Article Text

Abstract
There is substantial variability in the responsiveness of dystonia patients to deep brain stimulation (DBS), presumably due to the multiple causes of dystonia. This article presents the results of an analysis of the combined published results of individual patient outcomes following DBS for all types of dystonia. From 157 papers reporting clinical outcomes of DBS for dystonia, individual quantitative data were available for 466 patients with all forms of dystonia. The subclassification of these patients included 344 with primary forms of dystonia, 10 with myoclonus dystonia, 19 with heredodegenerative dystonias and 93 who had DBS for secondary dystonia. Patients with primary forms of dystonia, myoclonus dystonia, subtypes of heredo-degenerative dystonia and tardive dystonia have a greater than 50% mean improvement in dystonia severity following DBS. Among patients with primary generalised dystonia, multiple regression analysis showed that a shorter duration of symptoms (p=0.008), a lower baseline severity score (p=0.024) and DYT1 positive status (p=0.002) were all independently associated with a significantly higher percentage improvement from surgery. Patients with other forms of heredodegenerative and secondary dystonia have variable responses, making prediction of response in future patients difficult. The degree of dystonia response that justifies DBS is a highly subjective issue. Emphasis should be placed on both safety of surgical technique and an in-depth evaluation of patients' own perception of their life before and after DBS by using validated quality of life measures, in addition to existing use of objective severity scales.
- MeSH headings
- dystonia
- stereotaxic surgery
- systematic reviews
Statistics from Altmetric.com
Introduction
Dystonia is a common movement disorder, defined as ‘a syndrome of sustained muscle contraction usually producing twisting and repetitive movements or abnormal postures’. Classification of dystonia is made according to three main features; the age of onset of symptoms, the distribution of the region of the body affected (focal, segmental or generalised) and the underlying aetiology (primary, secondary, dystonia-plus conditions, or heredo-degenerative conditions). Patients with primary dystonia will present with no other neurological condition (with the exception of tremor) and will have no structural brain abnormalities or inborn errors of metabolism. About 10% of generalised dystonia starting in childhood or adolescence are linked to genetic mutations, the majority being caused by a GAG deletion in the DYT1 gene. Secondary dystonia results from other causes such as brain injury, drugs or toxins, or postencephalitis. Dystonia-plus conditions feature other neurological signs such as in the myoclonus–dystonia syndrome, but in these patients brain imaging is normal, no secondary cause is found, and genetic causes for these conditions have been identified. Dystonia is also seen in patients with a range of heredodegenerative conditions in which neurological symptoms and signs such as parkinsonism, ataxia, bulbar failure or neuropathy can provide clues to the underlying diagnosis.
Surgical treatment for dystonia dates from the 1950s to 1960s. Irving Cooper reported that 69% of 227 patients with dystonia improved with thalamotomy, with a marked improvement seen in 24% and mild to moderate improvement in 45%.1 Further teams subsequently demonstrated the benefit of lesioning the globus pallidus internus (GPi) for the treatment of dystonia,2 and subsequently deep brain stimulation (DBS) of the GPi was evaluated for the treatment of dystonia. The original reports of successful outcomes following DBS for dystonia included patients with the primary generalised form that were positive for the DYT1 GAG deletion.3 Since then, multiple centres have used DBS as a treatment for patients with many other subtypes of dystonia insufficiently helped by oral medications or Botulinum toxin injections. While mean results have generally been encouraging, a wide range of outcomes have been reported. Predictive factors of long-term outcome have been sought in small series with hints that shorter disease duration is a statistically significant predictor of better long-term outcome following DBS.4 Whether patients positive for the DYT1 deletion have a greater benefit has been unclear, with some reports suggesting that the DYT1 mutation is a predictor of better outcome,5–7 while others have not found a significant difference between the DYT1 positive or DYT1 negative groups.8 9 There is a lack of effective non-surgical treatment for patients with heredodegenerative and secondary dystonias, so DBS has been trialled among widely varying subtypes of such patients; however, the efficacy of DBS in the treatment of these patients is less clear.
In view of the substantial variability in the responsiveness of dystonia patients to DBS, we have reviewed the published literature and extracted the results of individual patient outcomes following DBS for dystonia. We have used these data in a metaregression to reanalyse factors predictive of outcome following DBS for all types of dystonia.
Methods
Search strategy
The PubMed database was searched for articles describing DBS for dystonia. MeSH headings used were ‘Dystonia’ and ‘Stimulation.’ Only articles written in English were reviewed, and only publications reporting individual clinical outcome data were included in statistical analyses. Papers that reported summary mean outcomes following DBS for dystonia are reported alongside the combined individual clinical outcome data. Where there were multiple serial publications from the same centre describing the same or overlapping patient groups, great care was taken to include data from any individual only once using their age at onset, age at surgery and baseline dystonia severity to distinguish them as individuals. Reports of patients with dystonia as a feature of Parkinson's disease were excluded. Dystonia subtypes were coded according to aetiology—primary, dystonia plus, heredodegenerative or secondary—then by subtype according to body distribution and or identified underlying cause.
Assessing the outcome of DBS for dystonia
The scale most commonly used for rating severity of generalised dystonia is the Burke–Fahn–Marsden Dystonia Rating Scale. This comprises a clinician-rated movement scale (120 point score) and patient-rated disability scale (0–30 point score). For patients with cervical dystonia (an adult-onset focal primary dystonia) the Toronto Western Spasmodic Torticollis Rating Scale is most commonly used with subscores for severity, disability and pain. While most studies have used the Burke–Fahn–Marsden Dystonia Rating Scale and Toronto Western Spasmodic Torticollis Rating Scale for measuring outcome, the Unified Dystonia Rating Scale, the Abnormal Involuntary Movement Scale, and the Tsui Scale have also been utilised.
Statistical analysis
From each paper documenting individual outcome data, the following information was noted: the dystonia subtype, gender, age at surgery, duration of symptoms, rating scale used, DBS target, preoperative and postoperative scores, duration of follow-up and whether assessment was open or blinded. The percentage improvement in dystonia severity was calculated for each patient. Microsoft Stata version 8 was used for all analyses (Microsoft, Seattle, Washington). Multiple regression was performed to assess whether percentage improvement in dystonia severity was associated with age at surgery, duration of symptoms, baseline severity and surgical target. The centre, the duration of follow-up, the rating scale used and whether the assessment was performed open or blinded were included as covariates in each model.
Results
The original Pubmed search revealed 1010 papers, of which 157 papers reported clinical outcomes of DBS for dystonia. From these papers, individual quantitative outcomes following DBS were available for 466 patients with all forms of dystonia. The subclassification of these patients included 344 with primary forms of dystonia, 10 with myoclonus dystonia, 19 with heredo-degenerative dystonias and 93 patients who have had DBS for secondary dystonia. The number of patients in each subcategory together with the references from which the patient data were obtained are presented in tables 1–3.
Published individual outcome data on patients with primary forms of dystonia (and myoclonus dystonia) operated on with deep brain stimulation
Published individual outcome data on patients with heredodegenerative forms of dystonia operated on with deep brain stimulation
Published individual outcome data of patients with secondary forms of dystonia operated on with deep brain stimulation
Primary dystonia
Primary generalised dystonia (PGD)
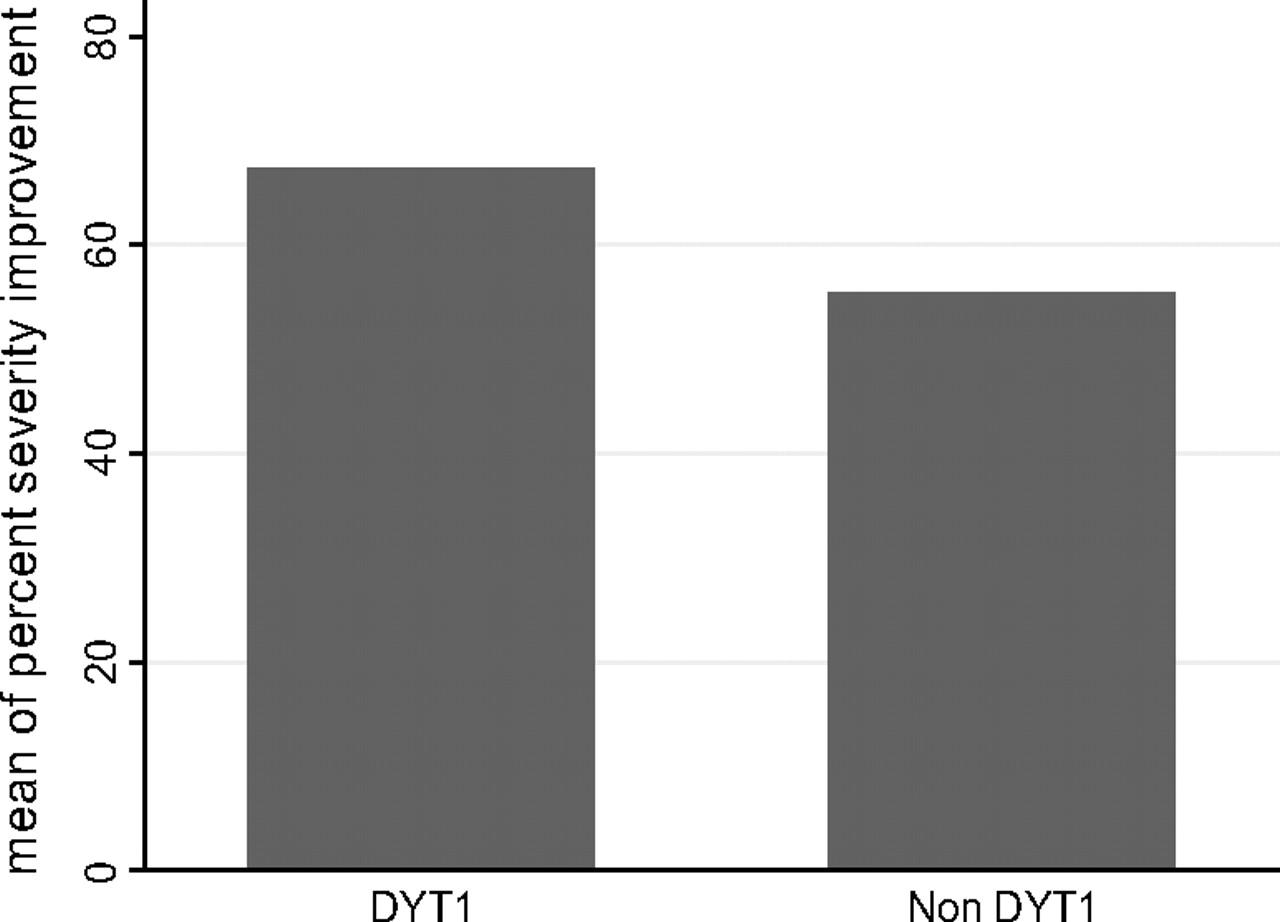
The search identified 209 patients who received DBS for primary generalised dystonia from 20 centres. The baseline features of these patients are presented in table 1. The mean percentage improvement of the group as a whole was 60.7%, (IQR −43.4% to 83.3%). Within this group, the 91 patients with DYT1 positive dystonia had the greatest percentage improvement. Multiple regression analysis (with adjustment for confounding covariates) showed that a shorter duration of symptoms (p=0.008) (see also figure 1), a lower baseline severity score (p=0.024) and DYT-1 positive status (p=0.002) (see also figure 2) were all independently associated with a significantly higher percentage improvement from surgery. In a single patient who had DBS of the subthalamic nucleus (STN) for idiopathic PGD, an overall improvement of 72.1% was observed.10

Graph to show the univariate relationship between duration of symptoms of dystonia and percentage improvement from deep brain stimulation among patients with primary generalised dystonia together with regression line (β coefficient=−0.48, CI −0.82 to −0.16). In our multivariate analysis of patients with primary generalised dystonia, 13% of the variance in outcome was predicted by duration of symptoms, DYT1 status and baseline severity alone.

{kind=link}
{kind=link}
Mean percentage improvement following deep brain stimulation for primary generalised dystonia patients with/without DYT1 mutation.
Additional patients have been published in other series but could not be included in the current analysis because of a lack of individual data in the published manuscripts. Among 24 patients with generalised dystonia that received GPi DBS in a double-blinded trial of DBS (the only double blind trial of DBS for primary generalised dystonia), there was a 41.9% mean reduction in dystonia severity.8 A further series of 30 patients followed up for 2 years had a mean reduction in motor severity of 82.5%.11 These authors demonstrated that the presence of fixed skeletal deformities and longer disease duration were both predictive of a lower percentage improvement following GPi DBS. A series of 24 primary generalised dystonia cases improved by a mean of 59% if DYT1 positive, and only 43% if DYT1 negative, but this difference was not significant.12
Spasmodic torticollis
Individual outcome data were identified for 67 patients from 14 centres with isolated spasmodic torticollis treated with DBS. The mean improvement was 48% (SD 41%), but none of the variables entered into the regression model were associated with the magnitude of improvement from surgery. Sixty-three patients had electrodes inserted in the GPi with a mean percentage improvement of 49.2%, whereas four patients had electrodes in the STN with an improvement of only 34.9%.10 Patients evaluated in a blinded fashion had a mean improvement of 33.3% compared with a mean improvement of 52.3% in those patients assessed in an open label fashion.
Meige syndrome
All 17 patients included in this analysis had GPi DBS, with a mean improvement of 64.3% (SD 29.5%). Compared with other patients with focal/segmental dystonias, the patients with Meige syndrome were older, with a shorter duration of symptoms and a higher percentage response to treatment. The regression analysis confirmed that the only variable showing a trend towards association with improved percentage outcome from DBS was a shorter duration of symptoms (p=0.06).
Focal/segmental dystonias
This subgroup of dystonia patients includes a mixture of phenotypes. The majority of published patients have not been tested for DYT-1 status. Patients had a mean improvement of 57.9% with the GPi target (n=37), all with open label assessments. A single patient receiving STN DBS for this condition had a 23% improvement in symptoms,13 whereas a single report of ViM DBS had a 58.3% improvement.14 An additional 16 patients with focal/segmental dystonia had GPi DBS as part of a blinded trial and showed a mean 52.6% reduction in dystonia severity but without individual data.8 None of the variables entered into the regression model predicted the magnitude of improvement from surgery for patients with focal/segmental phenotypes.
Myoclonus dystonia
From 10 patients with myoclonus dystonia, a mean improvement of 58% was seen following GPi DBS (table 1). Two case reports of VIM DBS for myoclonus–dystonia suggested improvement in myoclonus but not dystonia.15 16
Heredodegenerative dystonias
Patients with pantothenate kinase-associated neurodegeneration had the greatest percentage improvement of the heredodegenerative subcategory, all operated on in the GPi (table 2). The percentage response was not associated with age at surgery, duration of symptoms or baseline severity. Some individuals with neuroacanthocytosis manifest both dystonia and chorea. Reports of GPi DBS in this condition suggest that dystonia may be improved, but this may be at the expense of worsening of chorea.17
Secondary dystonia conditions
The number of patients with each secondary dystonia subtype is small (table 3). Patients with tardive dystonia (n=41) had a 69% improvement in dystonia severity following DBS. A lower preoperative score (p=0.04) and shorter duration of symptoms (p=0.02) both independently predicted improved percentage response. The 39 patients who had GPi DBS improved by 67.4% in comparison with two patients who had STN DBS improving by 92%.18
Patients with post-traumatic dystonia, dystonic cerebral palsy or postencephalitic dystonia respond less well to DBS with only isolated rare exceptions.19 20 The small number of patients with postanoxic dystonia have a higher mean percentage improvement, but the variance in response is higher and is not related to age, duration of symptoms or baseline severity.
Quality of life
The vast majority of studies measure the change in one of the validated dystonia severity scales to gauge outcome following DBS for dystonia. These scales are objective, but the resulting scores do not necessarily reflect the patient's subjective perception of changes in their daily life or their quality of life (QoL). For example, a minor improvement in neck posture, hardly detectable on the BFM movement subscale, may nevertheless have major importance in wheelchair comfort or in swallowing, and indeed the converse can also apply. An alternative is therefore to measure QoL which has been incorporated into several of the larger dystonia series.
Among 22 patients with primary generalised dystonia, significant improvements in general health, physical function and body pain were identified using the generic short form 36 (SF-36) scale. The mean scores did not deteriorate in any SF-36 domain, and measures of cognition and mood were unchanged.9 In the double-blind trial of DBS for 40 patients with segmental or generalised dystonia, there was a significant improvement in the SF-36 physical composite score at 3 months.21
Adverse effects of DBS surgery for dystonia
Not all published reports specifically document detailed adverse effects resulting from DBS for dystonia, so no attempt to quantify their overall frequency is made here. There are multiple reports of lead migration and lead fracture,4 5 8 22–26 and one group have proposed that this complication is more common among dystonia patients than other patients undergoing DBS.27 Other surgical adverse events do not seem to occur particularly more commonly in dystonia with only occasional reports of haemorrhage,26 infection4 8 13 22 28–33 and misplaced electrodes.26 34 Adverse effects specifically related to chronic GPi stimulation for dystonia include dysarthria25 30 33 35–37 and parkinsonism,7 38–40 both of which seem to be reversible but sometimes at the expense of inadequate dystonia relief.
Discussion
This review has drawn together the published data describing the outcomes of DBS for the range of subtypes of dystonia, and presents the overall results of the combined dataset. The most impressive and consistent results are among patients with DYT-1 primary generalised dystonia and patients with tardive dystonia. Because of the fairly recent introduction of DBS for dystonia, there is a lack of long-term follow-up, although four recent studies have reported on outcome at up to 7.5 and 10 years post-DBS implantation4 23 41 42 concluding that DBS can maintain a significant long-term benefit in responding patients.
Inevitably there are potential sources of bias in this type of review. Positive results from surgery are more likely to be reported than negative outcomes, and the vast majority of studies present data from open label assessments that are more likely subject to observer bias. Only two studies included in this review had blinded assessments of their patients (spasmodic torticollis19 34 and secondary dystonia19). Indeed, the quantitative outcomes following DBS for dystonia are considerably lower when patients are assessed in a blinded fashion. Despite these potential shortcomings, the data presented here represent the most comprehensive review of dystonia outcomes following DBS to date. DBS has been beneficial to the majority of dystonia patients highlighted in the literature, although the percentage improvement rate is very variable.
Primary generalised dystonia
This dataset confirms that patients with PGD respond well to pallidal DBS. Patients with DYT1 positive dystonia respond better than those that are DYT1 negative or untested, although all PGD groups respond well overall, but with considerable interindividual variability. Independent of DYT1 status, surgery performed at a younger age and with lower baseline severity is more likely to lead to a higher percentage improvement in symptoms of dystonia. While this trend is a useful guide, individual patients can confound this general trend—for example, a PGD patient experiencing only a 20% improvement in BFM despite a disease duration of only 5 years, and another patient with an 85% improvement despite a disease duration of 21 years.5
Analysis of further additional factors that might predict response to DBS was possible in a retrospective review of 40 PGD patients (included in this analysis) operated on in Montpellier, France with a 2–8-year follow-up. These authors created a multivariate model to evaluate which factors predicted response to DBS in PGD41 and, in addition to their data consistent with that presented here, found that increased anatomical and stimulated volumes of the GPi also predicted better outcomes. Several groups have attempted to look specifically at active electrode position within the GPi and relate this to outcome. Postero-ventral GPi stimulation has been found to provide the greatest overall effect, and has been considered superior for the arm and trunk.7 However, other series have found no correlation between active contact positions and postoperative outcome.9 The optimal programming parameters vary widely between patients and the interactions between the position of electrode contacts, pulse widths and mode of stimulation make comparisons difficult, although it has to be assumed that the optimal parameters have been chosen through an iterative process for each patient.
A further evaluation of factors predicting outcome following DBS for primary generalised dystonia was also performed as part of a 3-year study9 that followed up 22 patients (included in this analysis), and demonstrated sustained benefit from the pallidal stimulation (58% mean improvement from baseline). Their patients who had little improvement tended to have severe tonic posturing, whereas the patients with the greatest improvements (>75%) had diffuse phasic hyperkinetic involuntary movements preoperatively. In addition, most groups have found that those patients with fixed skeletal deformities do less well than those patients caught earlier in their disease progression, although they may still improve from their baseline state and therefore benefit from treatment. In addition to fixed skeletal deformities, the development of secondary disability from cervical myelopathy, for example, further limits possible improvements.43
Spasmodic torticollis
The most common of the adult-onset, focal primary dystonias is spasmodic torticollis. The sternocleidomastoid muscles are innervated from both hemispheres with most of their supply coming ipsilaterally; therefore, bilateral surgery is required even for the most asymmetrical patients. The variance in response, however, is substantial and does not appear to be explained by age at surgery, duration of symptoms or baseline severity. Even at the same centre, a range of improvement between 20 and 83% has been seen,30 despite postoperative MRI confirming electrode positions, and no correlation was found between location of electrode and magnitude of response.
Dystonia severity should not be the only measure of outcome following DBS. Among a single blind series,34 even patients with less than 30% improvement on motor score all improved in relation to their pain, disability and QoL. This study also investigated outcome predictors such as electrode location, surgical centre, surgical technique or type of dystonia (phasic, tonic or tremulous), but none appeared related. The only patient who deteriorated after DBS had good electrode placement.
Meige
The current analysis confirms the findings of case reports suggesting that GPi DBS is a useful therapy for patients with Meige syndrome (idiopathic cranial cervical dystonia).44–46 In a series of patients with Meige syndrome that followed six patients for 6 months, most patients had meaningful clinical improvements by 4 to 6 weeks' postimplantation. Overall improvements were seen in blepharospasm, oromandibular dystonia and cervical dystonia. Speech and swallowing both showed a trend towards improvement.38
Myoclonus dystonia
Although the number of published patients with myoclonus dystonia that have had DBS is small, the reports of good outcomes among these patients are consistent with our own experience. Both myoclonic features and dystonia can improve.
Heredodegenerative dystonia
Patients with heredodegenerative dystonia are distinct from other individuals with dystonia by the coexistence of other neurological deficits—for example, cognitive decline, seizures, etc. There is no evidence that non-motor symptoms or the degenerative process itself are improved by DBS. However, improvement in pain as a result of DBS can allow lower medication doses, which can have secondary beneficial effects.47 Among these patients, a vital prerequisite in the decision regarding surgery is the identification of the degree of disability that they suffer purely due to dystonia.
Secondary dystonia
The experience of GPi DBS in secondary dystonia has been limited, varied and less successful than in the idiopathic group. Conceptually it might be considered that patients with normal brain MRI have a reversible electro-physiological or neurochemical cause for their dystonia, whereas patients with abnormalities visible on conventional structural imaging may have an irreversible anatomical cause for their dystonia. The excellent response of patients with tardive dystonia is consistent with this. This concept is of course too simplistic in view of the diverse structural abnormalities in basal ganglia pathways that can all be associated with onset of dystonia added to the fact that the creation of lesions within basal ganglia structures can lead to resolution of dystonia.6
DBS of targets other than GPi
Thalamus
Thalamic DBS in dystonia, targeting various nuclei of the ventrolateral (VL) motor thalamus (Vim, ventral oral posterior (Vop), ventral oral anterior (Voa)), was tried initially as a treatment for dystonia based on the improvements in a minority of patients seen after thalamotomy. There has been no randomised comparison of GPi DBS versus thalamic DBS for dystonia, but the majority of centres have adopted the GPi target based on consensus experience. Among 12 patients who had thalamic DBS for a mixture of dystonia subtypes, three subsequently went on to have successful responses to GPi DBS because of insufficient benefit with thalamic DBS.44
Our view is that DBS of the VL thalamus should be restricted to those patients with marked tremor causing greater disability than dystonia, or in those patients with structural abnormality of the GPi (although the expectation of success in this group is lower).
Subthalamic nucleus
There is some experience of the STN as a target for dystonia patients, especially in patients with damage to the GPi. Unilateral STN DBS in a patient with left hemidystonia secondary to a basal ganglia infarct led to an improvement by 54.5% at 3 months.48 Improvements in tardive and post-traumatic hemidystonia have also been reported following STN DBS, while six patients with other forms of secondary dystonia had minimal improvements.49 The STN is still a novel target for DBS in dystonia patients, so further studies will be needed to assess efficacy.
Conclusions
DBS has been shown to be a safe, effective surgical treatment for medically refractory dystonia, with the postero-ventral sensorimotor GPi being the most favoured target site. Patients with primary forms of dystonia and tardive dystonia respond well, particularly so when the surgery is performed at an earlier stage and among patients with lesser disability. Patients with DYT-1 positive dystonia respond better than DYT-1 negative cases, although the DYT-1 negative group remains very heterogeneous. Patients with other forms of heredodegenerative and secondary dystonia have variable responses, making prediction of response in future patients difficult.
Differences in methodological approach, surgical technique, programming regimes and clinical presentation make determining outcome predictors in these subgroups even more challenging. A systematic and thorough approach to reporting all patient and technical variables needs to be implemented so that useful conclusions can be reached with accumulating reports. Additionally, emphasis should be put on in-depth evaluation of patients' own perception of their life following DBS by using validated QoL measures possibly including a qualitative approach.
Discussion with patients and their carers requires an honest explanation of the uncertainty of the usefulness of DBS, in particular for patients with heredodegenerative and secondary dystonia subtypes. There is undoubtedly a placebo response and/or a clinician bias in evaluation following DBS, as evidenced by the excess benefits documented in open-label follow-up compared with blinded trials. The safety record of the centre should be an important factor which determines how much a potential improvement may justify the small surgical risks, especially as patients with dystonia frequently do not have alternative treatment options.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
Supplementary materials
Lay Summary 81/12/1383
Files in this Data Supplement:
Footnotes
Funding Parkinson's Appeal.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.