Article Text

Statistics from Altmetric.com
Head-up tilt table testing had been used as an investigative tool in the pathophysiology of orthostatic stress for more than 50 years,1 before the initial demonstration of its utility in the diagnosis of unexplained syncope.2 The Westminster group's landmark study found that 67% of patients with otherwise unexplained syncope demonstrated a vasovagal reaction during head-up tilt, compared to only 10% of healthy controls.2 Head-up tilt table testing has since evolved into the diagnostic test of choice in vasovagal syncope and related disorders, but there are still wide variations in the protocols used in various centres, hampering not only the clinical utility of the test but the adequate assessment of research activity in the field. The following protocols are based on the available evidence and our experience in this field and, as such, provide a practical and standardised approach. They are intended for use by cardiologists and other physicians with an interest in this topic, and hence assume some prior knowledge of the procedure. A more detailed description and justification for the protocols is readily available.3 ,4
Indications for head-up tilt table testing
Head-up tilt table testing should be considered in patients with recurrent syncope or presyncope, or in high risk patients with a history of a single syncopal episode (for example, those suffering serious injury during syncope or those experiencing syncope while driving) where no other cause for symptoms is suggested by initial history, examination or cardiovascular and neurological investigations. Tilt table testing may also be useful in the assessment of elderly patients with recurrent, unexplained falls.5 The head-up tilt table test may also have a role in the differential diagnosis of convulsive syncope,5-7 orthostatic hypotension,8 the postural orthostatic tachycardia syndrome,9 psychogenic10 and hyperventilation11 ,12 syncope, and carotid sinus hypersensitivity.13-15 The Newcastle protocol for carotid sinus massage is detailed later in this article.
Contraindications to head-up tilt table testing
Head-up tilt table testing is safe with few reported adverse events.4 ,16 While there are no reported deaths during tilt testing in the world literature, we are aware of some anecdotal reports of fatal outcome during tilt testing, and caution should be applied as follows: relative contraindications include clinically severe left ventricular outflow obstruction, critical mitral stenosis, and patients in whom low organ perfusion pressures may compromise end artery supplied tissue, as in severe proximal coronary artery and cerebrovascular stenosis. Where such pathology is suspected, caution should be exercised regarding the duration and degree of hypotension allowed during tilt testing. Contraindications to isoprenaline provoked tilt table testing are discussed in the appropriate section.
Head-up tilt table test methodology
The conditions under which the head-up tilt test are carried out critically influence outcome, hence these will be examined in detail.
PATIENT PREPARATION
Patients, in particular those over 60 years old, should be fasted for no more than two hours before the procedure in order to avoid the confounding effects of relative dehydration and hypotension.4 ,17 The procedure should be explained to the patient who should rest supine for 20–45 minutes.18-20 A longer period is particularly important if intravascular instrumentation is required.19 ,21 Where practicable, drugs affecting the cardiovascular and autonomic nervous systems and those likely to affect intravascular volume should be discontinued for at least five half lives before the test17 unless they are implicated as an attributable cause of syncope, in which case testing should be done on medications. While in the head-up tilt position, the patient should be instructed to avoid movement of the lower limb musculature and joints in order to maximise venous pooling.4 ,17
EQUIPMENT, MONITORING, AND ENVIRONMENT
The tilt table should be of the foot plate support type. Whether mechanically or electrically powered, it should allow rapid achievement of the upright posture and allow calibrated tilt angles of between 60° and 80°; rapid and smooth resumption of the supine position should be easily achievable. Electrocardiographic monitoring should occur continuously during symptoms or haemodynamic changes and every minute otherwise. Blood pressure monitoring should be of the continuous, non-invasive, beat-to-beat variety (for example, digital photoplethysmography, Finapres, Ohmeda, Wisconsin (fig 1), or Portapres, TNO Biomedical, Amsterdam), since sphygmomanometric measures are insensitive to rapid changes in blood pressure. The newly published classification of the haemodynamics of vasovagal syncope by Brignole and colleagues,22 which has important implications for both clinical practice and research, is dependent on continuous and detailed blood pressure monitoring, making beat-to-beat assessment essential, though sphygmomanometric measures continue to be used. The Portapres device has the added advantage of derived measures of stroke volume, cardiac output, total peripheral resistance, etc, but is unfortunately rather more costly, while Finapres is no longer in production. Routine intra-arterial blood pressure monitoring is not advised. Blood pressure should similarly be recorded continuously (or as frequently as is practicable) during symptoms and at one minute intervals otherwise. In order to minimise stimuli affecting autonomic nervous function, the test should occur in a quiet, dimly lit room at a comfortable temperature. Advanced resuscitation equipment should be immediately available and to the standard required in exercise tolerance testing facilities.4 The test should be continuously supervised by a physician, nurse or technician experienced in the management of the test and its potential complications. If not directly supervised by such, a physician experienced in advanced cardiac life support should be immediately available at all times.

Continuous digital photoplethysmography (Finapres, Ohmeda)
TILT TABLE ANGLE AND DURATION OF THE HEAD-UP TILT TABLE TEST
Tilt table angle and the duration of the tilt test are crucial determinants of its positivity, sensitivity, and specificity.4 ,23 ,24 Tilt angles of between 60° and 80° are optimal in provoking sufficient orthostatic stress without increasing the incidence of false positive results4 ,20 ,24 and are recommended by most authorities.4 ,5 ,24 Our own practice utilises a 70° angle for head-up tilt table testing.19 ,25
Duration of the drug free, passive tilt test has been reported from 10–60 minutes by various centres.5 ,19 ,20 ,24-32 There are little hard data available on the relative merits of different drug free, passive tilt test periods, though most recent reports favour prolonged passive head-up tilt (30–45 minutes).4 ,19 ,20Fitzpatrick and colleagues noted a significant increase in the number of false negative results with shorter tilt periods.20 The mean time to syncope in their patients was 24 minutes20; assuming a normal distribution plus two standard deviations, a duration approaching 45 minutes would be optimal at present,4 ,24and our own practice is to continue the tilt test for 40 minutes or until symptoms supervene.
Newcastle protocols overview
The Newcastle protocols for head-up tilt testing in the diagnosis of vasovagal syncope are summarised in table 1. Patient preparation, environment, and monitoring should proceed as described above. Termination of the test should occur immediately positivity criteria are achieved, or if patient discomfort, significant arrhythmia or other adverse event develops. Blood pressure is recorded at one minute intervals, with ECG recordings made at one minute intervals or continuously during symptoms or haemodynamic derangements. Intravenous cannulation is avoided in all but the isoprenaline protocols to preclude its adverse effects on specificity.19 ,21
Summary of Newcastle protocols for head-up tilt table testing
DRUG FREE PASSIVE HEAD-UP TILT
The patient is rested supine for 20 minutes before the test, then tilted upright for 40 minutes at an angle of 70°.
PHARMACOLOGICAL PROVOCATION HEAD-UP TILT TESTING
Isoprenaline head-up tilt test
The patient remains supine for 20 minutes, and is then tilted to 70° for five minutes. The supine position is again assumed for five minutes' re-equilibration. Isoprenaline is then infused at a rate of 1 μg/min for five minutes supine, then five minutes at 70° tilt. The infusion is discontinued for two minutes during which the patient remains supine. Isoprenaline is then recommenced at 3 μg/min for five minutes supine and five minutes at 70°. Higher doses of isoprenaline should not be used because of adverse effects on specificity.23 ,33 ,34 Contraindications include ischaemic heart disease, uncontrolled hypertension, left ventricular outflow obstruction, and significant aortic stenosis, while caution should be used in patients with known dysrhythmias. The infusion should be discontinued if heart rate exceeds 150 beats per minute (bpm), blood pressure exceeds 180/100 mm Hg or if arrhythmia, chest pain, severe tremulousness, vomiting or other intolerable side effects supervene. Side effects are particularly prominent in elderly subjects.35 In the face of a strong clinical history and an initial non-diagnostic passive tilt, glyceryl trinitrate (GTN) tilt, which is better tolerated and has equal specificity in this age group, should be used in preference.25 ,35
Glyceryl trinitrate head-up tilt test
The patient is rested supine as above, and two metred doses (400–800 μg) of sublingual GTN spray are administered. Two metred doses are given to ensure an effective dose to counter the effects of GTN's linear pharmacokinetic profile and variable absorption.36 The patient remains supine for a further five minutes and is then tilted to 70° for 20 minutes.25Others have reported adequate positivity and specificity with continuous 60° tilting for 45 minutes with the administration of 400 μg nitroglycerin at 20 minutes if syncope had not occurred,26 though this is not currently our practice.
LOWER BODY NEGATIVE PRESSURE
The patient should remain supine for 20 minutes and then tilted at 70° for 20 minutes. If symptomatic hypotension/bradycardia does not supervene, lower body negative pressure using a suction chamber surrounding a standard tilt table should be applied at 20 mm Hg at the 70° angle for 10 minutes (fig 2).42 Suction may be increased to 40 mm Hg for 10 minutes, though this may increase the rate of false positivity.

Lower body negative pressure chamber tilt testing
Positivity criteria
The head-up tilt table test is judged positive if syncopal or pre-syncopal symptoms reproducing the patient's original symptoms are accompanied by hypotension, bradycardia (relative or otherwise) or both. Heart rate and blood pressure changes in isolation should not prompt a diagnosis of vasovagal syncope.
Head-up tilt table testing in paediatric patients
Children as young as 3 years have successfully undergone tilt table testing.43 Indications, contraindications, and methodology are essentially the same as in adults,44-47with the proviso that isoprenaline dosage should not exceed 0.03 μg/kg/min where it is indicated.43 Sensitivities and specificities for both drug free passive tilt and isoprenaline provoked tilt are similar to those reported in adults,47though to our knowledge there is not yet any data on the merits of GTN provoked tilt testing in this population.
Head-up tilt table testing in the elderly
Few studies have addressed the issue of tilt testing specifically in the elderly, but those reported to date suggest that there should be no differences in tilting methodology.19 ,25 ,48-50 The main difference in older subjects lies in the more variable presenting symptoms seen in this group. Elderly patients with vasovagal syncope frequently have sudden onset of syncope with little or no prodrome, hence tilt test positivity criteria need to be viewed in this light.49 ,50
Heart rate variability during head-up tilt table testing
The role of heart rate variability in the analysis of autonomic function is well established, but its relevance in the assessment and prediction of the physiologic and pathophysiologic responses to head-up tilt table testing is uncertain. Its utility as a research tool is evident, but its role in the diagnosis and management of the vasovagal syndrome remains unclear.
Non-vasovagal syncope related diagnostic uses of the head-up tilt table
DIFFERENTIAL DIAGNOSIS OF CONVULSIVE SYNCOPE
Short lived tonic–clonic movements and myoclonic jerks are a not infrequent accompaniment of vasovagal syncope, particularly during prolonged asystole,5 and their presence may prompt a misdiagnosis of epilepsy,5 ,6 often labelled as refractory.7 Rapid recovery, the short duration of the episode, and the absence of postictal signs and symptoms suggest a vasovagal diagnosis, which can only be made with a high index of suspicion and appropriate tilt testing, particularly with concurrent electroencephalography.5-7
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME
Postural tachycardia in association with relatively mild hypotension has been recently described and diagnosed with the aid of the head-up tilt position, and is thought to represent a mild form of autonomic dysfunction rather than a variant of vasovagal syncope.9 The syndrome is diagnosed on the basis of a heart rate increase of > 30 bpm (or a maximum heart rate of 120 bpm) in the absence of profound hypotension but reproducing symptoms,9 which can include light headedness, fatigue, presyncope, and dizziness.
ORTHOSTATIC HYPOTENSION
Orthostatic hypotension has traditionally been diagnosed on the basis of a fall in blood pressure during active standing. This definition was recently expanded by the American Autonomic Society and the American Academy of Neurology to include a fall in systolic blood pressure of > 20 mm Hg or diastolic blood pressure of > 10 mm Hg using a tilt table in the head-up position within three minutes and at an angle of 60°.8
PSYCHOGENIC AND HYPERVENTILATION SYNCOPE
Psychogenic syncope, or loss of consciousness in the absence of heart rate, blood pressure, electroencephalographic or transcranial Doppler abnormalities, has been reliably diagnosed using the head-up tilt table test.10 Clinical features include sudden and dramatic syncope, a prolonged recovery period, and disorientation after the episode, all features rarely seen in vasovagal attacks.10 Hyperventilation syncope is considered under the same rubric of psychiatric disorder,11 with diagnosis established by the demonstration of hyocapnia (which is thought to stimulate cerebral vasoconstriction) and alkalosis during head-up tilt table testing.11 ,12 Traditionally, arterial blood gas measurement has provided the gold standard for these values, but a recent study reported on the use of end tidal Pco 2 as the marker of hyperventilation (“capnography tilt test”).11
Carotid sinus hypersensitivity
The diagnosis of carotid sinus hypersensitivity rests on the finding of > 3 seconds asystole (cardioinhibitory subtype), > 50 mm Hg fall in systolic blood pressure (vasodepressor subtype), or both (mixed subtype) during carotid sinus massage.14Recurrent syncope caused by carotid sinus stimulation, producing > 3 seconds asystole in the absence of medication that depresses the sinus node or atrioventricular node conduction, is a class 1 indication (level C) for pacemaker implantation, while recurrent syncope without clear, provocative events and with a hypersensitive cardioinhibitory response, is a class IIa indication according to American College of Cardiology/American Heart Association guidelines.51Despite these criteria, there is still wide variation within the UK of implant rates for carotid sinus syndrome, ranging from 25% of all systems implanted in centres with an interest in this disorder, to 1–2% in other UK centres.52 In both the clinical and research arenas, standardisation of carotid sinus massage (CSM), the sole currently practicable diagnostic test for carotid sinus hypersensitivity, is thus desirable.
Indications for carotid sinus massage
CSM should be considered in older patients presenting with loss of consciousness, unexplained falls and presyncope, where history, examination, and other cardiovascular and neurological investigations have not been clearly identified as an attributable cause for symptoms.
Contraindications to carotid sinus massage
Myocardial infarction, transient ischaemic attack (TIA) or stroke in the three months before attendance are absolute contraindications, as is any previous adverse reaction to CSM. Previous ventricular fibrillation (VF) or tachycardia (VT) are relative contraindications. If carotid bruits are present, carotid Doppler ultrasonography should precede CSM. We currently avoid CSM in those with a > 70% stenosis and perform the test supine only in those with a 50–70% stenosis. The presence of a carotid bruit is a poor indicator of the presence or severity of carotid artery stenosis,53 but in the absence of prospective studies on the predictive value of carotid Doppler studies, our current practice reflects a safe and pragmatic approach to this test.
Carotid sinus massage methodology
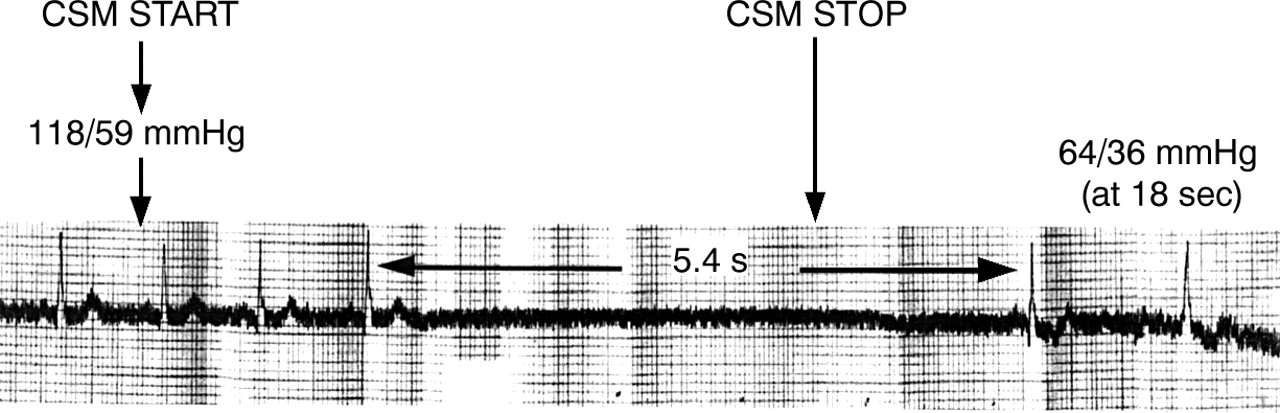
CSM should only be performed by a clinician skilled in the management of its potential complications. Following a detailed history, clinical examination (including carotid auscultation), and explanation of the procedure, the patient should lie supine for a minimum of 5 minutes with surface ECG and blood pressure monitoring on a footplate type tilt table. (Where possible, phasic non-invasive beat to beat blood pressure monitoring (for example, Finapres) is to be preferred since the blood pressure nadir occurs at around 18 seconds, returning to baseline at 30 seconds. Conventional automated systems will thus be insufficiently sensitive to track this rapid response. This is of most importance where the vasodepressor response is of particular interest. Firm, longitudinal massage should then be performed for 5 seconds over the site of maximal pulsation of the right carotid sinus,54 which is located between the superior border of the thyroid cartilage and the angle of the mandible. Some authors recommend continuing CSM for 10 seconds if there is no asystole after 5 seconds,55 but this is not our practice. Simple light pressure over the carotid sinus will not reliably produce a hypersensitive response.
CSM is performed initially on the right side when supine, as up to 66% of subjects with carotid sinus hypersensitivity have a positive response on the right side,56 potentially avoiding the need for repeated CSM. Massage should be discontinued if asystole > 3 seconds occurs (fig 3), while prolonged asystole should result in prompt frappe. Symptoms, including symptom reproduction, blood pressure, and R-R interval should be recorded. If right sided massage is non-diagnostic, the procedure should be repeated, consecutively, in the left supine position, and the right and left 70° head-up tilt position, following haemodynamic re-equilibration in all cases. In up to 30% of subjects the response cannot be elicited in the supine position and is only present during massage in the head upright tilt position.13-15 ,57 At the end of the procedure the patient should remain supine for at least 10 minutes, which in our experience has reduced neurological complication rates.

{kind=link}
{kind=link}
{kind=link}
Mixed carotid sinus hypersensitivity
Complications of carotid sinus massage
Stroke and TIA following CSM are rare.58 ,59 Where neurological signs ensue, the procedure should be abandoned, the patient placed in the supine position, and measures taken to ensure that the blood pressure is returned rapidly to normotensive levels. Consideration should be given to the administration of aspirin 300 mg if not contraindicated. Stroke should be managed as per local guidelines. Cardiac complications, including ventricular60 ,61 and atrial arrhythmias62have been reported rarely. In more than 16 000 episodes of CSM we have never encountered VT or VF,58 ,59 though advanced resuscitation facilities should be immediately to hand.
Conclusion
Neurocardiovascular disorders, including the vasovagal syndrome and carotid sinus hypersensitivity, are some of the most common causes of syncope, but clinical diagnosis and research activity are hampered by the diversity of diagnostic protocols used in different centres. Tilt table testing has developed considerably since its inception as a diagnostic test for vasovagal syncope,1 and the Newcastle protocols provide guidance not only on passive and provocative tilt testing, but also on diagnostic uses of the test outwith the realm of vasovagal syncope. These protocols, based on current evidence and our experience in this field, are an attempt to provide comprehensive guidance on tilt testing and carotid sinus massage, which will be of interest not only to those setting up new units, but also to those with existing similar facilities.