Article Text

Statistics from Altmetric.com
{kind=link}
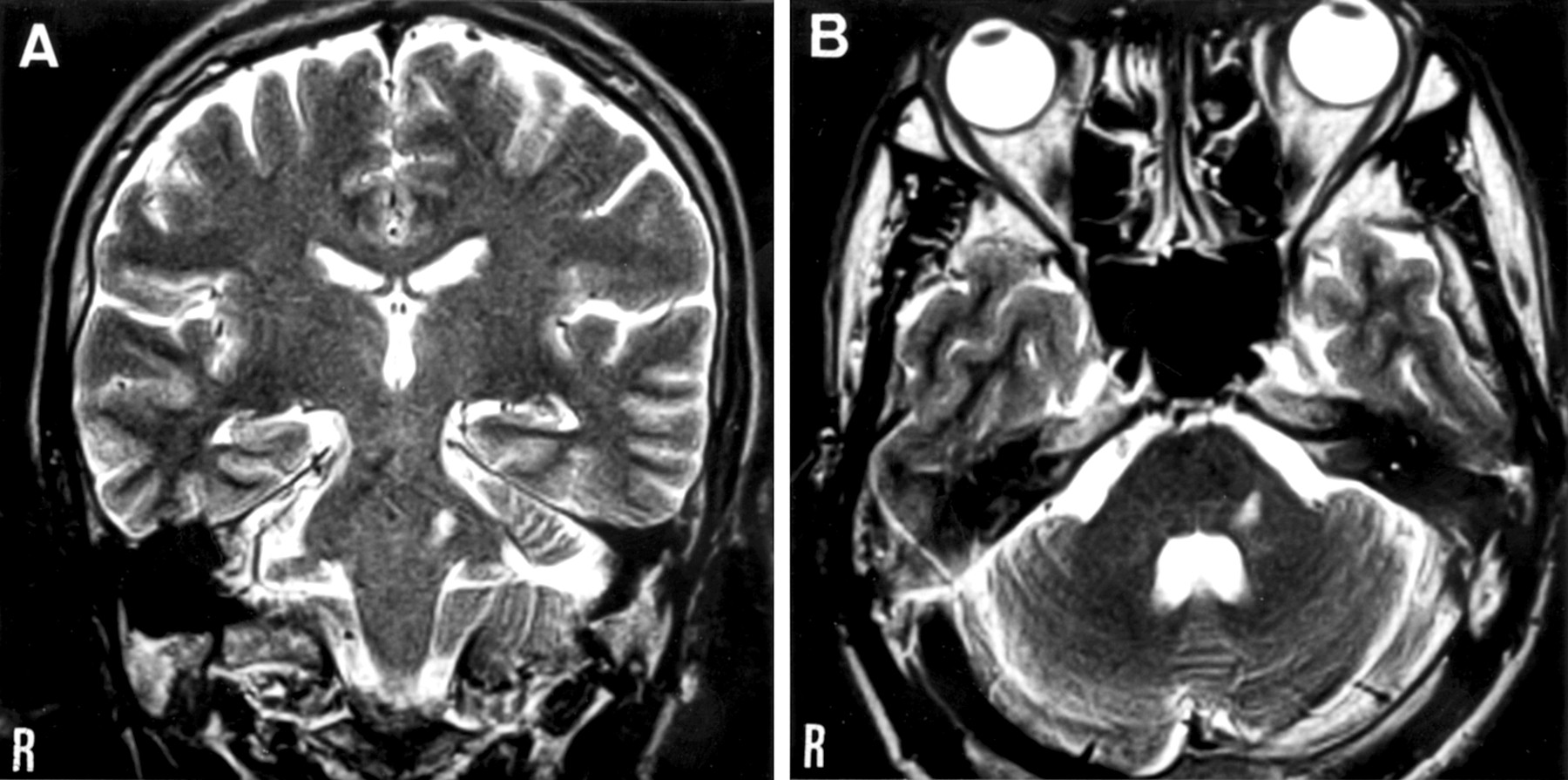
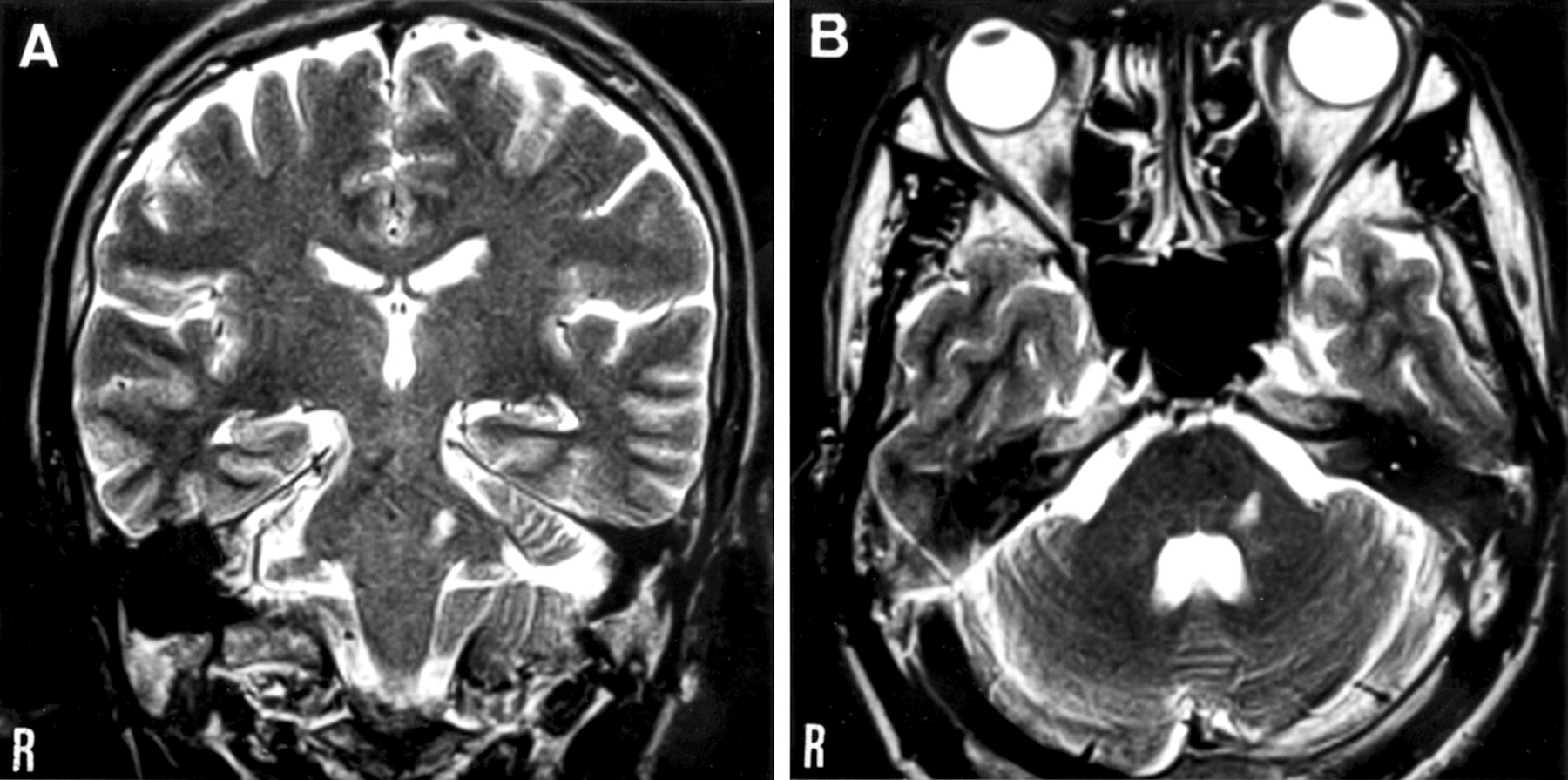
Small infarction in the left dorsolateral pontine tegmentum was identified by MRI in a 41 year old man presenting with isolated orofacial sensory deficits in the absence of other neurological findings.
Isolated trigeminal sensory neuropathy resulting from brain stem vascular lesions, either haemorrhagic1 or ischaemic,2 3 has been extremely rarely reported.
Our patient awoke to find numbness and paraesthesia over the left upper face, tongue, and buccal mucosa. Neurological examination disclosed non-dissociated sensory deficits on the same region. The corneal responsiveness was normal, and no hypotonus and weakness of the masseter muscle was detected. These findings implicated exclusive involvement of the pontine trigeminal sensory complex, including the principal sensory nucleus and pars oralis of the spinal trigeminal nucleus and tract.
The figure shows (A) the coronal and (B) the axial T2 weighted images, with a hypointense lesion in the left dorsolateral pontine tegmentum a few days after the onset.