Article Text

Abstract
Objectives: To gain an improved understanding of fatigue in Parkinson disease (PD) by exploring possible predictors among a wide range of motor and non-motor aspects of PD.
Methods: 118 consecutive PD patients (54% men; mean age 64 years) were assessed regarding fatigue, demographics and a range of non-motor and motor symptoms. Variables significantly associated with fatigue scores in bivariate analyses were used in multiple regression analyses with fatigue as the dependent variable.
Results: Fatigue was associated with increasing Hoehn & Yahr stages, specifically the transition from stages I–II to stages III–V. Regression analysis identified five significant independent variables explaining 48% of the variance in fatigue scores: anxiety, depression, lack of motivation, Unified PD Rating Scale (UPDRS) motor score and pain. Gender, age, body mass index, PD duration, motor fluctuations, dyskinesias, symptomatic orthostatism, thought disorder, cognition, drug treatment, sleep quality and daytime sleepiness were not significantly associated with fatigue scores. When considering individual motor symptom clusters instead of the UPDRS motor score, only axial/postural/gait impairment was associated with fatigue.
Conclusions: This study found fatigue to be primarily associated with symptoms of depression and anxiety, and with compromised motivation, parkinsonism (particularly axial/postural/gait impairment) and pain. These results are in agreement with findings in other disorders and imply that fatigue should be considered a separate PD entity differing from, for example, excessive daytime sleepiness. Fatigue may have a distinguished neurobiological background, possibly related to neuroinflammatory mechanisms. This implies that novel treatment options, including anti-inflammatory therapies, could be effective.
Statistics from Altmetric.com
Fatigue can be defined as an overwhelming sense of tiredness, lack of energy and feeling of exhaustion.1 It is a common symptom in chronic conditions, including many brain disorders.1 2 In Parkinson disease (PD), fatigue has been reported in up to two-thirds of patients, of whom many consider it one of their most disabling symptoms; yet it often goes undetected, has an unclear cause and lacks specific therapy.3 Studies have shown partly conflicting results regarding the association between fatigue and other disease aspects, such as parkinsonian and depressive symptoms.4–6 However, no such study to date has taken a broader range of motor and non-motor aspects of PD into consideration, and most rely on bivariate analyses. Here we sought to gain an improved understanding of fatigue by exploring possible predictors among a wide range of motor and non-motor aspects of PD.
METHODS
Patients
A total of 118 consecutive people with PD were included (for details, see Hagell et al7). Exclusion criteria were participation in other ongoing studies, ongoing infections, psychiatric adverse drug reactions and other clinically significant comorbidities (eg, depression, cognitive impairment, arthritis), as determined by patients’ attending neurologist and the study assessor. This was done to avoid cases with fatigue of alternate aetiologies. All participants provided signed informed consent.
Procedures and data collection
Patients were assessed during the “on” phase using the Unified PD Rating Scale (UPDRS), the Hoehn & Yahr (HY) staging of PD and the Mini-Mental State Exam (MMSE). HY stages were also estimated for the “off” phase from patient-reported history and medical records. The inter-rater concordance (Kendall W) among study assessors for UPDRS and HY ratings was ⩾0.85. UPDRS part III (motor score) was used as an overall measure of parkinsonism. In addition, the following symptomatic profile scores were calculated: axial/postural/gait impairments (items 18, 19, 27–31), rest tremor (item 20), postural tremor (item 21), rigidity (item 22) and limb bradykinesia (items 23–26).8
The Functional Assessment of Chronic Illness Therapy—Fatigue (FACIT-F)9 scale was used to measure fatigue. To ease interpretation relative to other variables, FACIT-F scores (range 0–52) were reversed in this study (0 = less fatigue). Sleep quality was assessed with the Pittsburgh Sleep Quality Index, daytime sleepiness by the Epworth Sleepiness Scale, depression and anxiety with the Hospital Depression and Anxiety Scale, and pain by the Pain scale of the Nottingham Health Profile (NHP). All patient-reported scales were completed during the “on” phase, and their reliabilities (coefficient alpha) were ⩾0.71.
Patients classified as fatigued according to the Energy scale of the NHP7 were asked whether their fatigue typically was worse when “on” or “off,” if their motor symptoms were worse when they experienced fatigue, and whether they had experienced fatigue prior to the onset of motor PD symptoms.
Analyses
Data were checked regarding underlying assumptions, and described and analysed accordingly using SPSS version 14 (SPSS, Chicago). The alpha-level for significance was set at 0.05 (two-tailed). Variables significantly associated with fatigue scores in bivariate analyses were entered as independent variables in regression models with fatigue (FACIT-F) as the dependent variable. First, the total UPDRS motor score was entered as an independent variable to assess the association between parkinsonism and fatigue. Second, the five UPDRS motor symptom profile scores were entered instead to explore whether fatigue appears associated with any particular aspect(s) of parkinsonism.
RESULTS
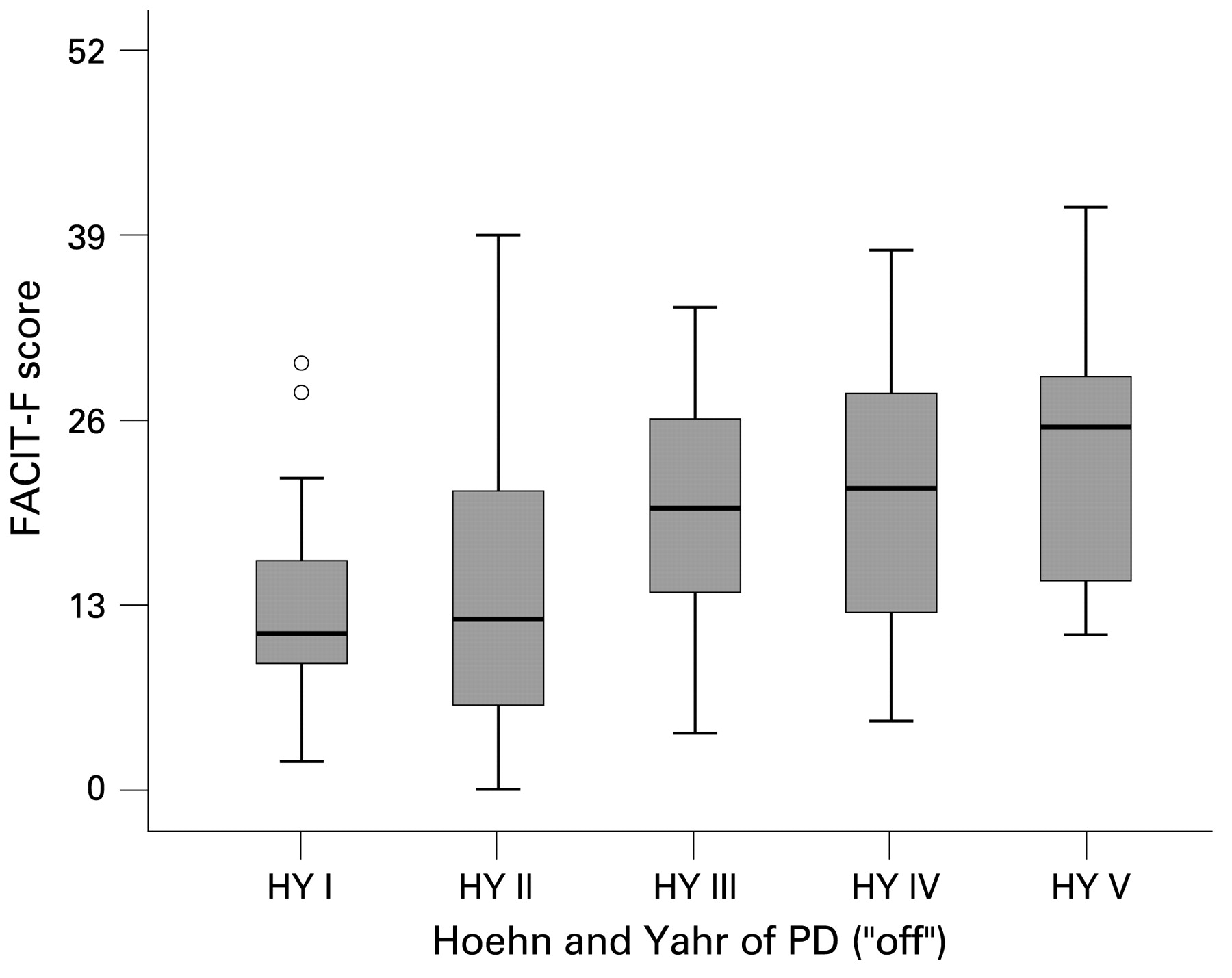
The sample consisted of 64 (54%) men; the mean (SD) age and PD duration were 63.9 (9.6) and 8.4 (5.7) years, respectively (see supplementary table S1 online). Among 57 (48%) fatigued participants, 42 (74%) experienced worsening of motor symptoms while fatigued. Thirty (53%) of the 57 fatigued patients experienced motor fluctuations. Of these, 25 (83%) reported that their fatigue was worse during “off.” Eighteen patients (32%) reported that their fatigue had begun prior to motor symptom onset. Fatigue scores increased across “off” phase HY stages (fig 1).
{kind=link}
Functional Assessment of Chronic Illness Therapy—Fatigue (FACIT-F) scores across “off” phase Hoehn & Yahr (HY) stages (higher scores = more fatigue). The Kruskal–Wallis test showed significant differences across HY stages (p = 0.005), and post-hoc Mann–Whitney U tests indicated a significant difference between HY stages II and III (p = 0.04 following Bonferroni correction) but not between other stages. Solid horizontal lines are median values, boxes are interquartile ranges (25th to 75th percentiles), and error bars are ranges. Open circles are outliers, defined as values >1.5 box lengths from the 75th percentile. PD, Parkinson disease.
The first regression model constructed based on bivariate analyses of associations between fatigue and other variables (see supplementary tables S2 and S3 online) identified five variables explaining 48.2% of the variance in fatigue scores (table 1). The strongest predictors were symptoms of anxiety, depression and impaired motivation. When the total UPDRS motor score was substituted with the five motor symptom profile scores (model 2), only axial/postural/gait impairment was associated with fatigue (table 1).
DISCUSSION
This study sought to improve the understanding of fatigue in PD by exploring potential predictors of fatigue among a range of motor and non-motor aspects of PD. We found fatigue to be associated with symptoms of depression, anxiety, compromised motivation, parkinsonism and pain. When considering individual motor symptom clusters, axial/postural/gait impairment (but not tremor, rigidity or bradykinesia) was found to be associated with fatigue.
We excluded patients with comorbidities such as depression. This may pose some limitations to the generalizability of results—for example by underestimating the role of depression. Since fatigue is common in major depression, and depression is common in PD, including depressed patients could have increased the predictive value of depression for fatigue. It should also be kept in mind that several of our variables were coarse single item ratings, and no laboratory measures were included. However, a major strength of this study is its comprehensiveness in terms of the number of variables considered. As such, this appears to be the first study of its kind in PD.
In contrast to what has been documented before in PD, we found that anxiety was a stronger predictor of fatigue than depression. Lack of motivation was also identified as a significant predictor of fatigue. This is in accordance with previous hypotheses suggesting that central motivational processes are important contributors to the experience of fatigue in neurological disorders.2 Taken together, anxiety, depressive symptoms and lack of motivation could predict about 42% of the variation in fatigue scores.
We found an association between fatigue and the underlying severity of parkinsonism. However, when considering individual symptom clusters, only axial/postural/gait impairment was associated with fatigue (despite no overt signs of multicollinearity). Accordingly, fatigue scores primarily appear to worsen in HY stages III (ie, when postural symptoms appear) and above. Similarly, Alves et al found fatigued PD patients to exhibit worse UPDRS motor scores and have more postural instability and gait difficulties than non-fatigued patients.5 Together with the observed lack of association with dopaminergic drug treatment and indications of more dysautonomy in fatigued patients, this could suggest involvement of extrastriatal pathology in the development of fatigue. Accordingly, a recent study among people with dopa-naïve PD found fatigued patients to have more severe parkinsonism but similar striatal dopamine transporter uptake compared with non-fatigued patients.10 Interestingly, we found that parkinsonism was associated with fatigue but only explained an additional 3.6% of its variance once the influence of anxiety, depressive symptoms and reduced motivation had been taken into account. Furthermore, while dopaminergic drugs can help improve fatigue,10 we failed to see any association between fatigue and dosages of antiparkinsonian medications. Taken together, fatigue does therefore not seem to be a direct consequence of the nigrostriatal dopaminergic pathology in PD.
We found indications that fatigue cannot be explained by excessive daytime sleepiness (EDS) or poor sleep. This is in accordance with previous work in PD,3 and other populations.11 The wake-promoting agent modafinil has been used for both fatigue and EDS.12 However, randomised controlled trials (RCTs) using the substance to treat fatigue have largely yielded negative or inconclusive results.12–15 However, when used to treat EDS in PD, results have appeared more encouraging.16 The distinction between fatigue and sleepiness may therefore have important implications, neurobiologically as well as in terms of symptom management.
Fatigue is common in inflammatory and infectious conditions. The combination of symptoms such as fatigue, depressed mood, pain and social withdrawal experienced during severe infections is often referred to as “sickness-behaviour.”17 Interestingly, this syndrome is similar to predictors for fatigue identified here and elsewhere.18 19 Chronic fatigue syndrome (CFS) has been found associated with hypocortisolism and elevations of the proinflammatory cytokine IL-6.20 In PD, there is evidence of neuroinflammation with activation of glial cells and elevation of cytokine levels.21 Whether primary or not, a sustained low-grade neuroinflammation could represent an alternative pathology in PD leading to symptoms such as fatigue. Indeed, a recent study found plasma cytokine levels to correlate with fatigue in PD.22
It is possible that fatigue has a specific underlying pathogenesis that is common across disorders and that requires targeted therapy. Although not excluding other possibilities, one alternative could be anti-inflammatory treatment. An RCT of acetyl-salicylic acid to treat fatigue in multiple sclerosis provides tentative support for this hypothesis.23 Moreover, cyclooxygenase-2 inhibitors have been used against treatment-resistant depression with promising results24 and have been suggested for treating CFS.25
Our results show that symptoms of depression and anxiety are the main predictors of fatigue in PD. Furthermore, fatigue is associated with lack of motivation, parkinsonism and pain. We propose that fatigue should be separated from sleepiness and suggest that it may have a distinct neurobiological background requiring different, non-dopaminergic treatment strategies such as anti-inflammatory therapies.
Acknowledgments
The authors want to thank all participating patients for their cooperation; H Widner for valuable discussions; B Eriksson, A Höglund, I Knutsson and J Reimer for assistance with data collection; and J Ahlberg, N Dizdar, H Edwall, B Johnels, J Lökk, S Pålhagen, H Widner and T Willows for patient recruitment.
REFERENCES
Supplementary materials
Web only appendices 80:5;489-93
Files in this Data Supplement:
Footnotes
-
Supplementary tables are published online only at http://jnnp.bmj.com/content/vol80/issue5
-
Funding: The study was supported by the Swedish Research Council, the Swedish Parkinson Foundation, the World Federation of Neuroscience Nurses, the Skane County Council Research and Development Foundation, the Vårdal Institute and the Faculty of Medicine at Lund University.
-
Competing interests: None.
-
Ethics approval: The study was approved by the Research Ethics Committee, Faculty of Medicine, Lund University, Sweden.
-
Patient consent: Obtained.