Article Text

Abstract
Objectives To develop prognostic models for time to 12-month remission and time to treatment failure after initiating antiepileptic drug monotherapy for generalised and unclassified epilepsy.
Methods We analysed data from the Standard and New Antiepileptic Drug (arm B) study, a randomised trial that compared initiating treatment with lamotrigine, topiramate and valproate in patients diagnosed with generalised or unclassified epilepsy. Multivariable regression modelling was used to investigate how clinical factors affect the probability of achieving 12-month remission and treatment failure.
Results Significant factors in the multivariable model for time to 12-month remission were having a relative with epilepsy, neurological insult, total number of tonic-clonic seizures before randomisation, seizure type and treatment. Significant factors in the multivariable model for time to treatment failure were treatment history (antiepileptic drug treatment prior to randomisation), EEG result, seizure type and treatment.
Conclusions The models described within this paper can be used to identify patients most likely to achieve 12-month remission and most likely to have treatment failure, aiding individual patient risk stratification and the design and analysis of future epilepsy trials.
- Epilepsy
- Randomised Trials
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Around a third of people with epilepsy have generalised epilepsy, but when compared with focal epilepsy there have been few randomised controlled trials assessing treatments for generalised epilepsy. Published trials have tended to focus on one particular seizure type such as absence seizures1 ,2 or upon generalised tonic-clonic seizures and have either excluded or ignored other seizure types.3–6 No trials have so far been reported that have assessed the treatment response of differing generalised seizure types or syndromes, and no prognostic models have been reported.
Arm B of the Standard and New Antiepileptic Drug (SANAD) trial7 enlisted 716 patients where the recruiting clinician considered valproate the treatment of choice: 473 with generalised, 191 with unclassified and 52 with focal epilepsy. These patients were randomised to start treatment with valproate, lamotrigine or topiramate. Overall results indicated that valproate was the first-line treatment as it was significantly superior to lamotrigine for time to 12-month remission and significantly superior to topiramate for time to treatment failure.
The SANAD B dataset provides a unique opportunity to use prognostic modelling to investigate which clinical factors influence outcome. Prognostic models are rare in epilepsy and include those derived from the National General Practice Survey of Epilepsy,8 the Medical Research Council (MRC) antiepileptic drug withdrawal study,9 and the Multicentre study of Early Epilepsy and Single Seizures.10 Most recently, we reported a prognostic model for patients with focal epilepsy derived from the SANAD A dataset.11 A number of factors influencing treatment outcome were identified and a prognostic model produced to aid outcome prediction for individual patients. In this paper, we report prognostic modelling of data from SANAD B in order to inform prognostication and treatment decisions for patients with generalised and unclassified epilepsy.
Methods
Patients and procedures
Full details are available in the original trial report.7 In brief, patients qualified for randomisation in arm B of the SANAD study if they had a history of two or more clinically definite unprovoked epileptic seizures in the previous year and if the recruiting clinician regarded valproate the better standard treatment option than carbamazepine. Patients were randomly allocated in a 1:1:1 ratio to valproate, lamotrigine or topiramate between 12 January 1999 and 31 August 2004.
The two primary outcomes in SANAD were time to treatment failure and time to the first period of 12-month remission from seizures. Treatment failure can be as a result of inadequate seizure control or due to unacceptable adverse events.
Prognostic modelling
As in our modelling of SANAD arm A,11 we wished to determine factors that predicted time to 12- and to 24-month remission, and factors that predicted time to treatment failure, either as a result of treatment withdrawal due to adverse events or treatment addition or replacement due to inadequate seizure control. Clinical consensus and knowledge from previous prognostic studies in epilepsy12 ,13 led to the following list of potential prognostic factors: sex, febrile seizure history, first degree relative with epilepsy, treatment history (antiepileptic drug treatment prior to randomisation), age at randomisation, time from first seizure to randomisation, neurological insult (learning disabilities or a neurological deficit), total number of tonic-clonic seizures before randomisation, EEG result, seizure type and epilepsy type. EEG result was classified as normal, not done, non-specific abnormality or epileptiform abnormality (focal or generalised spikes, or spike and slow wave activity).
Seizure type and epilepsy syndrome were highly correlated as would be expected. As there is often uncertainty about the precise syndrome that a patient has, we elected to include seizure type in the prognostic models (as well as age and EEG), which is more likely to be informative for prognostication in newly diagnosed epilepsy. Also, as only 52 patients were classified as having focal epilepsy these patients have been excluded from this analysis leaving a dataset comprised of 473 patients with generalised epilepsy and 191 patients with unclassified epilepsy. Analyses, adjusted for multiple variables, used Cox proportional hazards modelling methods. Variable centring was employed to diminish multicollinearity14 and variables were examined with the likelihood ratio test.15
The proportional hazards assumption was tested and the discriminatory power and the predictive accuracy of the models were assessed using the c-statistic.16 To assess the effect of factors on the different reasons for treatment withdrawal, a competing risks analysis was required. We therefore undertook cumulative incidence analyses to assess the probability of one of the two treatment failure events occurring (inadequate seizure control and unacceptable adverse events), with covariate effects tested by Gray's method.17
Continuous variables were investigated using logarithmic and fractional polynomial transformations.18–21 Continuous variable results are illustrated as post hoc defined categorical variables with categories chosen as per spline model fit knot positions.22 Time from first seizure to randomisation contains extreme values. Therefore, people with a time from first seizure to randomisation in the first or last 1% of the variable were removed from the dataset23—this applied to 17 patients.
Results
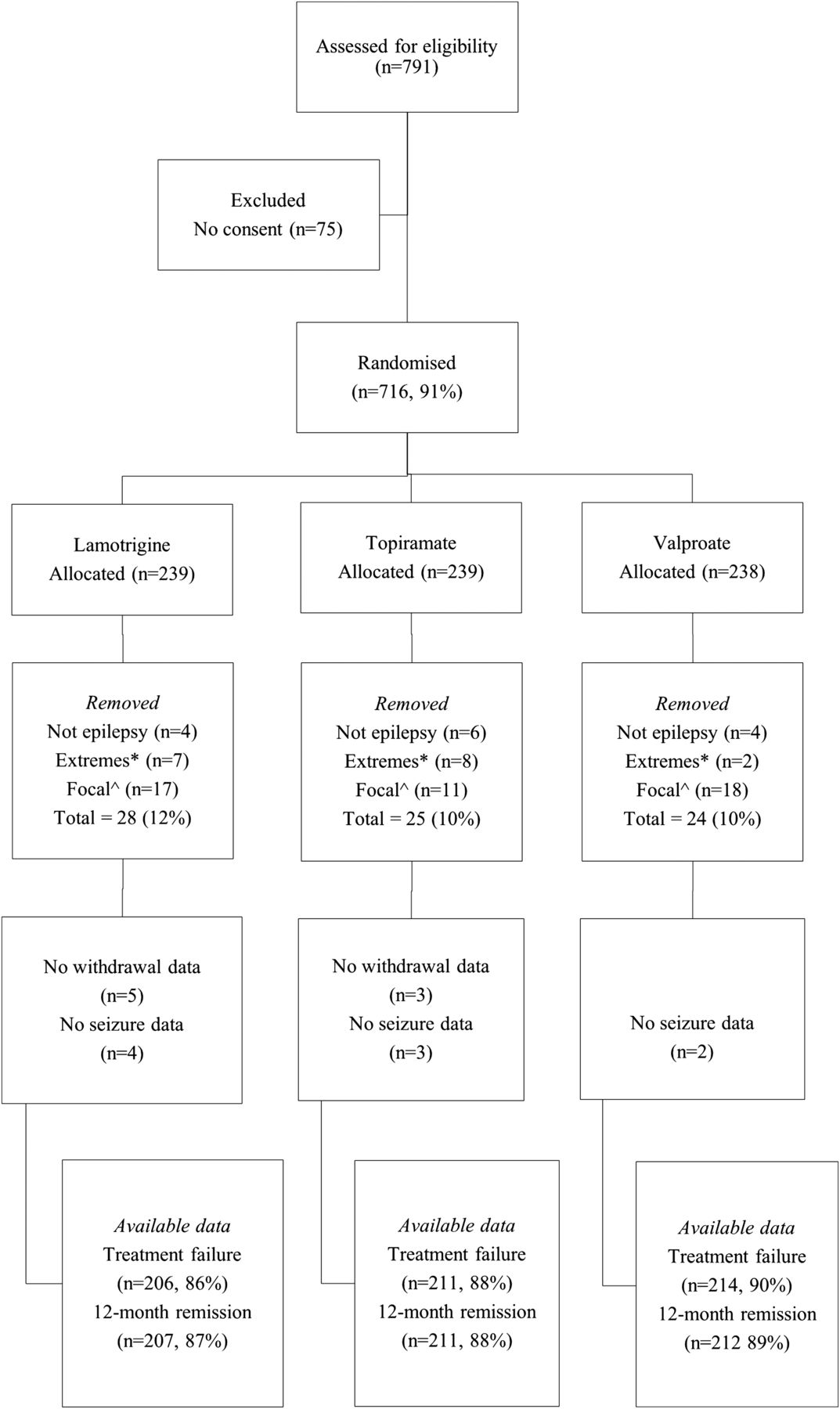
Figure 1 illustrates patient disposition for the 716 patients randomised to arm B of SANAD. Outcome data were available for 630 patients who contributed to the analysis of time to 12 months remission, 629 who contributed to the analysis of time 24 months remission and 631 patients who contributed to the analysis of time to treatment failure. Table 1 summarises the baseline demographic data for patients included in the analysis of time to treatment failure. Data were similar for time to 12 and 24 months remission (data not shown).
Baseline characteristics of patients entered into the Standard and New Antiepileptic Drug (SANAD) trial (arm B) by treatment group

Trial profile. *Patients with a time from first seizure to randomisation in the first or last 1% of the variable were removed from the dataset.23 ^Patients with focal epilepsy were removed from the analysis.
Time to 12- and time to 24-month remission
Table 2 shows results of the multivariable model for time to 12-month and time to 24-month remission (model coefficients and SEs can be seen in table 1 in the online supplementary web appendix). The c-statistic for both models was 0.7, indicating that the models accurately discriminate patients 70% of the time, which is acceptable internal validation.24 ,25 Rates of 12-month remission were significantly lower for patients with a first degree relative with epilepsy, and for those with a neurological insult. Regarding seizure types, compared with patients with generalised tonic-clonic seizures, 12-month remission was significantly less likely in patients with myoclonic or absence seizures with tonic-clonic seizures. The HR for unclassified tonic-clonic seizures was not significant but the estimate suggests that they have a lower 12-month remission rate than generalised tonic-clonic seizures. A 12-month remission was more likely in patients randomised to start valproate than those starting lamotrigine. For total number of tonic-clonic seizures, as the number increases the chance of 12-month remission decreases. Rates of 24-month remission were as for 12-month remission with the additional conclusions that patients with absence seizures, and patients with other seizure types, were significantly less likely to achieve 24-month remission than patients with generalised tonic-clonic seizures only. The HR for unclassified tonic-clonic seizures suggests the same 24month remission rate as for generalised tonic-clonic seizures. Additionally, 24-month remission was more likely in patients randomised to start valproate than those starting topiramate.
HRs for prognostic factors for time to 12-month and time to 24-month remission
Although age is not significant, it was included in the parsimonious model for time to 12-month remission. The HRs suggest that as age increases the chance of 12-month remission also increases. Similarly, febrile seizure history was included in the parsimonious model for time to 24-month remission, with remission more likely in those with a history of febrile seizures (HR plots for both continuous variables for 12-month and tonic-clonic seizures for 24-month remission can be seen in figure 1 in the online supplementary web appendix).
Forest style plots (figures 2 and 3) illustrate the range of rates of 12-month remission predicted by the relevant model at 1, 3 and 5 years after randomisation and the range of rates of 24-month remission predicted by the relevant model at 3 and 5 years after randomisation. These results apply to patients assumed to have no neurological insult treated with valproate. Results for patients treated with lamotrigine and topiramate and also for patients assumed to have neurological insult can be seen in tables 2 to 7 and figures 2 to 11 in the online supplementary web appendix. The data show that clinical factors including seizure types and first degree relative with epilepsy have an important effect on 12- and 24-month remission rates, while the number of tonic-clonic seizures has a smaller effect.

Combination of risk factors for 12 months remission immediately, at 3 and at 5 years—patients without neurological insult treated with valproate.

{kind=link}
{kind=link}
{kind=link}
Combination of risk factors for 24 months remission by 3 and 5 years—patients without neurological insult treated with valproate.
Time to overall treatment failure
Results for the parsimonious model for overall treatment failure are shown in table 3; treatment failure is more likely if the HRs are greater than 1 (model estimates and SEs of regression coefficients can be seen in table 8 in the online supplementary web appendix). The c-statistic for the model was 0.6 which suggests that the model's internal validity is reasonable. Treatment failure was significantly more likely in patients with seizures after remission than in treatment naive patients. It was also more likely in patients taking topiramate than in patients taking valproate and patients who did not have an EEG were more likely to experience treatment failure than patients with normal EEG. Patients with absence seizures, myoclonic or absence seizures with tonic-clonic seizures, and patients with unclassified seizures were also more likely to have treatment failure than those with generalised tonic-clonic seizures only.
Multivariable model HRs for time to overall treatment failure, treatment failure because of inadequate seizure control and treatment failure because of unacceptable adverse events, by prognostic factor
Time to treatment failure due to inadequate seizure control or adverse effects
The competing risks model was forced to include the same variables as the model for overall time to treatment failure results (table 3). All four variables are significant in the model for treatment failure because of inadequate seizure control. Patients taking non-SANAD AEDs were more likely to have treatment failure than treatment naive patients and compared with patients with a normal EEG result, patients with an epileptiform EEG result had a higher rate of treatment failure because of inadequate seizure control. Similarly, compared with patients on valproate, patients on lamotrigine and topiramate had a higher rate of treatment failure due to inadequate seizure control. Treatment failure was also more likely in patients with absence seizures only, or patients with myoclonic or absence seizures with tonic-clonic seizures, than in patients with generalised tonic-clonic seizures only. Treatment history and treatment were significant for time to treatment failure because of unacceptable adverse events (table 3). Patients on topiramate were more likely to have a treatment failure due to unacceptable adverse events than patients on valproate and patients with seizures after remission were also more likely to have a treatment failure than treatment naive patients.
Discussion
What have we found?
We have shown that numerous clinical factors influence treatment outcome. For time to 12-month remission, the multivariable model included first degree relative with epilepsy, age at randomisation, neurological insult, number of tonic-clonic seizures before randomisation, seizure type and treatment. The model for time to 24month remission was similar and also included febrile seizure history. This study allowed the assessment of prognosis in a subgroup of patients who were unclassified at the point in time that treatment was started; a group for whom prognosis has not previously been estimated in this way, despite being a relatively common clinical scenario. While some of these unclassified patients will have had their epilepsy reclassified during follow-up, it is important to emphasise that these additional data should not be used in a prognostic model that is attempting to inform likely prognosis at a point in time when those data are not available. Interestingly, compared with patients with generalised tonic-clonic seizures, patients with unclassified tonic-clonic seizures had the same 24-month remission rate, but a lower but not statistically significant 12-month remission.
Our model for time to 12-month remission has a number of similarities to the prognostic model for SANAD A. The SANAD A multivariable model focused upon focal epilepsy and included variables for sex, CT/MRI scan result, treatment history, age, time from first seizure to randomisation, neurological insult, total number of seizures before randomisation, focal epilepsy site of onset and treatment. Of these, age, neurological insult, number of seizures and treatment were in common with the SANAD B model presented in this paper. The SANAD A model did not identify first degree relative as a significant factor, which is not surprising given that the generalised epilepsies are primarily genetic in aetiology, are more likely in a first degree relative, and severity of the epilepsy and hence treatment response is likely to be determined at least in part by the causal variant. The multivariable model also allows estimation of the probability of 12-month remission for patients with differing combinations of risk factors. Examples are given in figure 2 while estimates for time to 24month remission for combinations of risk factors can be seen in figure 3. While these data illustrate a higher remission rate in those allocated to initiate treatment valproate compared with lamotrigine or topiramate, the treatment effects are small. Conversely, the data show a larger effect on outcome for the clinical covariates seizure type and first degree relative with epilepsy.
It is important to emphasise that the outcome 12- or 24-month remission does not necessarily imply treatment response. We remain uncertain as to the natural history of untreated epilepsy such that in clinical practice, as in this study, for any particular patient we are unable to state with certainty that any remission is treatment induced. This is particularly so for patients with a low seizure rate prior to starting treatment for whom a long period of observation may be required to be certain of complete seizure remission. It is not surprising therefore that patients with fewer tonic-clonic seizures prior to starting treatment were more likely to achieve a 12- or 24-month remission.
For time to overall treatment failure, the best fitting multivariable model included treatment history, age at randomisation, time from first seizure to starting treatment, EEG result and treatment (table 3). Competing risks analyses provided further detail about the relationship between these factors and treatment failure. Again, the results are similar to the SANAD A model, although this model included number of seizure before randomisation rather than time from first seizure.
Strengths and weaknesses
Pragmatic trials will usually recruit a heterogeneous group of patients, and while this approach has been criticised,26 ,27 this paper illustrates the strength of this approach as it can allow an investigation of sources of heterogeneity of outcome. In this analysis of arm B, we have been able to categorise patients according to their seizure types at presentation and assess the influence of this and other factors upon treatment outcome. Some may criticise the fact that the analysis has been undertaken according to seizure type rather than epilepsy syndrome. However, it is important to highlight that abnormal EEG was not a prognostic factor for 12- or 24-month remission, and also, at the point in time that a diagnosis and a decision to start treatment are made, there is often uncertainty about the precise epilepsy syndrome, which may become clearer at a later date when further seizures have occurred or other information including investigation results are available. This is illustrated by the fact that at randomisation the most common idiopathic generalised epilepsy type specified by the randomising clinician was ‘not specified’. Nonetheless, seizure types were identified, which this analysis demonstrates are of prognostic importance. Of note, patients with generalised tonic-clonic seizures had similar 12-month remission rate to patients with absence of seizures 0.98 (0.52, 1.83), and patients with generalised tonic-clonic seizures as well as myoclonic or absence seizures had the lowest remission rate 0.56 (0.43, 0.73), as did patients with unclassified tonic-clonic seizures 0.82 (0.64, 1.06). Additionally, two individual prognostic models were developed using either patients with generalised epilepsy only or using patients with unclassified epilepsy only and both models were found to be very similar to the model published here. Given the increase in sample size and associated increase in precision of the risk estimates with the combined model, only the combined model has been presented. Other limitations of SANAD have been discussed elsewhere.11
While we have presented a number of models that can further inform patient counselling and treatment decisions, ideally these models require validation in other similar datasets and the predictive power of the model also needs to be explored. Although SANAD II is currently underway, there are no other datasets that are similar to SANAD. The closest match is a set of individual participant data collected by the authors. However, these data are missing important covariates and the treatments patients were randomised to do not always coincide with SANAD drugs. Internal validation of the models presented here does suggest a satisfactory model fit, however.
Meaning
The data presented in figures 2 and 3 show that we can recognise, at the start of antiepileptic drug treatment, groups of patients with different risks of 12 or 24month remission or treatment failure. The results also highlight how heterogeneous epilepsy outcomes are and will improve outcome prediction for patients, and allow better stratification of patients, including the identification of patients more likely to have poor treatment outcome for which more intensive follow-up may be required. Similarly the models may also aid in the identification of patients with poorer seizure control outcomes who might be eligible to participate in future trials of new treatments, for example surgical treatments such as deep brain stimulation, which might carry greater risk than drug treatment.
Unanswered questions
A number of important clinical questions remain unanswered. First, the most appropriate treatment policy is yet to be determined for women with an idiopathic generalised epilepsy who are of childbearing years. While valproate remains the most effective first-line treatment, it is also the most teratogenic. The most appropriate policy will be informed by a synthesis of data from SANAD and other randomised controlled trials and observational studies assessing the risk in pregnancy,28 ,29 and by qualitative studies that assess the priorities and preferences of women with epilepsy, an important yet under-researched area.
While clinical predictors of outcome have been identified, the way these factors influence outcome remains to be discovered. Although there is increasing interest in stratified medicine and pharmacogenetics, it remains unknown as to whether genetic factors might explain the unexplained variability in our predictive models. However, given the assumed genetic aetiology of the idiopathic generalised epilepsies, the prognostic importance of having a first degree relative with epilepsy is of great interest and raises the question as to whether some epilepsies are inherently more drug refractory,26 rather than refractoriness being expressed via another mechanism.27 Better understanding of the genetic aetiology of these epilepsies may lead to novel targets and new treatments, although the prospect of preventing the epilepsy developing in the first place remains a distant hope, likely requiring some form of gene therapy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors LJB completed all analyses, drafted and redrafted the manuscript. All other authors contributed to the drafting and redrafting of the manuscript.
-
Funding This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Grant Reference Number RP-PG-0606-1062). The views expressed are those of the author(s) and not necessarily those of the NHS, NIHR or Department of Health. The researchers are independent from the funders.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval SANAD received appropriate multicentre research committee approvals and was managed according to the Medical Research Council good clinical practice guidelines.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The SANAD team are willing to share the SANAD data with any research team that makes a reasonable request. The team are in the process of setting up an IPD repository.