Article Text

Abstract
Background: Guillain–Barré syndrome (GBS) is generally considered to be monophasic, but recurrences do occur in a presently undefined subgroup of patients.
Objectives: To determine which subgroup of patients develops a recurrence and to establish whether preceding infections and neurological symptoms are similar in subsequent episodes.
Methods: A recurrence was defined as two or more episodes that fulfilled the NINCDS criteria for GBS, with a minimum time between episodes of 2 months (when fully recovered in between) or 4 months (when only partially recovered). Patients with a treatment-related fluctuation or chronic inflammatory demyelinating polyneuropathy with acute onset were excluded. The clinical characteristics of recurrent GBS patients were compared with those of 476 non-recurrent patients.
Results: 32 recurrent GBS patients, who had a total of 81 episodes, were identified. The clinical symptoms in a first episode were similar to the following episodes in individual patients, being GBS or its variant Miller Fisher syndrome (MFS) but never both. While neurological symptoms in subsequent episodes were often similar, the severity of the symptoms and the nature of the preceding infections varied. Recurrent patients (mean age 34.2 years) were younger than non-recurrent patients (mean age 46.9; p = 0.001) and more often had MFS (p = 0.049) or milder symptoms (p = 0.011).
Conclusions: Genetic or immunological host factors may play an important role in recurrent GBS, since these patients can develop similar symptoms after different preceding infections. Recurrences occur more frequently in patients under 30, with milder symptoms and in MFS.
Statistics from Altmetric.com
Guillain–Barré syndrome (GBS) is an acute polyradiculoneuropathy leading to flaccid paresis. Its annual incidence rate is 0.75 to 2 per 100 000.1 2 GBS is a heterogeneous disease in which approximately two-thirds of patients report a preceding incident, usually an infection, such as diarrhoea or an upper-respiratory-tract infection.
Although GBS is considered to be monophasic, recurrences are reported in 2–5% of patients.3 4 It is unknown why some patients have a recurrence and whether this occurs more frequently in a distinct subgroup of patients. It is suggested that recurrent GBS patients may have similar clinical symptoms in subsequent episodes, while having the same or different triggering events.4 It is important to distinguish between recurrent GBS patients and GBS patients with treatment-related fluctuations (GBS-TRF) or chronic inflammatory demyelinating polyneuropathy with acute onset (A-CIDP) especially because the treatment regimen for CIDP is different.5
The purpose of this study is to establish whether recurrent GBS patients have similar neurological symptoms in subsequent episodes and to determine whether these patients can be distinguished from non-recurrent patients based on their clinical characteristics. We additionally investigate whether recurrent GBS patients have similar infections prior to each episode, if the severity varies in subsequent episodes and if the interval between episodes tends to get longer or shorter. By analysing these features, we also aim to determine the relevance of host susceptibility factors in GBS.
METHODS
Subjects and methods
To determine whether the type of neurological symptoms or the type of preceding infections are similar in subsequent episodes, we studied 32 recurrent GBS patients. These patients were identified from the Erasmus MC GBS data bank, which contains information on patients enrolled in clinical studies between 1985 and 2008. Additional patients came to our attention on patient meetings organised by the Dutch Society for Neuromuscular disorders (VSN). Medical records or letters were screened, and missing or indistinct items were clarified by contacting the patients or treating doctors.
All cases were re-evaluated (by KK and PD) using the criteria of the National Institute of Neurological and Communicative Diseases and Strokes (NINCDS) for GBS.6 Patients were also included when they fulfilled the criteria for Miller Fisher syndrome (MFS), a GBS variant characterised by areflexia, ataxia and opthalmoplegia.1 The severity of each episode was graded according to the GBS disability scale.7
The GBS disability scale is a seven-point disability scale, ranging from no symptoms (zero points) to death (six points). Patients who were able to walk with or without support (GBS disability scale ⩽3) were considered as “mildly affected,” whereas patients who were bedbound (GBS disability scale ⩾4) were categorised as “severely affected.”
We defined a recurrent patient as one having two or more episodes that fulfilled the NINCDS criteria for GBS, with either a minimum interval ⩾4 months between the episodes if the patient did not recover completely (GBS disability scale ⩾2) or ⩾2 months when there was a complete or near-complete recovery (GBS disability scale ⩽1) after the previous episode.
We excluded GBS-TRF and A-CIDP patients.5 GBS-TRF was defined as (1) improvement in the GBS disability scale of at least one grade or improvement in the MRC sum score more than five points after completion of therapy (2 g intravenous Ig/kg body weight in 2–5 days), followed by a worsening of the GBS disability scale of at least one grade or a decrease in the MRC sum score of more than five points within the first 2 months after the disease onset or (2) stabilisation for more than 1 week after completion of therapy, followed by a worsening of the GBS disability scale of more than one grade or more than five points on the MRC sum score within the first 2 months after disease onset.5 8 A-CIDP was defined as a CIDP patient in whom the nadir of the first episode was within 8 weeks of onset, and the consecutive course was chronic, as in CIDP.9
Information was obtained concerning age, sex, cranial nerve involvement, preceding type of infection and/or trigger, GBS disability scale at nadir, and time between recurrences. Antecedent infections were classified clinically either as upper-respiratory tract or as diarrhoea/gastrointestinal. Reported flu or flu-like infections were classified as upper-respiratory-tract infections. Information was also obtained about the presence of other autoimmune or immune-mediated disease.
To investigate whether recurrent patients can be distinguished from non-recurrent patients, we compared the clinical characteristics with those of non-recurrent GBS patients admitted with a diagnosis of GBS between 1987 and 1996 in The Netherlands.2
We compared the groups with respect to age, sex, MFS, cranial nerve dysfunction, the need for artificial respiration, severity of the symptoms and preceding triggers.
Statistical analysis
For statistical analyses, an unpaired t test and χ2 test were performed, to compare characteristics of recurrent and non-recurrent GBS patients. If appropriate, the Fisher exact test was used. SPSS for Windows (version 15.0, SPSS, Chicago) was used for all statistical analyses, and p values <0.05 were regarded as significant.
RESULTS
Forty-eight patients were considered as potentially eligible. Sixteen patients were excluded: three with GBS-TRF and six with A-CIDP; three due to missing information about clinical symptoms during one of the possible episodes, and four because they did not fulfil the diagnostic criteria for GBS.
We identified 32 recurrent patients, 21 males and 11 females, who had a total of 81 episodes of GBS. Of these 32 patients, four had recurrent MFS, and three were known with another autoimmune disease (two inflammatory bowel disease and one hyperthyroidism). In the group of non-recurrent GBS patients, 11 were known to have one of the following autoimmune disorders: rheumatoid arthritis, polyartritis nodosa, spondylitis ankylopoetica, sarcoidosis, thyroid gland disease or inflammatory bowel disease. The clinical characteristics of the recurrent GBS patients during their first episode are listed in table 1.
Seven recurrent GBS patients had three episodes, two had four episodes, and two had five episodes. All patients with at least four episodes were female. The mean age during the first episode was 34.2 (range 1–87) and of the first recurrence 42.1 (range 5–88). The interval between recurrences ranged from 2 months to 37 years. The mean interval between all recurrences was 7 years. Most patients had a long interval between subsequent episodes, and only two patients had an interval of 2 months in between episodes with near complete recovery. The mean GBS disability score at nadir was 3.1 for the first two episodes, increasing to 3.8 for the fourth episode. The characteristics of all episodes are shown in table 2.
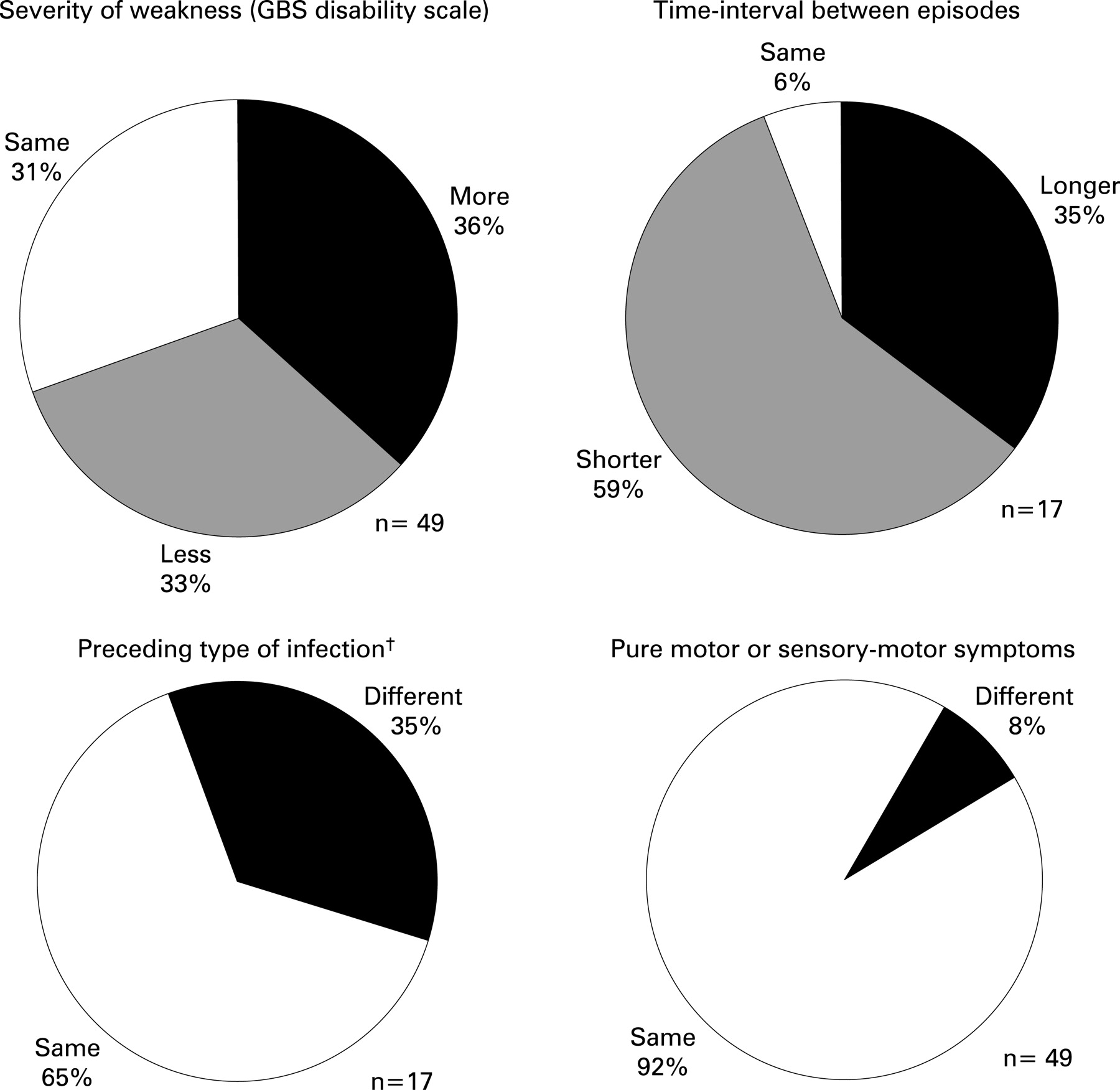
The GBS disability scale, type of preceding infection and neurological symptoms (pure motor or sensory–motor) were compared with the previous episode. The characteristics during a recurrence were compared with those during the previous episode (fig 1).
{kind=link}
In individual patients, a preceding infection in two subsequent episodes was reported 17 times. Eleven times the infections were reported as either respiratory or gastrointestinal, whereas six times a gastrointestinal infection was reported prior to one episode and a respiratory infection before the other. Two patients had an upper-respiratory-tract infection preceding three episodes and a gastrointestinal before another. Four patients had a serologically confirmed infection prior to one episode; one patient had a varicella zoster virus and a Mycoplasma pneumoniae, one a herpes simplex virus infection and two a Campylobacter infection.
One patient reported a tetanus vaccination as a trigger in two subsequent episodes. Another patient, with inflammatory bowel disease, had two episodes of GBS after starting treatment with the drug Salazopyrine. In the two patients, reporting the same trigger in subsequent episodes, neurological symptoms developed faster in the second episode. Two other patients reported a vaccination (flu virus or hepatitis virus) as a trigger prior to one of the episodes.
In 18 out of 49 successive episodes (36%) there was a more severe GBS disability scale at nadir; in 16 (33%) a less severe GBS disability scale and in 15 (31%) the GBS disability scale was equal in comparison with the previous episode.
Most patients had either pure motor or sensory–motor symptoms in subsequent episodes (fig 1). None of the patients initially had GBS in one episode followed by MFS in a subsequent episode.
One patient had right-sided oculomotor nerve dysfunction in four subsequent episodes, and another patient had three episodes with right-sided oculomotor nerve and abducens nerve palsy, accompanied by dysphagia. One patient had acute motor axonal neuropathy (AMAN) with moderate recovery five times over a period of 14 years.
In the recurrent group, patients more often had MFS (13% vs 4%, p = 0.049) and were more frequently <30 years (44% vs 22%, p = 0.006) and more often had a mild course (59% vs 37%, p = 0.011) compared with the non-recurrent group. The mean age was lower in the recurrent group than in the non-recurrent group (34.2 vs 46.9, 95% CI −20.4 to −4.9, p = 0.001). The clinical characteristics of recurrent and non-recurrent patients are listed in table 1.
DISCUSSION
The patients with a recurrent GBS in our study showed similar signs and symptoms during every episode despite having different types of symptoms of a preceding infection. This may indicate that genetic and immunological host factors partly determine the clinical phenotype irrespective of the preceding infection. The recurrent patients were younger and more often had MFS and a milder course of disease, which suggests that a distinct subgroup of patients has a higher susceptibility of recurring.
To our knowledge, this is the largest group of recurrent GBS patients described so far, and a comparison with non-recurrent patients has not been documented before. We excluded GBS-TRF and A-CIDP patients. One study reported 12 “recurrent” patients with a progressive phase of less than 8 weeks, therefore not excluding the possibility that some of these patients had A-CIDP or subacute GBS.3 Distinguishing between recurrent GBS, GBS-TRF and A-CIDP can be difficult but is clinically relevant because treatment may differ. In a previous study, we found that nine out of 11 patients with GBS-TRF had their TRF within 9 weeks from onset, and most patients having an exacerbation after 9 weeks eventually developed CIDP.5
Whether clinical symptoms and preceding infections differ in recurrent patients has already been addressed in other case studies and is controversial.10–12 Two studies have reported different antecedent events in individual recurrent GBS patients.10 11 In contrast, another study described similar antecedent illnesses in individual recurrent GBS patients.12 Unfortunately, infection serology in this group of patients was not always testable since serum was not systematically obtained. Two of our patients appeared to have had recurrences after the same specific triggers, one after the drug Salazopyrine and one after a tetanus vaccination; both showed a shorter time between trigger exposure and symptom onset the following episode. Tetanus toxoid vaccination as a trigger for GBS with a shorter symptom onset in subsequent episodes has been reported previously.13 The drug Salazopyrine has not previously been described as a trigger for GBS, but ulcerative colitis has.14 We cannot exclude that these events occurred coincidental or that there had not been a subclinical preceding infection in this patient.
In subsequent episodes, most of the recurrent GBS patients had either pure motor or sensory–motor symptoms. Some patients had very specific symptoms during subsequent episodes, such as unilateral cranial nerve palsy at the same site. We cannot explain this specific finding, but it could be related to a local susceptibility of neural tissue-related epitopes, as replicated laterality of cranial nerve dysfunction has been described before in MFS.15 16
Our observations identify a trend towards shorter intervals between subsequent recurrences, and a more severe deficit with each recurrence. The GBS disability scale is not a linear scale, but a tendency to accumulate neurological deficits after each episode has been reported previously.4 It has been established that patients over 50 years of age are more likely to have a worse recovery, which may explain that disability becomes worse after each subsequent recurrence.17 Recurrent patients are more likely to have MFS than non-recurrent patients. The presence of anti-GQ1b antibodies in almost all MFS patients highlights the importance of immunological factors in this disorder. Since females are more susceptible to autoimmune diseases, it is of interest that the recurrent patients with at least four episodes were all female. Three of the recurrent GBS patients were known with another autoimmune disease, which suggests that genetic host factors are relevant.
The mean age was significantly lower in the recurrent group compared with non-recurrent GBS patients. Age as a risk factor for a recurrent GBS has not been described before, but it has for CIDP. The mean age of relapsing CIDP patients (27 years) is reported to be significantly lower compared with CIDP patients with a non-relapsing course (51 years).18
Due to the retrospective nature of our study, we cannot estimate unbiased the exact incidence of recurrent GBS, but as there were 32 recurrent patients out of a total of 524, the crude estimated prevalence will be around 6%. We cannot exclude the fact that some non-recurrent GBS patients have developed a recurrence outside the geographic boundary of the study area or after the 10-year study period. It is possible that some “non-recurrent” patients had their first GBS episode just before the end of the study period, which would have limited the chance of recording a recurrence.
Individual patients developed either GBS during all episodes or MFS, never both. Because recurrent GBS patients were significantly younger, more mildly affected and more often had MFS, neurologists should be aware that these patients are more prone to recurrences. Since similar neurological symptoms can occur after different infections, this study further indicates that immunological and genetic host factors play a role in determining the clinical phenotype in recurrent GBS.
REFERENCES
Footnotes
-
See Editorial Commentary, p 3
-
Funding: None.
-
Competing interests: None.