Article Text

Abstract
Background The analytical and clinical validity of cerebrospinal (CSF) biomarkers has been extensively researched in dementia. Further work is needed to assess the ability of these biomarkers to improve diagnosis, management and health outcomes in the clinical setting
Objectives To assess the added value and clinical utility of CSF biomarkers in the diagnostic assessment of cognitively impaired patients under evaluation for Alzheimer’s disease (AD).
Methods Systematic literature searches of Medline, EMBASE, PsycINFO and Web of Science research databases were conducted on 17 December 2022. Data from relevant studies were extracted and independently screened for quality using a tool for bias. Clinical utility was measured by clinicians’ changes in diagnosis, diagnostic confidence and patient management (when available), after their examination of patients’ CSF biomarkers. Cost-effectiveness was assessed by consideration of additional cost per patient and quality-adjusted life years.
Results Searches identified 17 studies comprising 2090 patient participants and 593 clinicians. The meta-analysis revealed that clinicians’ use of CSF biomarkers resulted in a pooled percentage change in diagnosis of 25% (95% CI 14 to 37), an increase in diagnostic confidence of 14% (95% CI 9 to 18) and a pooled proportion of patients whose management changed of 31% (95% CI 12 to 50). CSF biomarkers were deemed cost-effective, particularly in memory services, where pre-test AD prevalence is higher compared with a primary care setting.
Conclusions CSF biomarkers can be a helpful additional diagnostic tool for clinicians assessing patients with cognitive impairment. In particular, CSF biomarkers consistently improved clinicians’ confidence in diagnosing AD and influenced on diagnostic change and patient management. Further research is needed to study the clinical utility of blood-based biomarkers in the clinical setting.
- DEMENTIA
- ALZHEIMER'S DISEASE
- CSF
Statistics from Altmetric.com
Introduction
There are over 850 000 people with dementia in the UK,1 and numbers are expected to rise as the population ages, with over 1.1 million people living with AD in the UK by 2025. The diagnosis of Alzheimer’s disease (AD), which is the most common form of dementia, has advanced in the last decade through the availability of in vivo biological measures or ‘biomarkers’. These biomarkers can detect the pathological hallmarks of AD: pathological tau and beta amyloid proteins, as well as neurodegeneration.2 Biomarkers have been incorporated into the diagnostic framework of AD in clinical research.3 A consensus ‘roadmap’ was set out in 2017 to aid the incorporation of these biomarkers into the clinical setting to improve diagnostic accuracy.4
Cerebrospinal fluid (CSF) biomarkers are currently used in the diagnostic investigation of AD at specialist tertiary Neurology Centres in the UK.5 However, they are not routinely used in UK Memory Services.6 7 CSF biomarkers have demonstrated analytical validity.8 9 Validated AD CSF biomarkers include amyloid-β1–42, total-tau and phosphorylated-tau181 (ptau-181).10 A reduction in Aβ42 and raised levels of ptau are indicative of Aβ and tau pathologies in AD, while increased total-tau is a non-specific marker of neuronal injury.11 Many studies have demonstrated the correlation between CSF levels and neuropathology.12 13 14 15 These CSF biomarkers have garnered attention as, in contrast to imaging biomarkers such as amyloid PET, they are cheap, quick and simple to obtain in a clinical setting.16 However, there are reported concerns regarding lumbar puncture (LP) due to its perceived more invasive nature. The most frequent reported side effect is a post-LP headache.17 Several large multicentre studies have demonstrated that LP is a safe and tolerable procedure.17 18 Further barriers to the routine use of LP in Memory Services include a lack of skills training in this procedure.19
Biomarkers may also assist clinicians in differentiating AD from non-AD dementias, and mild cognitive impairment (MCI) from early AD.20–22
There have been several studies exploring the validity and diagnostic accuracy of CSF biomarkers in AD.23 However, to date, this may be one of the first systematic reviews to explore the clinical utility of CSF biomarkers in the diagnostic evaluation of cognitively impaired patients. In this study, we aim to assess the real-world added value and clinical utility, defined as relative improvement in clinicians’ diagnostic confidence or change in diagnosis or management, of CSF biomarkers in patients being evaluated for cognitive impairment due to AD.
Methods
Study design
A systematic review with mixed-methods quantitative and narrative synthesis was conducted following the Preferred Items for Reporting of Systematic Reviews and Meta-Analyses (PRISMA) guidelines.24
Eligibility criteria
Included studies performed a diagnostic and clinical utility analysis of CSF biomarkers, where clinicians cognitively assessed at least 10 cognitively impaired participants of any age undergoing evaluation for AD. Peer-reviewed published studies in English were included if their primary or secondary outcome included at least one of change in diagnosis, diagnostic confidence, patient management or cost analysis. We excluded reviews, protocols, and conference presentations.
Search strategy
An online literature search was carried out on 17 December 2021 using Medline, Embase, PsycINFO and Web of Science (WoS) databases, using the terms listed in the online supplementary data appendix 1. The search terms were modified to meet the criteria for medical subject headings in the various databases. The references of identified articles were also screened to ensure all relevant studies were included.
Data extraction
Two authors (JH and MW) independently screened and selected potentially relevant abstracts and assessed the full study texts according to eligibility criteria. Any disagreement between authors was resolved through discussion. If there was any further disagreement, this was resolved by discussion with a third author (SR).
Two authors (JH and MW) independently extracted data. If there was a disagreement, this was resolved in discussion between the two raters. We extracted data on study characteristics (design, setting, duration, intervention, inclusion criteria), relevant outcomes (change in diagnosis, diagnostic confidence and change in management plan) and participant characteristics (population, sample size, initial diagnosis, age, sex, demographics).
Risk of bias in individual studies and quality assessment
Two authors (JH and MW) independently assessed studies for bias using a modified Quality Assessment Tool for Quantitative Studies, originally developed by the Effective Public Health Practice Project.25 Any disagreement was resolved by discussion with a third author (SW). Quality of studies was assessed across several domains including selection bias, study design, confounders, data collection method, and withdrawals and dropouts. The scores were collated to give an overall global rating for each paper as “Strong”, “Moderate” or “Weak”. If a study received a weak rating in all areas of bias, it was excluded from the review.
Synthesis of results and meta-analysis
A mixed-methods quantitative and narrative synthesis was carried out due to the small number of studies and heterogeneity in study methodology.
In terms of the quantitative analyses, the percentage of change in diagnoses, diagnostic confidence and management was computed using available study data. A random-effects meta-analysis was conducted to calculate pooled estimates of the percentage change in diagnoses, confidence and management, due to the heterogeneity in study settings and study populations.26 Subanalyses were performed on the percentage change in AD diagnoses, that is, changes in diagnosis from AD to non-AD and from non-AD to AD. The I2 statistic was used to assess the degree of heterogeneity of the percentage change in diagnosis, confidence and management across studies.27 We followed Tu’s 2016 methodology for testing the relationship between percentage change and baseline values, which uses a modified Pearson’s test.28 All analyses were performed using R Software R V.4.1.2; R Foundation for Statistical Computing.29
Results
Study identification
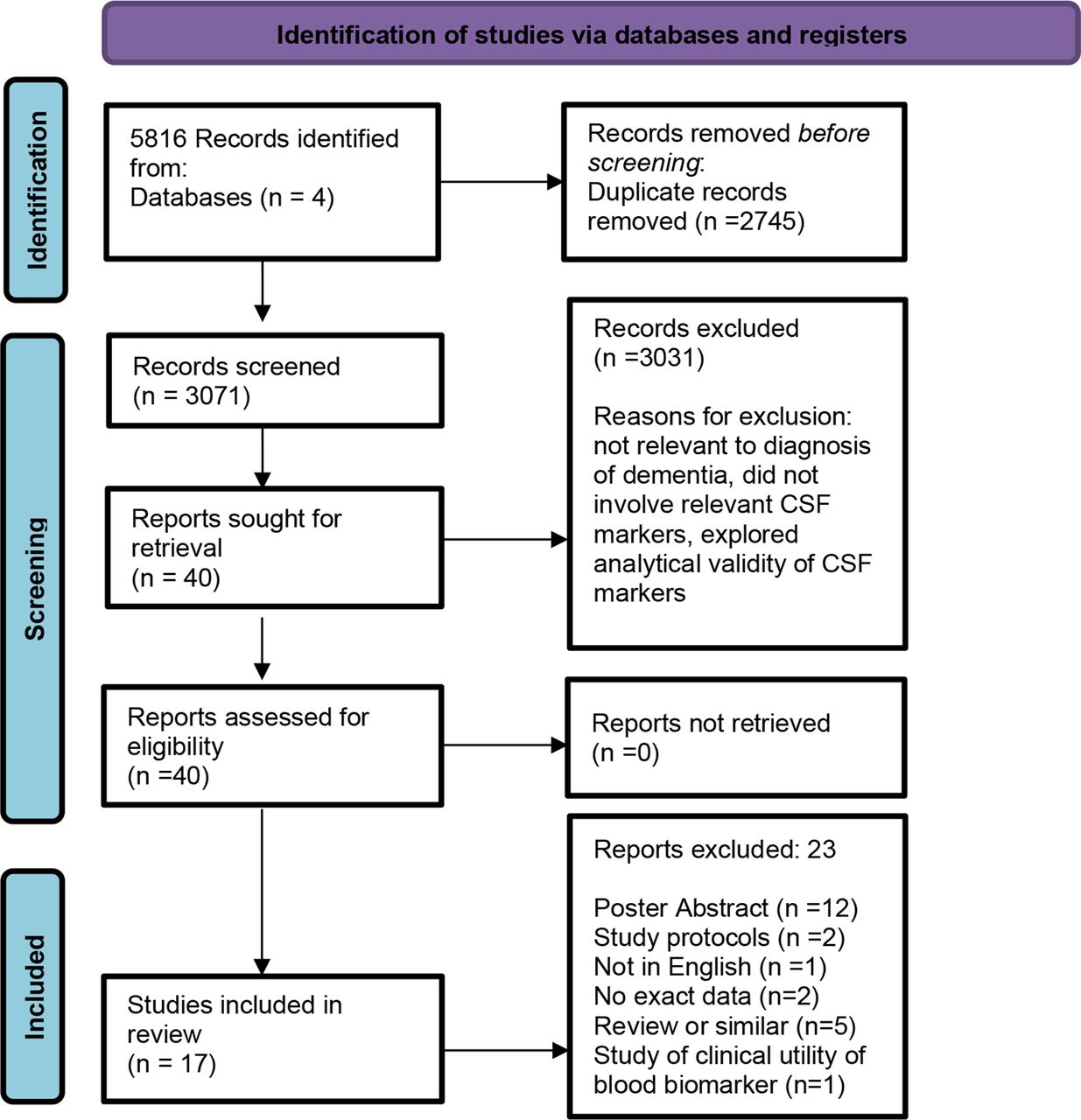
Seventeen studies were identified for inclusion. The PRISMA flowchart is displayed in figure 1. In total, 5816 records were identified from 4 databases; Medline, EMBASE, PsycINFO and Web of Science. After removal of duplications, 3071 records were screened; 3031 records were excluded. Reasons for exclusion included not relevant to diagnosis of dementia, did not involve relevant CSF markers and explored analytical validity of CSF markers. Forty reports were assessed for eligibility. Twenty-three reports were excluded. Reasons for exclusion were poster abstracts, study protocols, not in English, no exact data, review or similar and study of clinical utility of blood biomarker.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of selected papers. CSF, cerebrospinal fluid.
Study characteristics
Study characteristics are shown in table 1 and table 2 and in online supplemental table 2.
Supplemental material
Table of study characteristics observational studies
Table of study characteristics and findings—cost-effectiveness analysis studies
Study design
Most (12 of 17, 71%) of the included studies were prospective observational studies.30–40 One study was a survey of clinicians using simulated clinical scenarios.41 Other study designs included three cost-effectiveness analyses42–44 and two retrospective observational studies.45 46 All studies assessed the impact of CSF biomarker results. The mean sample sizes of patient and clinician participants were 149 and 66, respectively. Seven studies were performed at specialist memory clinics with a single site, five were multicentre and two were early-onset dementia clinics.
Patient and clinician characteristics
The mean age of patient participants in the studies was 66.3 years (±SD 7.66), and two studies restricted inclusion criteria to patients aged <65 years.30 ,34
Of the 17 studies, AD and MCI were the most common initial (pre-biomarker) diagnoses. The initial (pre-biomarker) diagnoses for patient participants in the studies included subjective cognitive disorder, MCI, AD dementia, frontotemporal lobe dementia, vascular dementia, dementia with Lewy bodies, dementia with unknown aetiology, Parkinson’s disease and Parkinson’s plus syndromes, psychiatric disorders or “other”. In addition to AD, the final (post-biomarker) dementia diagnoses included progressive supranuclear palsy, Creutzfeldt-Jakob disease, corticobasal degeneration and Huntington’s disease. Non-demented patients were categorised as “no cognitive disorder”, symptoms of a cognitive disorder caused by a developmental disorder, or a psychiatric or neurological disorder.
Most studies recruited clinicians with a speciality in Neurology, but only one study provided detailed clinician demographics.41
Outcome measures
Outcome measures are described in online supplemental table 2. The majority (13 of 17, 76%) of studies required the clinician to complete a pre-CSF and post-CSF results questionnaire, listing initial and final diagnoses, respectively.30–34 36–41 46 47 Of these studies, eight examined how CSF biomarker results changed diagnostic confidence,32–36 40 41 46 and seven assessed their impact on patient management, defined as the initiation or discontinuation of dementia medications such as cholinesterase inhibitors, the ability to enrol in clinical trials, and/or length of follow-up.32–34 37 39 41 46
Of the three studies that performed a cost-effectiveness analysis of CSF biomarkers to diagnose AD,42–44 two examined lifetime costs and quality-adjusted life-years (QALYs)42 43 and one performed an economic evaluation.44 Outcome measures are described in table 2.
Quality assessment
Most (14 of 17, 83%) studies were assessed as being of moderate quality30–41 45–47 and three studies were assessed as being of high quality.42–44 No studies were assessed to be of low quality (online supplemental table 1). High-quality studies comprised the cost-effectiveness analysis, which included in the study design methods to reduce confounding and selection bias. For the studies of moderate quality, study quality limitations included limited information about baseline clinician demographics and ethnic diversity of the patient participant study population, observational study design, and a lack of a validated or uniform method of data collection on questionnaire.
Findings
Change in diagnosis
Eleven studies, comprising 1891 patient participants and 395 clinician participants, reported on the percentage change in clinicians’ diagnosis after the availability of fluid biomarker results,31–33 35–40 45 46 which ranged between 7% and 61%. The overall pooled percentage change in diagnoses was 25% (95% CI 14 to 37) and there was substantial heterogeneity (I2 97%, p<0.001) (figure 2a). Subgroup analyses found no significant change in diagnoses from initial AD to final non-AD or initial non-AD to final AD (online supplemental figuers1A and B).

{kind=link}
{kind=link}
(A) Forest plot showing the pooled percentage change in diagnosis. (B) Forest plot showing the pooled percentage change in confidence. (C) Forest plot showing the pooled proportion of patients whose management changed (%).
Two studies explored the accuracy of clinicians’ final diagnoses through longitudinal patient follow-up. In one study, after 12 months of follow-up, 89% of patients’ diagnoses were found to be correctly classified.46 Similarly, another study showed that after a mean follow-up time of 31 months, 88% of AD participants maintained their diagnosis and all MCI participants who had positive CSF results progressed to AD dementia.30
Clinician-rated diagnostic confidence
Eight studies calculated and showed an overall increase in diagnostic confidence,32–38 40 ranging from 5% to 22% (online supplemental table 2). The overall pooled percentage change in confidence was 14% (95% CI 9 to 18) and there was substantial heterogeneity (I2 88%, p<0.001) (figure 2b).
The change in confidence was inversely proportional to the initial pre-test confidence level, such that lower pre-test confidence was associated with a greater percentage change in confidence (Pearson’s r=−0.91, p<0.001).
Two studies that reported an overall increase pooled percentage change in confidence also showed a decrease in diagnostic confidence for a minority of clinicians.33 35 This was often associated with patients for whom CSF results did not alter the final diagnosis and who had a pre-biomarker diagnosis of subjective memory complaint or a psychiatric disorder.33
Change in management
Five studies, comprising 918 patients, evaluated the impact on CSF biomarkers on patient management.32 33 38 39 46 The overall proportion of patients whose management changed after availability of fluid biomarkers ranged between 13% and 47%, and the overall pooled proportion of patients whose management changed was 31% (95% CI 12 to 50) with substantial heterogeneity (I2: 97%, p<0.001) (figure 2c). The most common management change was the commencement or stopping of cholinesterase inhibitors or other dementia medications (four of five studies).
Cost-effectiveness
Three studies analysed the cost-effectiveness of CSF biomarkers to diagnose AD in MCI and dementia populations: a 2014 Spanish study and two studies published in 2017 from Canada and The Netherlands. All three studies assessed CSF biomarkers (amyloid-beta 1–42, total tau and phosphorylated tau). In one study,44 CSF biomarkers were reported to be an alternative, less expensive and more efficient diagnostic tool compared with standard diagnostic procedures in patients with MCI, as per guidelines of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINDS-ADRDA guidelines). The same study reported that for patients with dementia, despite higher uncertainty, CSF biomarkers were also a cost-effective alternative compared with standard clinical diagnostic criteria.
A second study43 used a Markov model to estimate the lifetime costs and QALYs of CSF biomarkers in patients referred for cognitive assessment with suspected AD, where diagnosis remained unclear after neuroimaging. The study reported that the cost-effectiveness of CSF biomarkers depended on the prevalence of AD in the population, such that with a pre-test probability of AD of 12.7%, the addition of CSF biomarkers to neuroimaging had an incremental cost-effectiveness ratio (ICER) of $C11 032 per QALY gained. However, at a lower prevalence such as in the general practice setting, CSF biomarkers were unlikely to be cost-effective at a willingness-to-pay threshold of $C50 000 per QALY gained. The study concluded that CSF biomarkers are likely to be cost-effective in specialist memory clinics where pre-test prevalence may be greater than 15%.
The third study42 found that the use of CSF biomarkers in an MCI population resulted in an ICER of €9,416, although there was a high degree of uncertainty. This was due to the uncertainty of input parameters computed in the model such as expert opinions and risk prediction coefficients.
CSF in addition to FDG-PET or amyloid-PET imaging
Four studies examined the additional benefit of CSF biomarkers in participants who had specialist FDG-PET or amyloid-PET imaging.34 38 45 46 One study reported that CSF biomarkers and amyloid-PET results showed a good concordance and that there was no difference in terms of added diagnostic value between them, with no apparent benefit of using another biomarker if amyloid-PET or CSF biomarkers had been performed.34 However, in another study, amyloid-PET provided greater changes in diagnosis and diagnostic confidence than CSF biomarkers.38
For participants correctly diagnosed as patients with AD, CSF biomarkers had a significantly higher impact on diagnostic and a significant reduction in the need for further investigations when compared with FDG-PET.46 One study reported that for 35% of patient participants, FDG-PET and CSF-based diagnosis did not correspond.45
Discussion
Previous systematic reviews have reported on the analytical or clinical validity of fluid biomarkers, or the clinical utility of imaging biomarkers such as amyloid-PET.48–51 In this review, we focused specifically on the clinical utility of CSF biomarkers in the assessment of patients with cognitive impairment and the cost-effectiveness of CSF biomarkers for AD.
Use of CSF biomarkers resulted in a change in diagnosis in 25% of cases, although this was not specific to any direction of diagnostic change (AD to non-AD or non-AD to AD). This result is similar to the overall change of diagnosis of 35.2% after amyloid-PET.48
Biomarker results are likely to provide an additional diagnostic assessment tool that clinicians will consider in combination with clinical findings. In one study that provided simulated clinical vignettes to clinicians,41 an AD clinical presentation with AD CSF results led to a significantly increased odds of an AD diagnosis, whereas when clinicians were given borderline CSF values, they relied on other clinical information to decide on the final diagnosis. Also, when clinicians were shown a mild AD clinical presentation with normal CSF results, they often chose a diagnosis of unknown aetiology, and when clinicians were shown an ambiguous clinical presentation with AD CSF result, they were more likely to make an AD diagnosis.
Studies consistently reported that CSF biomarkers improved clinicians’ diagnostic confidence with a pooled mean increase of 14%. This is in comparison with the impact of amyloid-PET where the change in confidence level reportedly ranged from 16% to 44%.48 However, some studies reported that biomarker results resulted in a reduction in confidence, for example, in the context of unexpected biomarker results when patients with subjective cognitive complaint or a psychiatric disorder had abnormal dementia biomarkers, or when patients initially diagnosed with AD had normal biomarkers. It is relevant that higher diagnostic confidence may not always equate to greater clinical utility,31 as decreased confidence after CSF results could sometimes help a clinician to question their pre-CSF diagnosis and prevent an incorrect diagnosis. A reduction in diagnostic confidence may also spur further diagnostic tests and have a substantial impact on management.
Use of CSF biomarkers led to a change in management in 31% of cases, mostly involving the initiation or discontinuation of cholinesterase inhibitors. One review examining the impact of amyloid-PET found that the overall change in management was 59.6%,48 which represents a larger pooled effect size compared with CSF biomarkers. This may be due to factors such as the proportion of patients already prescribed medication and degree of diagnostic certainty prior to amyloid-PET imaging. However, amyloid-PET is costly, less accessible and provides information solely on amyloid deposition.52 Cost-effectiveness analyses revealed CSF biomarkers to be a cost-effective alternative to standard diagnostic work-up.42–44
There was conflicting evidence regarding the utility of CSF biomarkers in addition to specialist imaging including FDG-PET and amyloid-PET.
Despite the findings in this review, there is low utilisation of CSF biomarkers in memory services in the UK, where staff to do not have access to the specialist equipment and expertise to perform routine LPs. There have been recent advancements in the validation of blood-based biomarkers, such as ptau-181 and ptau-217, which have been shown to have similar sensitivity and specificity to CSF biomarkers.53 In one prospective observational study, serum neurofilament light was perceived as a useful additional tool to CSF biomarkers in 53% of cases by neurologists in a tertiary memory clinic.47 In a recent position statement, blood biomarkers were recommended in memory clinics as part of the diagnostic work-up of patients with cognitive symptoms, with the results confirmed where possible with CSF or amyloid-PET imaging.54 Further studies are needed to establish if the clinical utility of blood-based biomarkers is comparable with CSF biomarkers and amyloid PET imaging. Blood-based biomarkers are simple to carry out and cost-effective.16 They could be made widely available and have the potential to be used within UK memory services to support the diagnosis of Alzheimer’s dementia.
In the UK, there is a lack of information on the investigation and management of MCI in the NICE guidelines.55 It would be important to address this in future guidance, given the increasing proportion of people diagnosed as MCI in UK memory services.56
Limitations
The interpretation of the findings is limited by the small number of included studies, small sample sizes and high methodological heterogeneity. Most included studies were of moderate quality. Study quality limitations included lack of information about baseline clinician demographics and were observational studies.
Only one study reported on clinician demographics such as ethnicity, age and level of seniority, and most clinicians were neurologists, so it is unknown how these clinician factors may have influenced the outcome measures, such as degree of diagnostic confidence and familiarity with the use of fluid biomarkers. The extent to which these findings are generalisable to other clinician specialities involved in making dementia diagnoses is also unclear.
Most studies include a population of mainly white and well-educated participants. In future studies, it will be important to investigate the use of CSF biomarkers in more diverse populations. The mean age of patients included in these studies was 66.1 years. Future studies should investigate older patients, who are more representative of local memory service populations.
Some studies requested clinicians in Memory Services to complete questionnaires on a voluntary basis, which may have introduced a selection bias as clinicians with a higher inclination to use biomarkers and find them useful in clinical practice may have been more likely to respond.32
No studies confirmed the final diagnosis with postmortem brain study findings, so we were unable to assess the overall diagnostic accuracy of fluid biomarkers. Future larger longitudinal studies would be helpful to assess the diagnosis accuracy of these methods.
Only one study assessed the clinical utility of a serum biomarker, sNfL, in the diagnosis of neurodegenerative diseases.47 Further studies are needed to assess the clinical impact of other blood-based biomarkers.
Conclusion
CSF biomarkers provide additional value in the diagnostic assessment of cognitively impaired patients presenting to memory clinic through changes in clinical diagnoses, improved diagnostic confidence and changes to patient management. Large multicentre studies have shown LP to be a safe and tolerated procedure. In the future, fluid biomarkers, especially blood-based biomarkers, offer a simple-to-obtain, cost-effective and scalable test to support clinicians in the diagnosis of Alzheimer’s dementia.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the conception and design of the review. MW and JH completed the data collection. JH and KYL performed the data analysis and interpretation. All authors contributed to drafting of the article, revision of the article and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.