at the axolemma of Ranvier nodes, followed by complement activation with the final formation of the membrane attack complex, disruption of nodal sodium channel clusters, detachment of paranodal myelin terminal loops and lengthening of the nodal region.31 All these changes lower the safety factor for impulse transmission and, when transposed to humans, suggest that at an early stage, the immunological reaction at nodal axolemma may induce a potentially reversible conduction failure. If the immune reaction progresses with the formation of membrane attack complex pores and calcium entry in the axon, a process of cytoskeletal degradation and mitochondrial injury develops with axonal damage and Wallerian-like degeneration. To support a continuum between reversible conduction failure and axonal degeneration, a reversibly reduced safety factor for impulse conduction has been documented by the threshold tracking technique and refractory period studies in nerves of AMAN patients, and one patient with AMCBN who progressed to axonal degeneration was reported.32–34 The above considerations explain why AMAN patients do not necessarily have a poor prognosis and may improve more rapidly or more slowly according to the relative proportion of axonal degeneration and reversible conduction failure, being the patients with AMAN with reversible conduction failure or AMCBN the ones with the best prognosis and complete recovery.30 35 36
An objection to the non-demyelinating nature of reversible conduction failure might come from the observation that CV was slow at the site of CB in some nerves of patients we finally diagnosed as axonal GBS with reversible conduction failure. In these patients, CV slowing was present from the first recording when CB was at a maximum, and CV rapidly increased with the decrease in CB and returned to normal range when CB had disappeared. Conduction slowing at CB sites may be a factitious phenomenon due to preferential block of large diameter fastest conducting fibres. The same explanation can be applied to the nerves showing prolonged DMLs which in sequential recordings quickly normalised in parallel with increased dCMAP amplitude. Alternatively, sodium channel dysfunction, which is hypothesised to be at the basis of reversible conduction failure, may be responsible for conduction slowing. In human poisoning by tetrodotoxin, slow CVs, increased DMLs and reduced dCMAP amplitudes recover in few days without temporal dispersion, possibly because of uniform involvement of all fibres in the nerve resulting in synchronous slowing of impulse conduction.37
Two patients were initially classified as AIDP because of progressive CMAP amplitude reduction along the nerve length, in some segments fulfilling the criterion for CB. At follow-up, the dCMAP amplitude decreased and equalised the proximal CMAP without the development of temporal dispersion. This pattern was named by van der Meché and colleagues ‘length-dependent CMAP amplitude reduction’ and initially thought to be due to demyelinating lesions scattered along the nerve followed by axonal degeneration.38 However, this pattern is also consistent with an immune-mediated primary axonal degeneration with progressive loss of excitability in fibres undergoing axonal degeneration.19 20 21 39 The dCMAP is initially greater than the pCMAP because the injured axons are unexcitable above the lesion site, whereas they remain excitable distally. The unexcitability progresses over a few days distally until it reaches the nerve terminals. Other possible explanations are that CB may be due to an axonal dysfunction, as in reversible conduction failure, which progresses to axonal degeneration or imputable to an adjunctive distal axonal involvement. In any case, the damage should be considered axonal in nature.
Because of the recognition of reversible conduction failure and length-dependent CMAP amplitude reduction patterns, a total of seven patients shifted from the AIDP and equivocal groups to axonal GBS and none from axonal GBS to AIDP. In the study by Hadden and colleagues, six of 10 patients initially classified in the axonal group were later reclassified as demyelinating, three were equivocal, and only one remained in the axonal group. Of the original demyelinating group, 4% become axonal and 5% unexcitable.4 This study was published in the same year of the paper on reversible conduction failure in axonal GBS and we think that, at least in part, the differences in results may be due to the lack of recognition of reversible conduction failure pattern.4 12
In the series, we report that antecedent C jejuni infection and antiganglioside antibodies are more frequent in axonal GBS than in AIDP. Overall 79% of axonal GBS but only 13% of AIDP had antecedent C jejuni infection and antiganglioside antibodies. These results confirm that the three conditions axonal GBS (including reversible conduction failure), antecedent C jeuni infection and IgG to gangliosides GM1, GD1a or GD1b are closely associated.5 Hiraga and colleagues advanced the hypothesis that antiganglioside antibodies are associated with axonal degeneration or reversible conduction failure but not to true AIDP.15 In our series, all patients who shifted to the axonal group had antiganglioside antibodies. However, 28% of patients finally classified as AIDP have antiganglioside antibodies. Reversible conduction failure is thought to be due to a transient attack of antibodies and complement limited at the excitable axolemma of Ranvier node, but it is conceivable that an immunological process, although specific, cannot have the ‘surgical’ precision to completely spare the paranodal region. As a matter of fact, detachment of terminal loops of paranodal myelin and lengthening of the nodal region have been shown in AMAN patients and in the experimental model.10 11 31 This feature, although the primary pathology is on the axonal side, mimics paranodal demyelination and may explain the ‘grey zone’ of patients with antiganglioside antibodies and some de-remyelinating features in electrophysiology fulfilling the criteria for AIDP.
This study demonstrates that in the early phase of GBS, the distinction between AIDP and axonal GBS may be difficult or even impossible in some patients. Theoretically, Ho's criteria including excessive temporal dispersion but not CB should avoid the pitfalls due to reversible conduction failure and length-dependent CMAP amplitude reduction resulting more specific than Hadden's criteria for AIDP. However, the fact that reversible conduction failure can also transiently slow CV and increase DML eliminates the advantage, making the two criteria substantially equivalent.
In conclusion, in GBS only serial electrophysiological studies allow the identification of pathophysiological mechanisms of muscle weakness and the correct classification in subtypes. More reliable electrophysiological criteria taking into consideration the reversible conduction failure pattern should be devised and validated in large populations.
References
Footnotes
Funding This study was supported by a grant from Ministero della Salute (Ricerca Corrente 2006).
Competing interests AU received research support from Kedrion and payement for lectures by Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary