Article Text

Statistics from Altmetric.com
Neurologists should not be surprised if the cause of a disorder is remote from its effect, such as a parasagittal meningioma causing foot dragging, or a sacral ependymoma leading to deafness as the first sign of siderosis of the nervous system. Yet we were for some time bewildered by the following problem.
{kind=link}
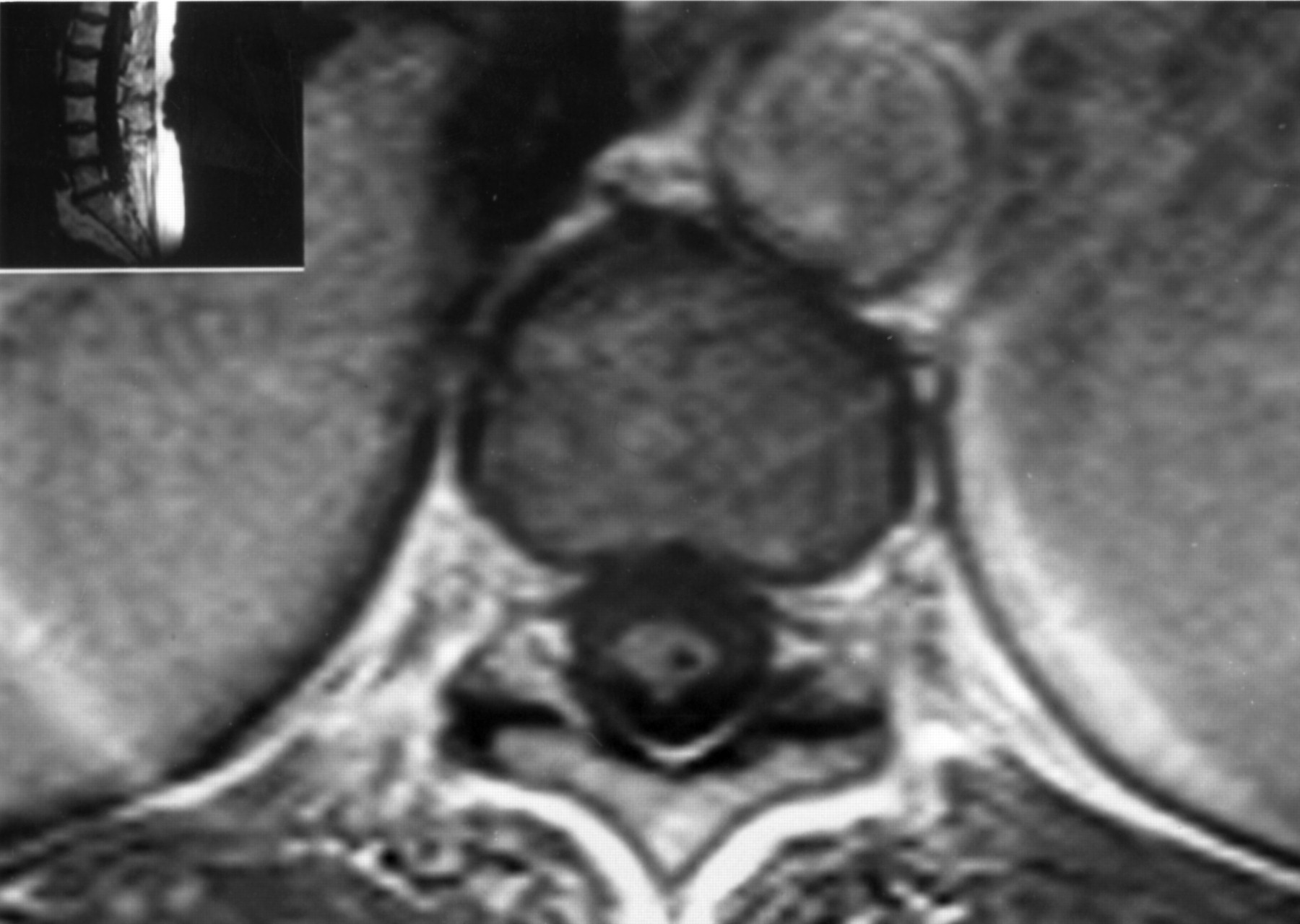
T1 weighted MRI at the level of the D10-D11 intervertebral disc. Hypointense lesion in the left dorsolateral region of the lumbar cord, corresponding to the posterior horn.
A 67 year old woman consulted us in 1996 for attacks of pain in the left leg that had started in 1978 and had gradually increased in severity and frequency up to three to four attacks an hour, each lasting a few minutes and so severe that she had to stop anything she was doing to nurse her pain. It was sharp and stabbing in character and radiated from the gluteal region to the groin, and further down to the lateral part of the upper and lower leg. Between attacks she was completely free of pain. The stabs also woke her up at night, six or seven times. In 1988 investigations at another hospital had established the diagnosis of cervical syringomyelia, secondary to tonsillar ectopia (Chiari I malformation); a year later a syringopleural drain was inserted. Subsequently the syrinx collapsed, but the attacks of pain continued unabated. Examination (in 1996) showed normal power and sensation in the arms, a thoracic kyphosis, and on the left side of the trunk a suspended level of hypaesthesia and hypalgesia, extending from just under the nipple down to the left leg, as far as 10 cm below the knee; vibration sense was abolished below the sternum on both sides. Power in the legs was normal; the tendon jerks were very brisk on the right and sluggish on the left, both plantar responses flexor. Repeated MRI studies confirmed a collapsed syrinx in the cervical region, extending throughout the thoracic cord, and deviating to the left at the level of the lumbar cord (figure). Many analgesic, antidepressive, antiepileptic, and antiarrhythmic drugs had previously failed or failed again in our hands, as did sympathetic blockade or transcutaneous electrostimulation. Implantation of an epidural stimulator gave considerable relief, the intensity of the pain decreasing by more than half; this was sustained up to the last contact, nine months after implantation.
Leg pain with syringomyelia has so far been reported only in patients with a syrinx confined to the lumbosacral cord, secondary to trauma or tumour.1 2 In our patient bouts of pain in the leg were associated with classic syringomyelia, which starts at the level of the cervical cord and results from obstruction of the CSF flow at the foramen magnum, most commonly by tonsillar ectopia.3 4 We propose that the pain resulted from disturbed impulse transmission in the posterior grey matter at the left side of the lumbar cord, the pain partially matching the area of sensory loss. It is not unusual for symptoms to correspond to paracentral cavitations only, the central part of the syrinx being clinically silent.5 Dysaesthetic pain from a paracentral syrinx is known to occur in the arm.6 Also in those cases the response to surgical treatment is unpredictable.6 Epidural stimulation was the only measure that made our patient’s life again bearable.
Acknowledgments
We are grateful to Dr HE van der Aa ( Enschede) for referring the patient and to AL Liem (St Antonius hospital, Nieuwegein) for implantation of the epidural stimulation device.