Article Text

Abstract
Background and aim: Muscle weakness is a potentially important, yet poorly studied, risk factor for falls. Detailed studies of patients with specific myopathies may shed new light on the relation between muscle weakness and falls. Here falls in patients with facioscapulohumeral disease (FSHD) who suffered from lower limb muscle weakness were examined. This study provides insights into the prevalence, relevance and pathophysiology of falls in FSHD.
Methods: A validated questionnaire was used as well as a prospective 3 month follow-up to examine the prevalence, circumstances and consequences of falls in 73 patients with FSHD and 49 matched healthy controls. In a subgroup of 28 subjects, muscle strength was also examined and balance was assessed electrophysiologically using body worn gyroscopes.
Results: In the questionnaire, 30% of the patients reported falling at least once a month whereas none of the controls did. Injuries occurred in almost 70% of the patients. The prospective study showed that patients fell mostly at home, mainly due to intrinsic (patient related) causes, and usually in a forward direction. Fallers were unstable while climbing stairs, rising from a chair and standing with eyes closed whereas non-fallers had normal balance control. Frequent fallers had greater muscle weakness than infrequent fallers.
Conclusion: These findings demonstrate the high prevalence and clinical relevance of falls in FSHD. The relation between muscle weakness and instability among fallers is also highlighted. Because patients fell mainly at home, fall prevention strategies should focus on home adaptations. As mainly intrinsic causes underlie falls, the impact of adopting balance strategies or balance training should be explored in this patient group.
Statistics from Altmetric.com
In patients suffering from neurological diseases, falling is a prevalent and clinically relevant problem. For example, in patients with Parkinson’s disease, about 50% fell at least once during a 6 month follow-up period and 25% experienced multiple falls.1 2 Comparable fall rates have been reported for patients with other central neurological disorders, such as cerebellar ataxia3 or Huntington’s disease.4 Injuries, fear of falling and an associated reduction of activities are also common among patients with neurological diseases.5
Much less is known about fall rates in patients with neuromuscular disorders. In one study, 27% of patients with a variety of neuromuscular disorders fell during a 3 month follow-up period. Among these, 79% of fallers sustained minor and 5% major injuries.6 Many patients reported fear of recurrent falling (58%), which also increases the risk of falls.7 A prospective study among patients with myotonic dystrophy showed a 10-fold increase in falls compared with healthy controls.8 Among patients with motor neuron disease, 30% experienced falls.5 In a small study among 11 patients with inclusion body myositis, six patients gave a history of falls.9
Developing optimal prevention strategies calls for good understanding of the complex pathophysiology of falls. Patient related risk factors such as cognitive impairment, previous falls, problems with dual tasks and use of sedative medication are examples of generally accepted risk factors for falling.1 5 6 10 More recent work has emphasised muscle weakness as another potentially important, but hitherto poorly studied, risk factor for falls.11 Weakness is often reported as a contributing element when present in elderly patients who feature multiple risk factors. But the risk of muscle weakness per se has rarely been studied. Lower extremity weakness increases the risk for recurrent falls threefold in the elderly.12 Muscle weakness has also been directly and indirectly associated with falls in post-polio patients.13 However, the prevalence and clinical relevance of falls in patients with various neuromuscular disorders featuring muscle weakness remains unclear.11 Intentionally, such epidemiological studies in neuromuscular patients could also serve as an “experiment of nature” to provide insights into the pathophysiology of falls.
As a first step, we studied the epidemiology and pathophysiology of falls in patients with facioscapulohumeral dystrophy (FSHD). We chose FSHD for four reasons.
FSHD is the third most common inherited muscular dystrophy.14 15
Our clinical impression is that falls among these patients are common and debilitating but this has never been studied formally.
FSHD is characterised by a specific pattern of weakness. It initially affects the facial, scapular and humeral muscles, then the peroneal muscles in 80% and pelvic girdle muscles in 20% of patients.14 Thus depending on disease stage and its progression pattern, patients may suffer from severe or minor, proximal, distal or overall weakness, allowing us to study the contribution of the severity and pattern of weakness on fall rates.
Other potential intrinsic risk factors for falling, such as visual deficits or somatosensory disorders, are usually absent in patients with FSHD.14 16 17
Because no cure exists for FSHD, care is essential. Developing fall prevention strategies should be an essential part of this care.
Our approach was bifold. We conducted a combined epidemiological and pathophysiological study that aimed to determine the prevalence, clinical relevance and mechanisms of falling in patients with FSHD. To this end, a validated retrospective questionnaire and a prospective follow-up were conducted. A balance assessment was performed among a subgroup of participants to see whether this could differentiate fallers from non-fallers and provide leads for prevention. A muscle strength assessment was performed to determine the influence of the severity and pattern of muscle weakness on falls. We hypothesised that FSHD patients have a greater fall incidence than healthy controls. The frequency and pathophysiology of falls is expected to be associated with the presence of either or both distal and proximal muscle weakness.
Methods
Participants
A total of 104 adult patients with a definite diagnosis of FSHD were asked to participate. Patients were recruited via the Neuromuscular Centre of the Radboud University Nijmegen Medical Centre and via the Dutch Neuromuscular Diseases Association (Vereniging Spierziekten Nederland, VSN).18 We purposely included patients with a broad spectrum of disease severity because of the exploratory nature of our study. Seventy-seven patients (74% of the eligible population) agreed to participate in the retrospective part of the study. Six did not return the falls questionnaire and were not included in the retrospective analysis. We also included 47 healthy controls, mainly partners or other carers. Seventy-three patients agreed to participate in the prospective follow-up which was completed by 72 patients (67 patients from the retrospective study plus five more) and 49 controls (47 from the retrospective study plus two more). The only exclusion criteria were the inability to read and write the Dutch language and any psychiatric or cognitive disease. Demographic and anthropometric details of the participants are given in table 1. In a subgroup of the participants, muscle strength and balance were assessed (see also table 1). For these participants, disease severity of FSHD was scored using a 10 grade clinical severity scale19 adapted from the Ricci score.20 The study was approved by the ethics committee of the Radboud University Nijmegen Medical Centre.
Participants characteristics of prospective fall study
Procedure
Epidemiology
A fall was defined as “any unexpected event that caused the person to land unintentionally on any lower surface (floor or object) regardless of any sustained injury”. A near fall was defined as “an event where a person lost balance, but prevented falling by regaining balance or seeking external support”.
Retrospectively, participants were asked to complete a questionnaire, detailing their current medical condition (including neurological, orthopaedic, balance problems), prior history of falls, near falls and stumbles for the last week, month, year, and fall frequency in general, and the consequences of these falls. Participants also reported the site and (subjective) severity of their muscle weakness. The questionnaire also included questions regarding the functional ability of performing four different tasks: standing on toes and standing on heels requiring mainly distal lower limb strength, and getting up from a chair and walking stairs requiring mainly proximal strength. The questionnaire had been validated in previous studies on falls in patients with neurodegenerative disorders1 3 4 and a pilot study in patients with neuromuscular disorders.6 The questionnaire gave us the opportunity to determine fall prevalence, relevance and its relation to muscle weakness over a longer period.
Additionally, participants were contacted by telephone once a week over 13 weeks to register any falls prospectively. The telephone call was delivered by an automatic computer phone system (Pfizer Medconnect, Capelle aan den Ijssel, The Netherlands). All participants received written instructions on how to answer this phone call. The researcher personally contacted the subjects who could not be reached by computer and also approached all subjects who had fallen. During this personal telephone interview, information was gathered about the timing, location, preceding activities, direction, consequences (eg, injuries) and apparent cause of the fall. The follow-up enabled us to collect detailed information on fall circumstances for each fall separately.
Pathophysiology
Balance assessment
Balance was measured in a subgroup of participants (see table 1), including eight frequent fallers (with at least one fall a year according to the questionnaire and at least two falls during the follow-up), nine infrequent fallers (with less than one fall a year according to the questionnaire and a maximum of one fall during the follow-up) and nine healthy controls (with less than one fall a year according to the questionnaire and a maximum of one fall during follow-up). Balance was measured using body worn gyroscopes21 measuring trunk sway in the forward–backwards (pitch) and sideways (roll) direction during several stance and gait tasks. The system measuring balance control (Swaystar Balance International Innovations GmbH, Switzerland) was connected to a computer via a Bluetooth connection. The stance tasks lasted 20 s and consisted of standing on firm surface with eyes closed, and standing on a foam support surface with eyes open and eyes closed. The gait tasks included climbing stairs (two steps of height 30 cm); walking eight tandem (heel-to-toe) steps; and rising from a chair and walking 3 m. In addition, a timed up and go test (ie, rise from a chair, walk 3 m, turn around and return to a seated position in the chair) was completed without wearing the device. The balance assessment provided us with information on high fall risk activities and with a method to differentiate fallers from non-fallers.
Muscle strength assessment
To determine whether fall prevalence relates to severity and pattern of muscle weakness, upper and lower limb muscle strength were evaluated by manual muscle testing according to the Medical Research Council (MRC) scale22 in eight frequent fallers, 10 infrequent fallers and 10 controls. Specifically, shoulder abduction and exorotation; elbow flexion and extension; wrist flexion and extension; hip ante- and retroflexion and ab and adduction; knee flexion and extension; and ankle plantar and dorsiflexion were tested.
Data analysis
The main outcome measures were self-reported frequency of falls, near falls and stumbles. Secondary outcome measures were self-reported circumstances and consequences of falls. The latter included injuries, fear of falling and reduction of activities due to fear of falling. Self-reported muscle weakness and the (in-)ability to do certain functional tasks were compared with fall frequencies. Trunk sway angles in the roll (side-to-side) and pitch (for-aft) direction for the gait tasks and trunk angular velocities for the stance tasks were used as outcomes of the balance assessment. Differences between patients and controls were assessed using the unpaired Student t test, ANOVA and Bonferroni, Mann–Whitney, χ2 and Kruskal–Wallis H in SPSS. Relative risk (RR) of falls was also calculated. Significance was set at p<0.05.
Results
Prevalence of falls
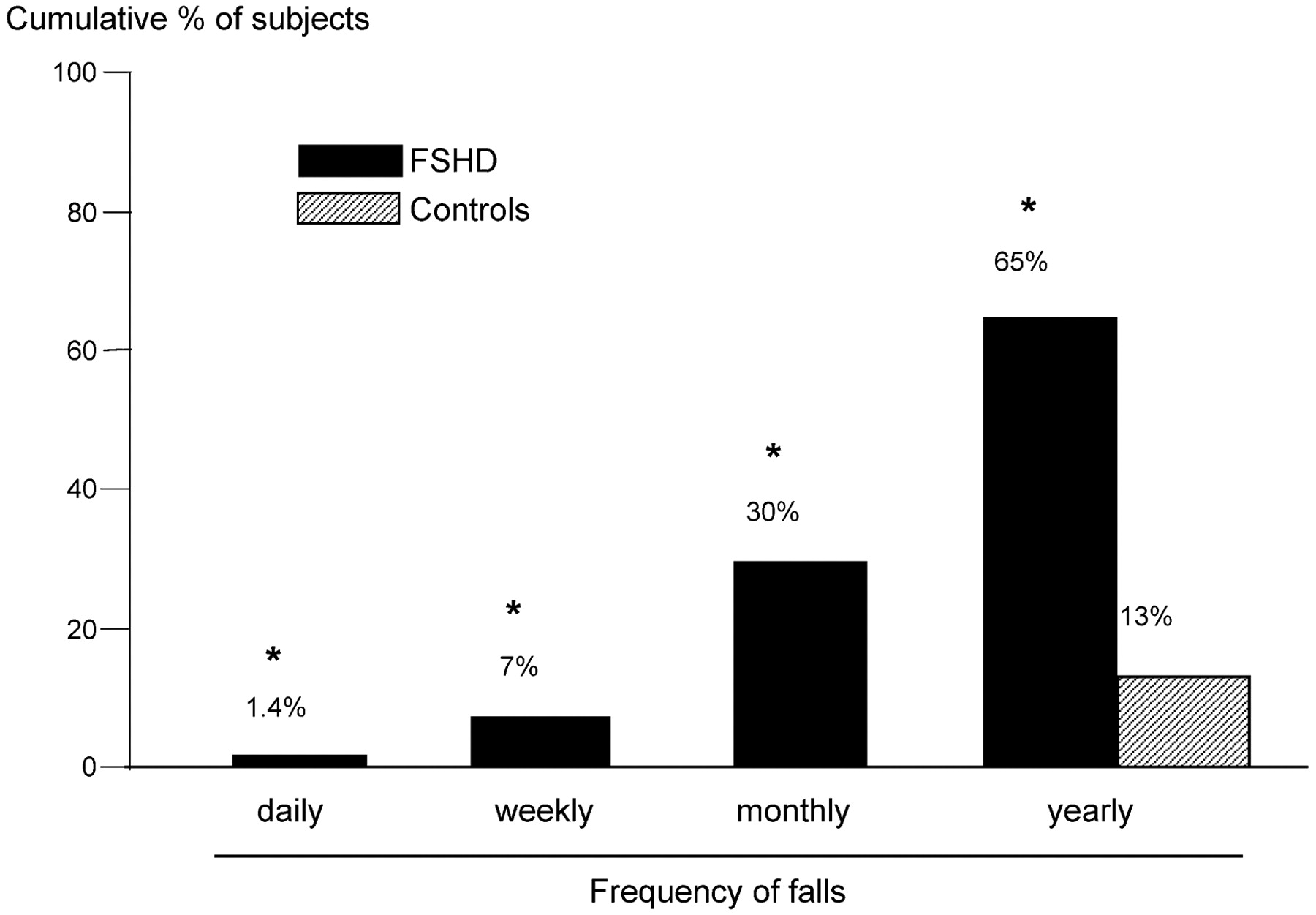
Falls occurred significantly more often in FSHD patients than in controls. In the retrospective questionnaire, 30% of the patients reported having at least one fall a month whereas none of the controls reported monthly falls (fig 1). Sixty-six per cent of the patients suffered at least monthly near falls compared with 6% of controls (p<0.05). Stumbles occurred at least monthly in 57% of patients and in 9% of controls (p<0.05).

Retrospective falls in facioscapulohumeral disease (FSHD). Bar graphs depict the cumulative percentage of patients with FSHD and controls and their frequency of falls as reported in the questionnaire. Note that none of the controls reported a frequency greater than once a year. *p<0.05 FSHD versus controls.
During the 13 week prospective follow-up, 34 patients (47%) reported 104 falls and four controls (8%) reported 11 falls. The proportion of patients who reported at least one fall was much higher than that of controls (RR 5.8; 95% confidence interval (CI) 2.2 to 15.3; p<0.05). Also, a much higher proportion of patients (26%) than controls (4%) suffered multiple falls (RR 5.3; 95% CI 1.3 to 21.9; p<0.05). The RR of suffering at least one fall during follow-up when falls were reported in the questionnaire (at least monthly falls and/or monthly near falls) was 3.11 (95% CI 1.48 to 6.54; p<0.05).
Clinical relevance of falls
Sixty-nine per cent of patients and 57% of controls reported sustaining one or more injuries from a fall at some point in time (p = 0.253) according to the retrospective questionnaire. Thirty-four per cent of patients and 16% of controls reported severe injuries. Patients reported approximately 3.5 times more injuries due to falls than controls, while the proportion of patients (69%) and controls (57%) who had experienced an injurious fall hardly differed. This discrepancy can be explained by the number of multiple injuries in patients. Only 4.3% of controls suffered three or more injuries compared with 23% of patients (p<0.05). More than half of the patients (51%) reported fear of falling compared with 7% of controls (p<0.05). Due to their fear of falling, 35 patients (49%) and two controls (4%) reported reducing their participation in certain activities (p<0.05). Most of the patients reported having stopped participating in sports and bicycling, and some reported having stopped walking, gardening, housework, shopping or leaving the house for pleasure activities. Control subjects only mentioned having stopped doing extreme sports, such as skiing.
During prospective follow-up, similar results were seen; 67% of the patients reported one or more injuries as a result of falling and six patients (18%) reported multiple injurious falls. Controls all suffered at least one injurious fall and two reported multiple injurious falls. Major injuries that occurred among patients were fracture of the metacarpal bones, and three head skin wounds. One control suffered a rib contusion. All controls were able to get up by themselves after they had fallen whereas 24% of patients could not get up without help and 12% needed help occasionally. The results of one patient were missing.
Fall circumstances
The most common direction of falling could be specified by 39 patients in the questionnaire: 72% of these reported falling forwards. During follow-up, most patients (41%) fell in a forward direction also. For controls, the direction of falls varied with each fall. In the questionnaire, most patients did not report a common time of day of falling (81%). During follow-up, the time varied in 35% of patients: 26% reported falling in the afternoon, 21% in the morning and 9% in the evening. Only three controls specified a moment of falling, each at a different time of day. In the questionnaire, 35 patients and 17 controls specified a location for their falls; 39% of these patients reported falling mostly at home while none of the controls did (p<0.01). Also, during follow-up, the largest proportion of patients (33%) always fell at home. During follow-up, most patients (41%) suffered falls with an intrinsic cause. Controls always fell as a result of environmental hazards (six during skiing, three during ice skating, one on a slippery surface and one over the leg of a bed) compared with 32% of patients (p<0.05).
Pathophysiology
Characterising balance
Two frequent fallers were unable to climb stairs and were omitted from evaluation. Figure 2A shows individual trunk sway angle traces in the pitch and roll plane for a control subject, an infrequent FSHD faller and a frequent FSHD faller while climbing stairs. The frequent faller showed greater trunk sway angle in the pitch and roll direction compared with the infrequent faller and the control subject. A significant difference in sway angle was found between the frequent fallers and controls in the pitch direction and in the roll direction between frequent fallers and the two other groups (fig 2B). There was no significant difference in task duration.

Trunk sway during static and dynamic balance tasks. The upper three graphs (A) represent sway angle traces in the roll (grey lines) and pitch (black lines) directions while climbing stairs for an individual frequent faller with facioscapulohumeral disease (FSHD), an infrequent FSHD faller and a healthy control subject. Bar graphs (B) represent the mean (SEM) of trunk sway angle for FSHD infrequent and frequent fallers and healthy controls when climbing stairs (B) and get up and go (C). For the stance tasks, standing on a firm surface with eyes closed (D) and standing on foam with eyes closed (E), trunk angular velocity is given as a measure of balance. *p<0.05, frequent fallers versus controls, ‡p<0.05, frequent versus infrequent fallers.
For get up and go, one frequent faller was unable to get up without help and was omitted from the analysis of this test. Trunk sway in the pitch and roll directions was lowest for the controls and highest for the frequent fallers (fig 2C). The differences in trunk sway between frequent fallers and controls were significant for roll velocity (p<0.05) and pitch velocity (p<0.05). No significant differences in task duration for this task were found or for the timed get up and go test.
Mean duration of standing on a firm support with eyes closed for frequent fallers was significantly shorter than for controls and infrequent fallers (14.5 s for frequent fallers vs 20 s for infrequent fallers and controls; p<0.05). The pitch sway velocity was significantly increased for frequent fallers compared with infrequent fallers and controls (p<0.05) (fig 2D).
Significant differences in duration for standing on foam with eyes closed between frequent fallers and the two other groups (10.3 vs 20 s; p<0.01) were apparent. The sway angular velocities in controls and infrequent fallers were similar (fig 2E) but roll velocities were greater in frequent fallers compared with controls (p<0.05), and pitch velocities were increased for frequent fallers compared with the two other groups (p<0.05).
There were no significant differences between the three groups for the remaining tasks: standing on one leg, standing on foam with eyes open and tandem gait.
Influence of muscle weakness on falls
Figure 3 gives a schematic figure for the muscle weakness found in a frequent faller, who fell seven times during follow-up (fig 3A), and an infrequent faller, who did not fall during follow-up (fig 3B). The mean and median MRC scores of the distal and proximal joint movements are given in table 2.

Muscle weakness in infrequent and frequent fallers. The schematic figures depict the Medical Research Council (MRC) scores of several muscles (prime movers of the joint movement tested) for an individual infrequent and frequent faller with facioscapulohumeral disease (FSHD).23
Mean and median MRC scores for frequent and infrequent fallers
In the questionnaire, 94% of the patients reported having some degree of lower limb muscle weakness while none of the controls did. More than 70% of the patients reported moderate or severe weakness and 29% little or no weakness. Figure 4 reports the RR for functional weakness and subjective performance on the functional tasks versus fall, near fall and stumble frequencies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative risks (RR) of falls, near falls and stumbles versus functional weakness. Plots represent RR and 95% CI for falls, near falls and stumbles for functional weakness and the various functional tasks reported in the questionnaire. Muscle weakness: “considerable” or “little to no” weakness, as reported in the questionnaire; Chair: ability to get up from a chair; Stairs: ability to walk stairs; Toes: ability to stand on the toes for 5 s; Heels: ability to stand on heels for 5 s. Each of these tasks was scored “with difficulty” or “with ease”. Note the difference in scales for fall frequency versus near falls and stumble frequency. *p<0.05.
Discussion
This study showed that falling is a prevalent and clinically relevant problem among patients with FSHD. Retrospectively, 65% reported at least yearly, and 30% at least monthly, falls whereas 47% of the patients suffered a fall during the 13 week follow-up. To our knowledge, this is the first study concerning falls among FSHD patients. In our FSHD population, having experienced falls in the past (according to the questionnaire) increased the risk of experiencing falls during follow-up more than threefold.
The high prevalence of falls and the high rate of reported unfavourable consequences indicate the clinical relevance of falls in FSHD patients. Sixty-nine per cent of our patients reported sustaining an injury following a fall at some point in their lives. Patients reported 3.4 times more multiple injuries than controls and had significantly more severe injuries (34% vs 17%). During follow-up, 26% of the patients experienced injurious falls. The fact that 24% of the patients could not get up after falling underlines the clinical relevance even more. Fear of falling was reported by 51% of patients; consequent reduction of activities by 49% (compared with 6% and 4% among controls). It has been shown that fear of falling increases the fall frequency, creating a vicious circle.7 On the other hand, reduction of activities may lead to decreased fall frequency because of a reduced risk exposure.24 Lack of correction of the fall frequency for activity level is a weakness of this study.
Fall circumstances were determined. In the follow-up and the questionnaire, most patients reported falling at home whereas none of the controls did. This may simply reflect the fact that patients were more housebound than controls but it also emphasises the importance of the home environment in fall aetiology. Home adaptation should play an important role in preventing falls in FSHD patients. Most patients reported falling forwards. Awareness in patients and clinicians of the risk of forward falls might prevent falls in the future, for example by teaching patients to use more knee bending to maintain balance. It has already been shown that voluntary knee bending can be incorporated into automatic balance correction responses after forwards perturbations.25 The activities during which patients most frequently fell, during follow-up, were often linked to fatigue (ie, after strenuous activity, standing for a long period of time and standing on one leg). Indeed, fatigue is increased in FSHD patients and part of the clinical spectrum.26 Research from our group also reported that lower muscle strength contributed to lower levels of physical activity, which, in turn, contributed to fatigue severity.18
According to the muscle strength assessment, FSHD patients who fell regularly had significantly lower muscle strength than infrequent fallers. An association between muscle weakness and falls is apparent which support findings in previous studies.11 12 The findings in the questionnaire also support this and show that walking stairs and standing on heels may be good measures to predict increased fall risk in FSHD patients. However, it should be noted that these basic tasks do not examine muscle strength exclusively. A combination of muscle strength, dynamic balance and adequate range of motion of the lower extremities are necessary to perform these tasks.27 It should also be noted that self-reported weakness might have been biased by fall frequency; for example, those with high fall frequencies might be prone to report more weakness. Objective assessment of muscle strength and performance on functional tasks is a more reliable method for determining fall risk.
The balance assessment showed that fallers were specifically more unstable during walking stairs, getting up from a chair and standing with eyes closed. Thus increased fall risk can be expected during these activities because balance measurements have been shown to distinguish fallers from non-fallers (eg, in Huntington’s disease4 or the elderly28 29). Patients and clinicians should be aware of this increased fall risk, and prevention strategies should focus on these specific activities. For example, handrails on stairs, or a stair elevator, might prevent falls. Moreover, balance measures might be a useful means of identifying FSHD patients at risk of falling. The lack of differences for the other tasks may be the result of greater variability in trunk sway; a consequence of increased difficulty of balance tasks within small groups. These tasks appeared unsuitable for distinguishing between FSHD fallers and infrequent fallers or controls in this study. But studies in a greater number of patients may reveal differences in more detail.
The influence of the pattern of muscle weakness (distal versus proximal) could not be differentiated in this patient population because many patients had both distal and proximal weakness. Moreover, we did not investigate the influence of asymmetry of muscle weakness on balance control. Studies in larger number of patients suffering from pure distal versus pure proximal weakness and with specific patterns of weakness (symmetric versus asymmetric) will increase knowledge on the influence of muscle weakness on the pathophysiology of falls.
It would be interesting to compare our findings with fall frequencies in other neuromuscular disease populations but this remains difficult because prospective epidemiological studies on falls in patients with neuromuscular disease are rare (reviewed by Horlings and colleagues11). Comparing rates of falls and the mechanisms leading to falls in different types of neuromuscular diseases may also shed light on the underlying pathophysiology, and further pinpoint the role of the peripheral nervous system in normal balance control.
Conclusion
In conclusion, falling is a common and clinically relevant problem among patients with FSHD. Falling is related to muscle weakness. Patients fall mainly due to intrinsic causes in a forward direction, and often fall at home. An increased fall risk can be expected during walking stairs, getting up from a chair and when the eyes are closed (or in the dark). Our findings highlight the clinical importance of falls in FSHD patients, the need for increased awareness of both the clinician and the patient in this matter, and the need for fall prevention strategies, for example to train patients in using different balance strategies.
Acknowledgments
We thank all patients and control subjects for participating in this study.
REFERENCES
Supplementary materials
Lay Summary 80/12/1357
Files in this Data Supplement:
Footnotes
Funding BRB was supported by NWO VIDI grant 016.076.352. JHJA was supported by the Swiss National Research Fund grant 32-117950/1.
Competing interests None.
Ethics approval The study was approved by the ethics committee of the Radboud University Nijmegen Medical Centre.
Provenance and Peer review Not commissioned; externally peer reviewed.