Article Text

Abstract
Objective To investigate salivary cortisol samples in patients with Parkinson's disease (PD) with and without impulsive compulsive behaviours (ICB) during a risk task.
Methods Salivary cortisol levels were measured in 13 PD patients without ICB (PD−ICB) and in 15 PD patients with ICB (PD+ICB) before, after medication and throughout the day, and were compared with results with 14 healthy controls. All participants also performed a gambling task to assess risk taking behaviour.
Results Significantly higher diurnal cortisol levels were found in the PD−ICB group compared with healthy controls but no differences were seen between the PD+ICB and the control group. Increased cortisol levels were significantly correlated with increased risk taking in PD+ICB patients but no interaction was found in the PD−ICB group.
Conclusions The findings are in keeping with previous studies which have linked low cortisol levels with antisocial behaviour. The higher cortisol levels during the risk task in the PD+ICB group are consistent with reports in pathological gamblers during gambling and addicts during drug abuse. The results support the hypothesis that cortisol plays an important role in risk taking in ICBs.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
The cause of Parkinson's disease (PD) remains unknown but acute severe stress has been suggested as a possible precipitant.1 Elevated cortisol levels in animal models of PD have been associated with dopaminergic cell loss and motor handicap.2 Higher cortisol levels have been described in depression,3 anxiety4 and also in Alzheimer's disease and PD.5 An acute increase in cortisol levels has been reported during intake of illicit drugs.6 Although a large proportion of addiction related research has highlighted the importance of dopaminergic pathways,7 there is also a line of evidence supporting the role of cortisol in the development of addictive or impulsive behaviours.8 9
A subgroup of PD patients develop impulsive compulsive behaviours (ICB) which are associated with antisocial behaviour.10 ICBs are usually triggered by dopamine agonist therapy and there is growing evidence linking the aetiology of these ICBs to the development of drug addictions.11 12 Previous studies have found lower cortisol levels in impulsive non-PD participants.13 14 Given the link between cortisol and addiction in healthy subjects, and between addiction and the development of ICBs in PD patients, we hypothesised that cortisol levels might be reduced in PD patients with ICBs, relative to PD patients without ICBs.
For this study, we measured salivary cortisol levels from PD patients with (PD+ICB) and without (PD−ICB) ICBs, and healthy controls, and correlated these results with their performance on a risk task.15 Increased salivary cortisol levels have also been positively correlated with risk taking in non-PD pathological gamblers.16 Therefore, we sought to correlate cortisol with risk taking behaviour, having previously shown increased risk taking in gambling tasks in all PD patients on medication compared with controls, with highest risk taking behaviour in PD patients with pathological gambling.17
Methods
Participants
Cortisol samples from 13 PD−ICB, 15 PD+ICB patients and 14 healthy controls were collected. All patients were recruited from the National Hospital for Neurology and Neurosurgery, Queen Square, London, fulfilling the Queen Square Brain Bank criteria for PD18 and were taking L-dopa. PD+ICB patients were diagnosed using proposed criteria.19–21 Most PD+ICB patients had more than one ICB. Healthy controls were usually recruited from among the patient's partners and were not taking any medication that could influence cortisol measurement. None of the participants was taking steroids. Written informed consent was obtained from all subjects according to approved ethical protocols from the regional and local research ethics committee.
We excluded participants who scored under 27/30 points on the Mini-Mental State Examination and who had a current or past medical history of an anxiety disorder, and patients with current depression. Patients without a known previous diagnosis of anxiety or depression were screened for these conditions in a semi-structured clinical assessment. Furthermore, all participants were asked to complete the positive and negative affect schedule which has been recommended as a supplement to measure anxiety and depression.22 Samples were obtained in a quiet environment, usually at the patient's home, to control for and reduce the amount of stress.
To control for the potential effects of food23 and L-dopa24 on cortisol levels, PD patients were asked not to take their usual anti-Parkinson medication for at least 12 h and not to have breakfast on the day of testing. All participants woke up between 6:00 and 7:00. The morning samples were obtained together with the researcher and the other samples were collected by the participants themselves.
Cortisol
Participants were instructed to collect saliva samples by turning the cotton roll for 2–3 min in their mouth. In total, five saliva samples were collected from controls and 10 samples from patients. Samples from all participants were obtained between 8:15 and 8:45—baseline level. All patients were tested in their ‘off condition’ in the morning, which was assessed by the Unified Parkinson's Disease Rating Scale (UPDRS) part 3 motor score. Furthermore, we collected five more saliva samples from the patient group. One was obtained immediately prior to the risk task, one just after the risk test and prior to medication, the next 5 min after medication, then 15 min after medication, 30 min after medication and 45 min after medication. Sixty minutes after medication, between 9:15 and 9:45 and after the second test (‘on condition’ in patients), another sample was taken, this time from both controls and patients (figure 1).

Schematic outline of the time course of saliva samples. Ten samples were taken from Parkinson's disease (PD) patients prior to medication (‘off’) and after medication (‘on’). Five samples were obtained from controls.
All participants then collected samples between 13:00 and 14:00, between 19:00 and 20:00 and between 22:00 and 23:00 on their own. These times were deliberately flexible for patients to ensure that the cortisol sampling was undertaken approximately 1 h after taking their usual dopamine replacement therapy. Controls were tested in the same way without taking any medication in between.
Subjects were asked to avoid excessive physical activity, stress and heavy meals on the study day, and were provided with a collection diary where they entered the time of saliva collection and their activity during the hour prior to each cortisol sample. In addition, participants were instructed not to eat anything at least 30 min prior to collecting a sample.
The therapeutic motor response to L-dopa was assessed by UPDRS scores (part 3) during ‘off’ and ‘on’ states. All patients had an excellent L-dopa response and had a similar improvement in UPDRS scores. All patients were ‘on’ at the time of the second risk task. Levodopa equivalent units (LEU) was calculated as described previously21 (see table 1 for demographic information).
Characteristics of patients and healthy controls
Risk task
All patients were tested on a validated computerised gambling task to assess risk behaviour15 once in their ‘off medication’ state after their first salivary cortisol sampling, and once in their ‘on medication’ state approximately 50 min after receiving their usual morning anti-Parkinson medications. Controls were tested in the same way but did not take dopaminergic medication between the tests. Participants had to choose between two gambles with varying levels of risks—either a low risk or a high risk gamble, where participants could win real money. Feedback was given immediately. Details about this task are published elsewhere.17 Risk aversion was assessed parametrically by fitting a model to each participant's behaviour, separately for each test session.17
Biochemical measurements
Saliva samples for the determination of cortisol concentration were collected in Salivettes (Sarstedt, Leicester, UK) and stored at −20°C until analysed. Details on the analysis were published recently elsewhere.25
Statistical analysis
Demographic and clinical features
Data analyses were performed using SPSS V.18. Age, gender, age of onset, UPDRS scores, L-dopa and LEU dose were used as dependent variables and group (PD−ICB, PD+ICB and control) was modelled as a between subject factor. We used ANOVA, the Student's t test or the χ2 test where appropriate.
Cortisol salivary samples
The data were positively skewed as cortisol levels show a diurnal variation with a peak during the morning (figure 2). As a result, we log transformed the data and residuals were checked and found to be normally distributed. We performed a linear mixed model ANOVA with the log transformed scores as the dependent variable and group (PD−ICB, PD+ICB and control) was modelled as a between subject factor. The model also included subject as a random factor, and the interactions between the two fixed factors (time and group). All post hoc comparisons were corrected by the Bonferroni method; the level of significance was p<0.05. For the diurnal cortisol measurement we excluded those extra samples that were obtained from the patients between the tests.
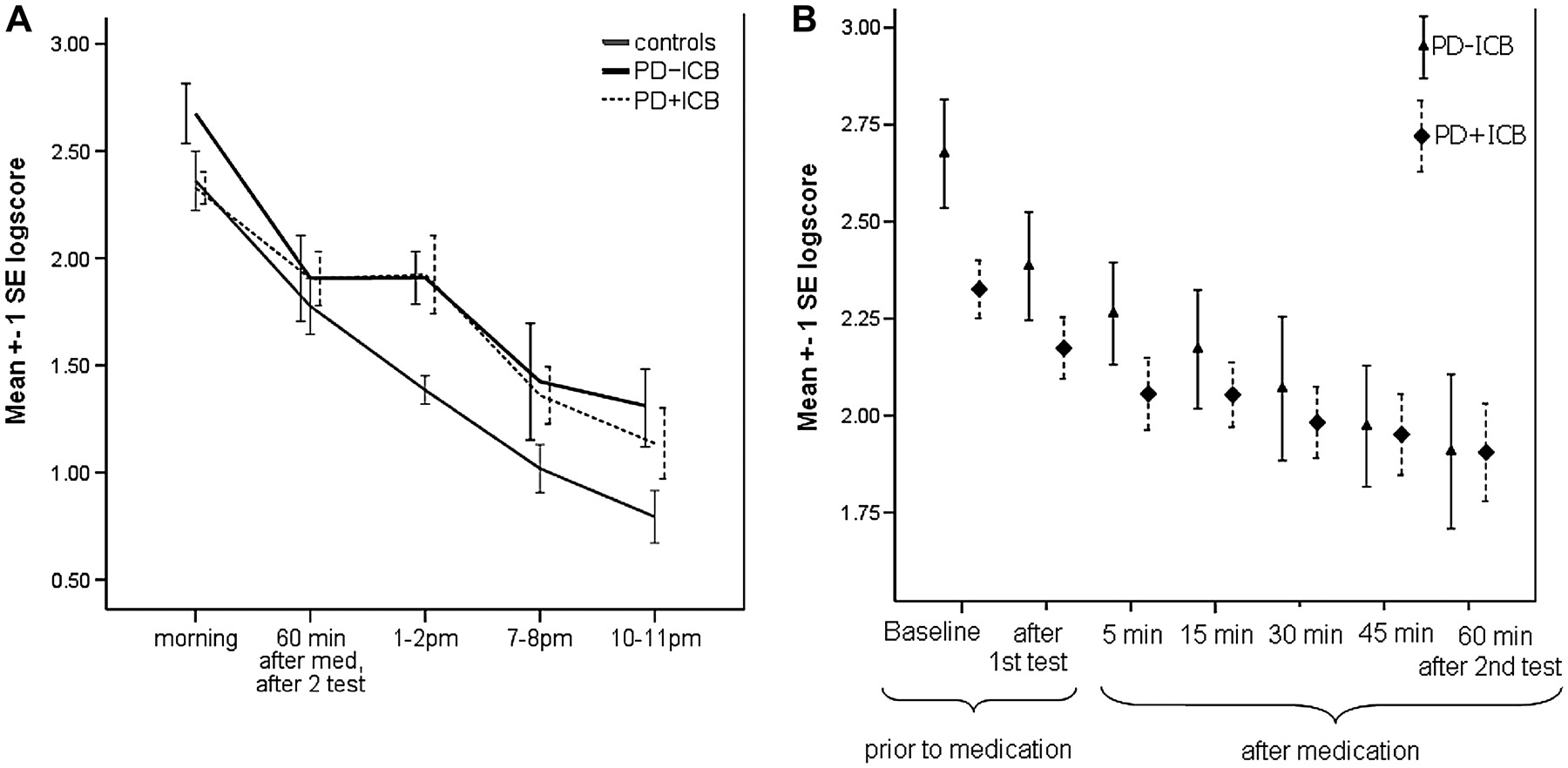
(A) Diurnal cortisol levels of all three groups. (B) Cortisol levels between Parkinson's disease patients without (PD−ICB) and with (PD+ICB) impulsive compulsive behaviour. All values are mean (±1 SE). Although not significantly different, baseline morning cortisol levels were lower in the PD+ICB group.
We correlated the change in risk aversion with the change in cortisol levels. This is a within subjects analysis. Specifically, we calculated the correlation coefficient between: ΔR and ΔC, where ΔR=R1–R2 is the difference in risk aversion in the first and second test session; ΔC was defined accordingly for cortisol levels. One value for ΔR and one for ΔC was derived for each subject, and these values were then correlated using Pearson's correlation test.
Results
Demographic characteristics
The groups were generally well matched. There was no significant age difference between the groups (F(2,38)=2.5, p=0.091). However, PD+ICB patients had an earlier disease onset (t24=2.6, p=0.014). There was no difference in the daily L-dopa doses or the dose given in the morning, LEU dose, UPDRS (part 3 motor) scores or disease duration (see table 1 for further details).
Cortisol levels
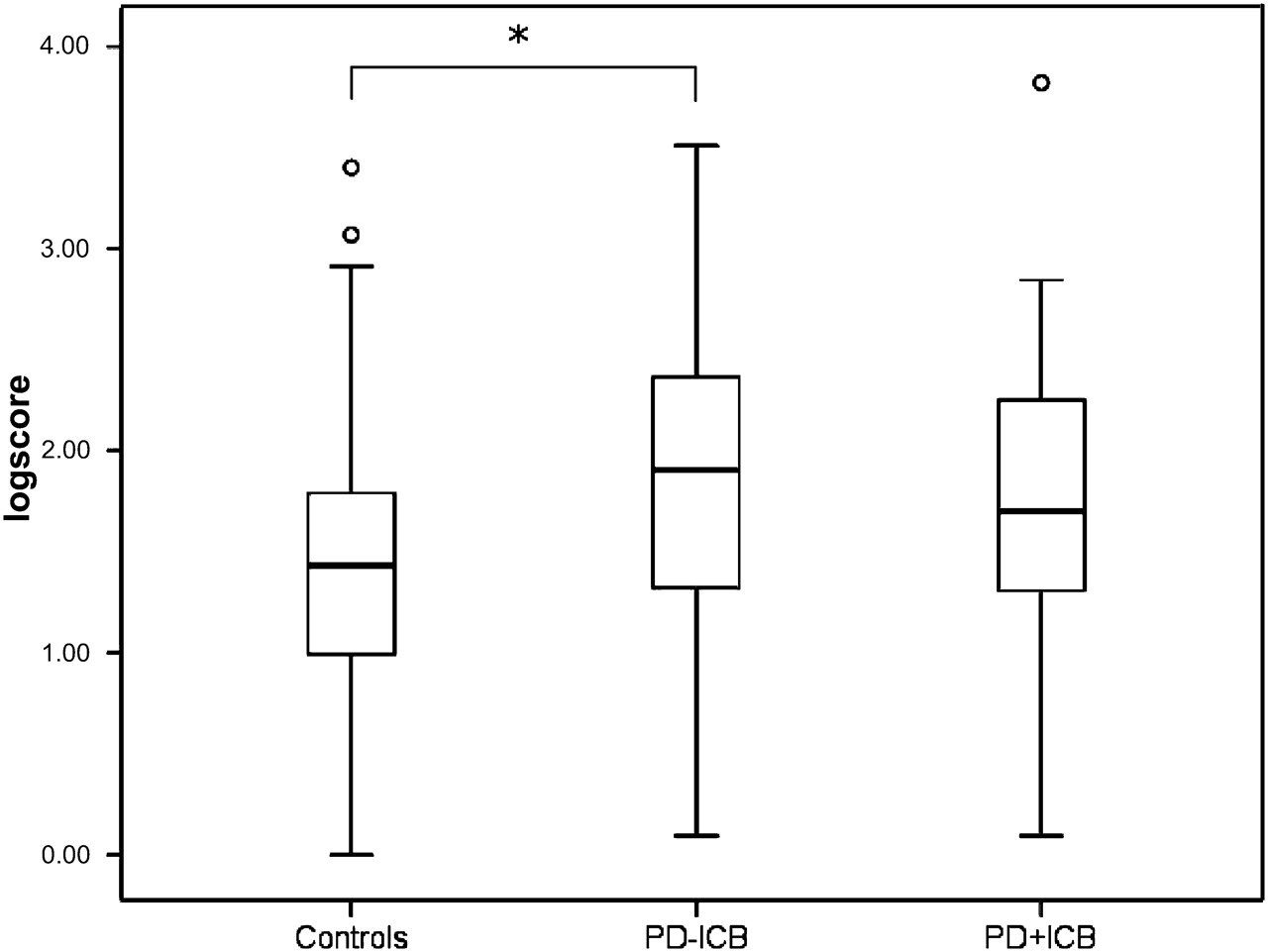
We found a main effect of group (F(2,37)=4.6, p=0.016) and a main effect of time (F(4,144)=51.0, p<0.001), with the highest cortisol level being in the morning. There was no interaction between time and group (F(8,144)=0.9, p=0.48). Post hoc analysis revealed that the PD−ICB group had significantly higher cortisol levels than the control group (p=0.019) (figure 3). There was no difference between the control and PD+ICB group (p=0.1) and no difference between the patient groups (p=1.0). We next looked at just the morning cortisol levels between the patient groups by excluding the control group but found no significant difference (t24=2.4, p=0.2). There was no correlation between UPDRS off score and baseline cortisol levels (all p values >0.4).
{kind=link}
{kind=link}
{kind=link}
Log scores of diurnal salivary cortisol levels in controls and in patients with Parkinson's disease without (PD−ICB) and with (PD+ICB) impulsive compulsive behaviour. Box plot showing the median (horizontal line) within a box containing the central 50% of the observations (ie, the upper and lower limits of the box are the 75th and 25th percentiles). Outliners are shown as a circle symbol. *Significant difference.
Risk task
Participants were tested twice on a behavioural task that assessed risk taking behaviour15 once off medication and once on medication. Cortisol samples were taken just before each administration of the task. The task assessed the extent to which participants preferred large, low probability rewards to smaller more probable rewards. We have reported detailed analyses of the behavioural results previously, the main finding being that patients became more risk prone on medication, relative to controls.17 Here we focus on the relationship between cortisol and behaviour in the task. In the PD+ICB group, there was a significant correlation between change in risk from the first to the second test session (from the off medication state to the on medication state) and change in cortisol levels measured just before each test session (r=−0.617, p=0.0144, n=15). Specifically, increased risk preference was associated with increased cortisol levels. In the PD−ICB group, the correlation was not significant (r=0.166, p=0.669, n=11). Furthermore, the correlation coefficients were significantly different between the PD−ICB and the PD+ICB groups (Z=1.99, p=0.047) such that there was a significantly stronger correlation in the PD+ICB group than in the PD−ICB group.
Discussion
As expected, cortisol levels were found to be highest in the morning in all participants and decreased over the day (figure 2). Furthermore, we found significantly higher daily salivary cortisol levels in PD−ICB patients compared with healthy controls but no difference between PD+ICB patients and controls.
Increased irritability and lability, higher scores of disinhibition and novelty seeking and a previous history of addictive behaviours have been reported in PD+ICB patients.12 26 Furthermore, all PD+ICB patients had higher schizotypy scores, which is a personality trait related to the risk for psychosis, than controls.27 In this study, it is not possible to determine whether changes in cortisol are a cause or effect of the impulsive compulsive behaviours. However, impulsiveness, carelessness and aggressive behaviour have been associated with attenuated cortisol levels in adolescents and adults.13 28–30 Impulsive adults with illicit drugs abuse,14 patients with antisocial behaviour31 32 and controls with reduced negative feedback learning33 also had lower cortisol levels. Increased temporal discounting, the tendency to choose earlier, smaller over delayed, larger rewards has been found only in PD+ICB patients27 and has been associated with attenuated cortisol levels in healthy volunteers.34 Various studies have also shown impairment in feedback learning in PD+ICB patients.17 35 36
However, we did not find any difference between the two patient groups and between the control and PD+ICB groups. Previous studies found sustained elevated cortisol levels in Aborigines after receiving their wages which they planned to gamble with.37 Therefore, the expectance of being tested and the subsequent modest monetary reward for completing the study could have led to an increase in baseline cortisol levels in PD+ICB patients. Another possible explanation is that PD itself is associated with increased cortisol levels5 while personality traits typical of PD+ICB patients are linked with lower cortisol levels. This might explain why we did not find any difference between PD+ICB patients and the two other groups. Critically, we observed a change of direction of cortisol levels only in the PD+ICB group during gambling. This change of direction in cortisol levels following a stressor has been linked with antisocial behaviour.30
We have reported previously that all PD patients were more risk prone on medication compared with controls, with a subgroup of PD+ICB with pathological gambling taking the most risky decisions.17 When correlating changes in cortisol levels with risk taking behaviour, we found a significant interaction in the PD+ICB group but not in the PD−ICB group, despite both groups showing similar performance on the risk task. Our findings are consistent with previous studies in male non-PD gamblers showing a rise in salivary cortisol levels16 38 and blood cortisol levels39 during gambling. Acutely raised cortisol has been linked with anticipation of increased chances of making money and can be euphorogenic.40 41 Alcohol and nicotine induce an increase in cortisol levels8 42 and addicts have an increased activation of the hypothalamic–pituitary–axis during drug intake.8 Several preclinical studies have also shown that cortisol acts as a positive reinforcer and causes addiction.43 Self-administration of cocaine leads to elevated cortisol levels in rodents,9 non-human primates44 and humans.45
Our findings, with a relative increase in cortisol in PD+ICB during a risk task, further strengthen the links between biological and drug addictions. This finding in a PD population is especially interesting since L-dopa has a dual effect on cortisol and behaviour. It increases risk behaviour in all PD patients17 and high doses of L-dopa can reduce cortisol levels.24 The latter finding contrasts with our results but in this study by Muller et al, a control group was not included, morning samples were obtained at a time of the day when cortisol levels decrease fastest and no information on circadian cortisol levels was provided.
To our knowledge, this is the first study that has tested salivary samples in PD+ICB patients. Our results suggest that in general, cortisol levels are elevated in PD−ICB patients compared with controls but not in the PD+ICB group. This is in keeping with the literature which links lower cortisol levels with antisocial behaviour, and further links ICBs with substance addiction. Additionally, we found a significant correlation between risk taking behaviour and cortisol levels in the PD+ICB group with higher cortisol levels being associated with risk prone behaviour but no significant interaction in the PD−ICB group.
Acknowledgments
The authors thank the patients and their families for participating. The authors also thank Irene Papadopoulos for technical assistance with the saliva cortisol assays and Professor Peter Brown for critically reading the manuscript.
References
Footnotes
BBA and AL contributed equally to this study.
Funding This work was supported in part by the Intramural Program of the National Institutes of Health, National Institute of Mental Health.
Competing interests AL serves as historical section editor for Movement Disorders; has served as a consultant to Genus; has served on advisory boards for and received honoraria from Novartis, Teva Pharmaceutical Industries Ltd, MEDA Pharmaceuticals Inc, Boehringer Ingelheim, GlaxoSmithKline, Ipsen, Lundbeck Inc, Allergan Inc, Orion Pharma UK Ltd and Eisai Inc; and has received research support from the PSP Association and the Reta Lila Weston Trust.
Ethics approval This study was conducted with the approval of the the Joint UCL/UCLH Committees on the Ethics of Human Research.
Provenance and peer review Not commissioned; externally peer reviewed.